
Strike the Rock
And Let Your Waters Flow.
Dr. Kevin Ham, MD
The Signal
“The gap between what medicine knows and what people are told is where 695,000 Americans die every year. I started a YouTube channel because video was the fastest way to close it.”
Caldwell Esselstyn Jr., MD. Cleveland Clinic.
Three months ago, I started a YouTube channel. My daughter graduated from film school. Talented. She had an eye for it. And I had an artist at my company who understood how to build something visually. So we started shooting.
The idea was simple. Save lives. Help people understand what disease really is and how to reverse it through lifestyle medicine. More specifically, through food and exercise. I wanted to help prevent the number one global killer from doing what it does every single year: killing 20 million people. Not in a war. Not in a pandemic. Quietly. In gyms and kitchens and bedrooms and hospital corridors. People who did not know what was building inside them until the moment it was too late to stop.
Three weeks ago, I had 1,000 subscribers.
And then one video changed everything. Then two, then three videos. Viral. People were sharing it with their loved ones. Another answered prayer.
Within a week, it had 630,000 views and counting. My channel crossed 24,000 subscribers in under two weeks. The comments came in faster than I could read them. And what struck me, what has not stopped striking me, is what people were actually asking. They were not asking about the latest drug trial or the newest surgical technique. They were asking a much simpler question—a much older one.
Watch the channel: youtube.com/@DrKevinHam
Top video: 2 Foods That Dissolve Heart Plaque
How do I stop this from killing me? How do I separate what actually works from the noise? How do I find the signal?
That is what this newsletter is. A signal. Not a wellness guide. Not a supplement list. Here is what it covers:
✓ What the science says about what builds plaque
✓ What stabilizes it before it kills you
✓ What reverses it, documented in peer-reviewed studies
✓ What dramatically reduces the chance of a heart attack, stroke, or sudden cardiac death
✓ And now I am realizing, the principles that reverse heart disease reverse all our modern diseases.
I am a doctor who became a patient. And I am telling you what I wish someone had told Rob, had told me ten years ago.
Before you read further, I want to ask you something.
Is there anyone you know who has heart disease? Who has died of a heart attack? Who has had a stroke? Who has gone blind from vascular disease?
Do you believe that when you turn 50, you will have no plaque or disease in your arteries?
How about at 60? How about at 70? Will you spend the last decades of your life in disease and suffering?
If you even thought yes, then this is for you. Educate yourself. Don’t leave your valuable the health in the hands of others.
Here is what the people watching already know. These are just 3 comments from many:
Just had an endarterectomy. Left side still 50% blocked. Starting pomegranate juice and nattokinase. Thank you Doc. @averagejoe7333
Cleared 20 to 25% of plaque in 3 months. Incredibly inspiring. Focusing on lifestyle now. @SmartWellnessTips
74 years old. Better late than never. God bless your ministry because that is what this is. @princesstoby653
The Vow
“I will give you a new heart and put a new spirit within you; I will remove the heart of stone from your flesh and give you a heart of flesh.”
Ezekiel 36:26
I was 14 years old, lying in a hospital bed, genuinely believing I was dying. My immune system had declared war on my own body. The disease was Henoch-Schönlein Purpura, an autoimmune vasculitis in which the immune system attacks the blood vessels, causing them to leak. I was a child, frightened, and in that fear, I made a vow. If God, if the universe, allowed me to survive, I would become a doctor. I would spend my life doing for others what the doctors around me were trying to do for me: finding the cause, naming the disease, fighting back against it.
I survived. I kept the vow.
Then I got busy. The vow faded from my memory as I got busy with business. And for 25 years, I tried to understand medicine, but it was more theory than truth. I stood on the physician's side of the room and believed I understood what it meant to be sick. I did not. Not really.
Then I became a patient.
When I found out that I had a CT calcium score of 505, in the worst 90th percentile for heart attack risk, and that I had coronary plaques in every vessel, I was humbled into the depths of my life—77% stenosis, 55%, 45%, everywhere. The numbers did not feel like numbers. They felt like a verdict.
Before that, the warning shockwaves: on the morning of May 10, 2020, severe wet macular degeneration announced itself in my eyes—first the right, then the left. A straight line is bent. Vision distorted—the unmistakable signature of fluid beneath the retina. I was only 50 years old. Wet AMD is a disease of the 70s and 80s. I was 20 to 30 years too early. Even if I were able to live a long life, I was told, it would likely be in blindness—no cure yet known. I was looking at a future in the dark.
I had literally a heart of stone, in my coronary arteries and in my retina. Also, in my will, blocking my understanding and my purpose. The calcified endothelium, the resistant heart, the stiffened soul: all the same condition. And I had not seen it coming.
All of a Sudden
“Create in me a clean heart, O God, and renew a right spirit within me.”
Psalm 51, written after Nathan said: you are the man
On the morning of February 10, 2025, my friend Rob Thompson, 58, a 35-year Goldman Sachs veteran, got up at dawn, made his favourite black tea, went to his home gym to train, and died on the elliptical. He was supposed to fly to Vancouver that day to see me. We had texted the night before. See you tomorrow. He had no warning, no prior cardiac event, no alarming stress test. Inside his arterial walls, an internal mountain was building, one that he did not know he had to climb, with each effort he toiled upon his heart, until that morning of February 10, on his elliptical, he fell off the cliff inside—all of a sudden.
I want to tell you who Rob was. Rob was one of the most physically disciplined people I knew. He had attempted the Matterhorn twice before. The Matterhorn. A 14,692-foot pyramid of rock and ice on the Swiss-Italian border, one of the most iconic and demanding alpine climbs in the world. To attempt it, you train for months: back-to-back mountain days carrying a 30-pound pack, 3,500 feet of elevation gain on consecutive days, cardiovascular sessions of four to six hours at sustained effort, and rock climbing in boots on technical terrain. You build to a cardiovascular fitness level that puts you in the top fraction of the population. Summit day itself starts at 4 in the morning, in the dark, from the Hörnli Hut at 10,700 feet. You climb for eight to twelve hours. The ascent is 1,200 meters of vertical, with fixed ropes on the upper section, crampons on snow and ice near the top, exposed ridges where a fall means death, and thin air that taxes even elite athletes from the first hour. Your heart rate climbs and stays there. Your legs burn with lactic acid. Your fingers ache on cold rock. The descent, on the same technical terrain, exhausted and in fading light, demands more concentration than the ascent. The mountain has killed over 500 people since its first ascent in 1865. It does not forgive a lapse.
Rob attempted it twice. Both times, the mountain turned him back. Weather. Conditions that could not be negotiated with, the kind of danger that an experienced climber recognizes and respects and retreats from. He went home. He trained harder. He prepared again. And on his third attempt, despite difficult conditions on the upper mountain, Rob Thompson summited the Matterhorn. He told me it was one of the proudest moments of his life.
This was not a man with a hidden weakness. He was brilliant, financially exceptional, and by every external measure, in superb physical condition. A man who had trained his cardiovascular system to perform at 14,000 feet in thin alpine air for twelve hours at a time. And inside his arterial walls, for forty years, a mountain of disease had been building—all of a sudden.
Rob's death reminded me of the vow. Of what I had promised to do with this life if I was allowed to keep it. This newsletter, every video I make, every data point I track in my own body, is the vow made good. It is for Rob. And it is for you.
What Medicine Knows and What Medicine Does
“We require a new yardstick to measure cardiovascular excellence. No longer will the number or quality of interventions and their temporary benefits suffice. Heart disease is a toothless paper tiger that need not exist, and if it does exist, need not progress.”
Caldwell B. Esselstyn Jr., MD. Cleveland Clinic, 2000
Here is the indictment. Rob Thompson did not die because science failed him. Rob died because none of it reached him. Not from his cardiologist. Not from his annual physical. Not from a system that tracked his LDL, prescribed him a statin, and sent him back into the world with a clean bill of health.
The gap between what medicine knows and what medicine does is where people die. Heart disease kills approximately 695,000 Americans every year. The Esselstyn protocol was first published in 1995. That is thirty years of documented reversal evidence, and it still is not the standard of care. The number of people who have died in that gap is not a rounding error. It is a generation. They were not Goldman Sachs executives who climbed the Matterhorn. They were John, your neighbour, who mowed his lawn on Saturday and did not wake up on Sunday. John had no reason to believe he was running out of time. No one had told him to look at his arterial wall. They deserved at least the option to take the simple healing remedy, rather than just management and short-term fixes.
This is not a failure of knowledge. It is a failure of transmission. The only way to close the gap is to pass the knowledge directly, person to person, outside the system that has failed to carry it. This is why I am writing this. To inform and educate. And to have people join me in my journey to climb down the mountains in my own blood vessels.
What Has Been Pressed Upon Me
“I saw it and it has been pressed upon me. And I want to press it upon you. These studies, seen over and over again, ingrained in the brain. Imprinted in the heart. Move to action.”
Kevin Ham, MD
I want to press something upon you. Not gently. With the full weight of what I have seen in the imaging, the studies, and the grief of people whose losses were preventable.
Picture a room of 100 people over the age of 50. 91 of those 100 have measurable, visible plaque in their coronary arteries right now. 91 who consider themselves generally healthy, who have been told their cholesterol is fine, 91 who do not know.
And it starts earlier than we want to believe. Korea, 1950. Army pathologist William Enos autopsied 300 soldiers, average age 22, fighting a major war:
77% had visible, gross atherosclerosis in their coronary arteries
5% had 90% or greater obstruction of at least one major coronary artery
Virtually none had symptoms or knew anything was wrong
If the bullets had not killed them, the Western diet would slowly do so decades later.
“The wall is already building. The question is only whether you know it, and what you do next.”
In 2018, researchers found the mean area of ruptured lipid-rich plaque in sudden cardiac death hearts:
0.34 square millimeters.
When I first saw my coronary CT, my low-attenuation plaque was only 0.1 percent. That number sounded reassuring. It was not. Low-attenuation plaque accounts for 70 to 90 percent of all heart attacks that result in sudden death. The SCOT-HEART trial confirmed it beats every other predictor of heart attack, including the calcium score.
5× higher risk of heart attack for patients with low-attenuation plaque burden over 4% of coronary vessel volume. This single measure outperformed every other predictor: risk scores, calcium score, and stenosis severity—all of them.
24 Patients. 12 Years. One Cardiac Event.
“We both agreed. It is so simple. Anybody can do it. Just that. No one has the mindset to do so. Not to save even their own lives, or the lives of people around them.”
Kevin Ham, MD, reflecting on his call with Dr. Esselstyn at age 92
In 1985, Dr. Caldwell Esselstyn recruited 24 patients at the Cleveland Clinic, all with severe coronary artery disease, five of them told they had less than a year to live. No exercise protocol. No sleep program. No meditation. Just a low-fat, whole food, plant-based diet for 12 years.
The result: essentially one subsequent cardiac event among adherent patients. Among the six who returned to standard care, 13 new cardiac events occurred. Thirteen. Against one. In end-stage patients who could barely walk to the end of the block.
His oldest patient was Stanley. Eighty-seven years old. His cardiologist had told him he needed bypass surgery. The surgery might kill him. He was referred to Dr. Esselstyn not in hope, but because of the absence of alternatives. He was a grandfather. He had things he still wanted to do. Stanley started the diet. Within days, he felt better. One day, he called and said, "I just wanted to thank you. I never thought I would live to be 100.
He called every year after that. This year he called at 103. He is now 11 years older than the doctor who saved his life. What do you say to a man who gave you a life you were not supposed to have? Stanley says: I just wanted you to know I am still here. And Esselstyn says: I know, Stanley. I know.
I spoke to Dr. Esselstyn on a Zoom call two weeks ago. He looked at me and said something I have not stopped thinking about since: Can you get plaque from broccoli? From arugula? From beans? You cannot. The disease comes from what we feed the endothelium. Feed it whole plants, and it heals itself. Nobody in medicine argues with the data. They just do not change what they prescribe.
I cannot unsee the images from his book, Prevent and Reverse Heart Disease. That book is the foundation of my protocol. It is the manual I wish I had been given the day of my diagnosis. I hope to one day thank him in person for reversing my extensive plaque and for helping others do the same. I pray he lives a long and blessed life. I am so grateful to him. And to God. And to my family. Blessed beyond measure.
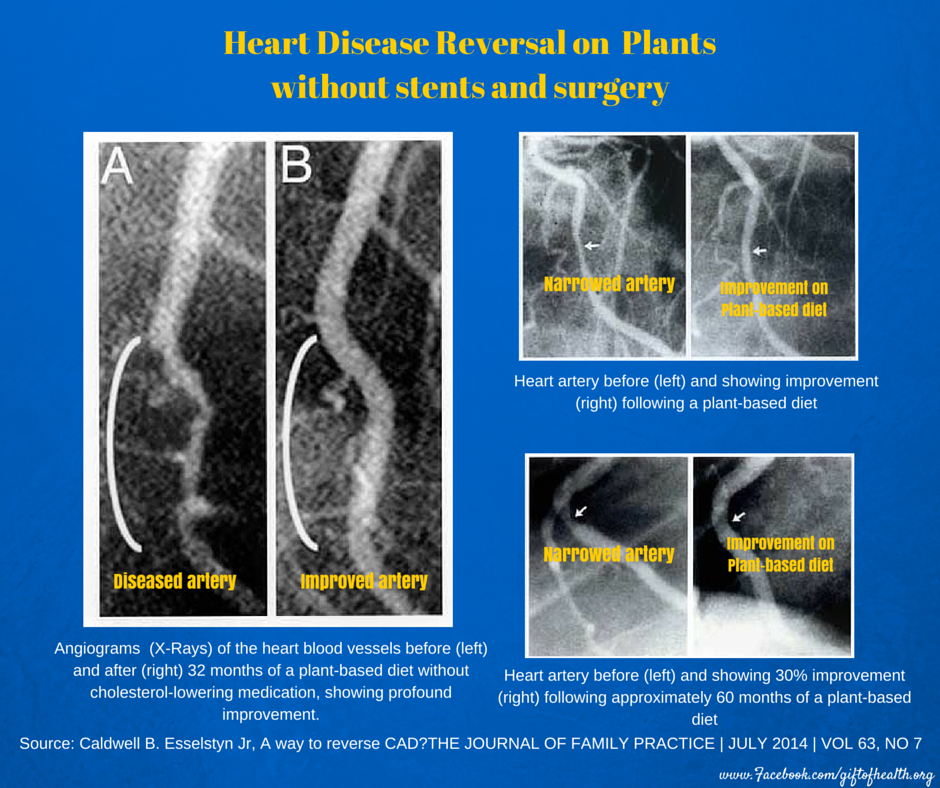
Dr. Joe Crowe: complete reversal of 100% LAD occlusion at 32 months on the Esselstyn WFPB protocol. Before and after angiogram. Cleveland Clinic. Esselstyn CB Jr. Prevent and Reverse Heart Disease. 2007.
Why It Did Not Tip
“The tipping point is that magic moment when an idea crosses a threshold, tips, and spreads like wildfire. There is a simple way to package information that, under the right circumstances, can make it irresistible. All you have to do is find it.”
Malcolm Gladwell, The Tipping Point. 2000
Here is the question that keeps me awake. William Enos published his autopsy findings on Korea in JAMA in 1953. Irrefutable data. The most respected journal in medicine. And nothing changed. Caldwell Esselstyn published his 12-year reversal data in 1999: one cardiac event among adherent patients versus thirteen among those who returned to standard care. Diet alone. And nothing changed.
Why did it take a doctor posting videos online to move 600,000 people in a week when peer-reviewed data could not move the cardiology establishment in seventy years? Because data is not sticky. Story is. Data is processed in the part of the brain that manages information. Story is processed in the part that manages identity. When you read that 91 percent of people over 50 have plaque, your brain files it. When you read about a 58-year-old man who got up at dawn, made his favourite tea, and fell off the cliff inside on his elliptical, your brain does not file it. It flinches. That flinch is the beginning of change. The Korea data had no face. Esselstyn's data did not have a YouTube channel. I am posting videos with my daughter and a gifted artist, telling you what happened to my arterial wall and what I did about it. Not more rigorous than the JAMA study. But stickier. And sticky is what saves lives.
This newsletter and these videos do not describe the tipping point. They are the tipping point. And I pray that you see that it is not only in others around you. But that it is in you. I made this grave error for 25 years. But now I know. And now you do too.
Strike the Rock
“I will stand before you there on the rock at Horeb, and you shall strike the rock, and water will come out of it, that the people may drink.”
Exodus 17:6
There is a moment in Exodus I keep returning to. The people are in the wilderness, catastrophically thirsty, no water in sight. Moses strikes a rock with his staff. Water pours out. The people drink. They live. What strikes me is not the miracle. It is the object. Not a river. A rock. The hardest thing. The most unyielding thing. And out of the rock, water.
I thought about this when I looked at my carotid images. What I had inside my arterial wall was not soft tissue. It was plaque that had hardened, visible on ultrasound, that a close physician friend described as among the worst he had seen in a 55-year-old man. When the arterial wall becomes rock, the blood cannot flow freely. The organs that depend on that flow begin to fail. The water of life is inside you. The question is whether the rock will yield it. Mine did.
The Rock Inside: What Calcification Is
“Your arteries are not passively accumulating calcium the way a kettle accumulates scale. They are actively building bone, running the same molecular program that builds your skeleton, reprogrammed by inflammation.”
Kevin Ham, MD
Atherosclerosis begins as an insult to the endothelium. LDL particles penetrate, oxidize, trigger foam cells, and build a necrotic core under a fibrous cap. When that cap tears, the clotting cascade activates instantly. This is a heart attack. Not a gradual blockage. A rupture. Calcification enters later, reprogramming smooth muscle cells into osteoblasts that deposit the same mineral as bone. Microcalcifications within the cap are volatile — stress concentrators that can trigger rupture without warning. Macrocalcifications deep in the plaque act as a stabilizing splint. This is why a rising calcium score can coexist with falling cardiac risk. They describe different stages of the same process.
The Fracture That Heals Stronger
“Before I saw my results, I thought of a broken bone. A fracture heals in six weeks, strengthens over twelve, and at the fracture point becomes even stronger than the bone that never broke. What if arterial plaque is a fracture that has never been given the conditions to heal?”
Kevin Ham, MD
The fracture point of a healed bone becomes measurably stronger than the surrounding tissue. What if arterial plaque is a fracture that has never been given the conditions to heal? Osteoclast-like cells have been detected in heavily calcified lesions. Remove the conditions driving osteoblastic transformation, and the wall can resume functioning as an arterial wall. 51 studies. 9,000+ patients. The evidence for plaque regression is now robust. The question is no longer whether it happens. It is whether you create the conditions.
And here is what reversal looks like. My carotid plaque. Gone. Remodeled. In three months. Bilateral carotid IMT of 1.8 mm and 1.6 mm with visible plaque on both sides, dropping to 0.84 mm and 0.86 mm with no visible plaque detectable on ultrasound. My CT-FFR on a dominant D1 diagonal with 77 percent stenosis: improved from 0.75 to 0.80, crossing from ischemic into the normal range. LDL: 61, a 64 percent reduction. ApoB: 45. The word my physician friends used: Unbelievable!
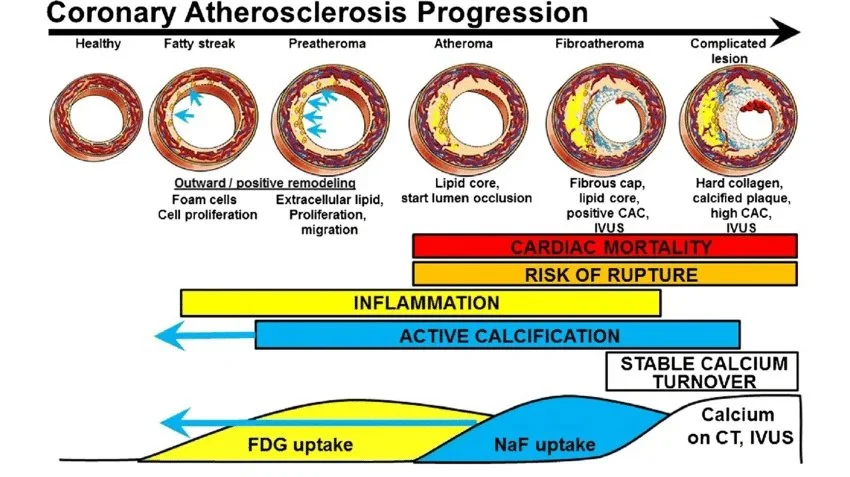
The six types of atherosclerotic plaque and their progression. My plaque is in stages 4 to 6. The later the stage, the more difficult to reverse. But not impossible. European Journal of Nuclear Medicine and Molecular Imaging, November 2018.
The Fracture That Heals Stronger
“Before I saw my results, I thought of a broken bone. A fracture heals in six weeks, strengthens over twelve, and at the fracture point becomes even stronger than the bone that never broke. What if arterial plaque is a fracture that has never been given the conditions to heal?”
Kevin Ham, MD
The fracture point of a healed bone becomes measurably stronger than the surrounding tissue. What if arterial plaque is a fracture that has never been given the conditions to heal? Osteoclast-like cells have been detected in heavily calcified lesions. Remove the conditions driving osteoblastic transformation and the wall can begin to function as arterial wall again. 51 studies. 9,000+ patients. The evidence for plaque regression is now robust. The question is no longer whether it happens. It is whether you create the conditions.
And here is what reversal looks like. My carotid plaque. Gone. Remodeled. In three months. Bilateral carotid IMT of 1.8 mm and 1.6 mm with visible plaque on both sides, dropping to 0.84 mm and 0.86 mm with no visible plaque detectable on ultrasound. My CT-FFR on a dominant D1 diagonal with 77 percent stenosis: improved from 0.75 to 0.80, crossing from ischemic into the normal range. LDL: 61, a 64 percent reduction. ApoB: 45. The word my physician friends used: Unbelievable!
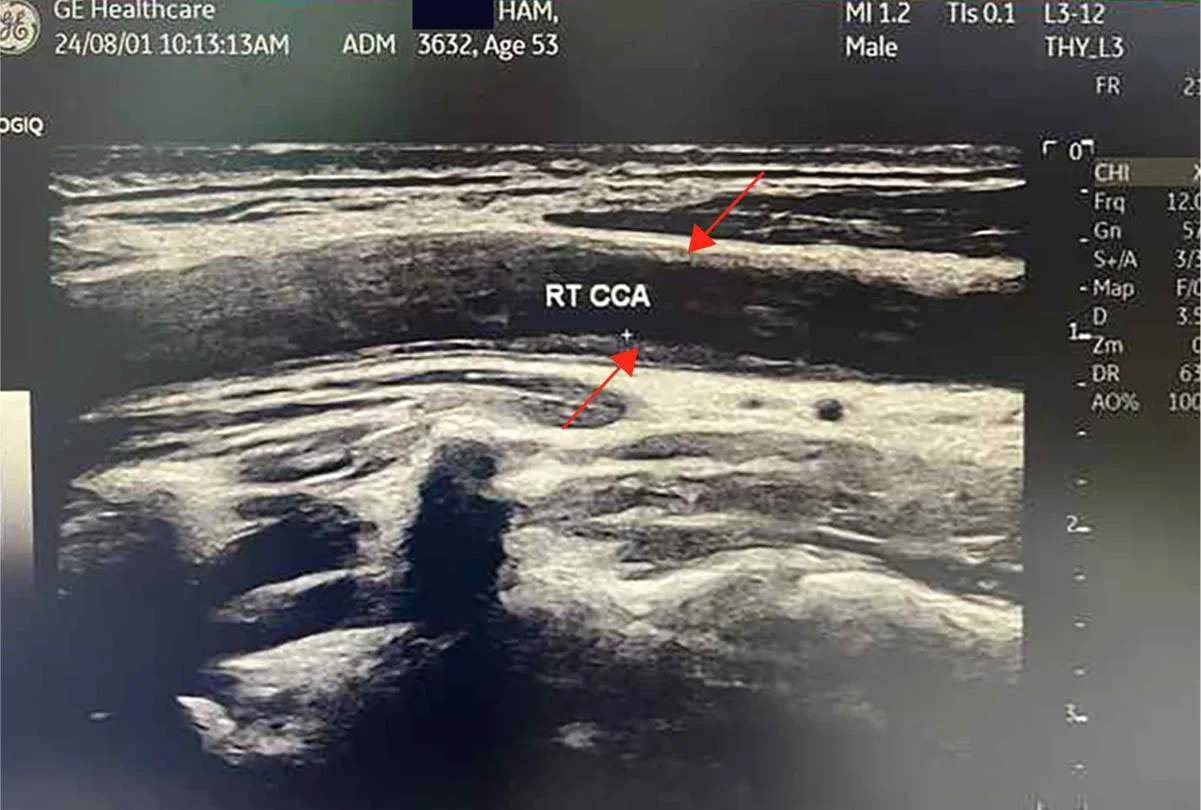
Before: RT CCA . Longitudinal . Baseline

Before: LT CCA . Longitudinal . Baseline
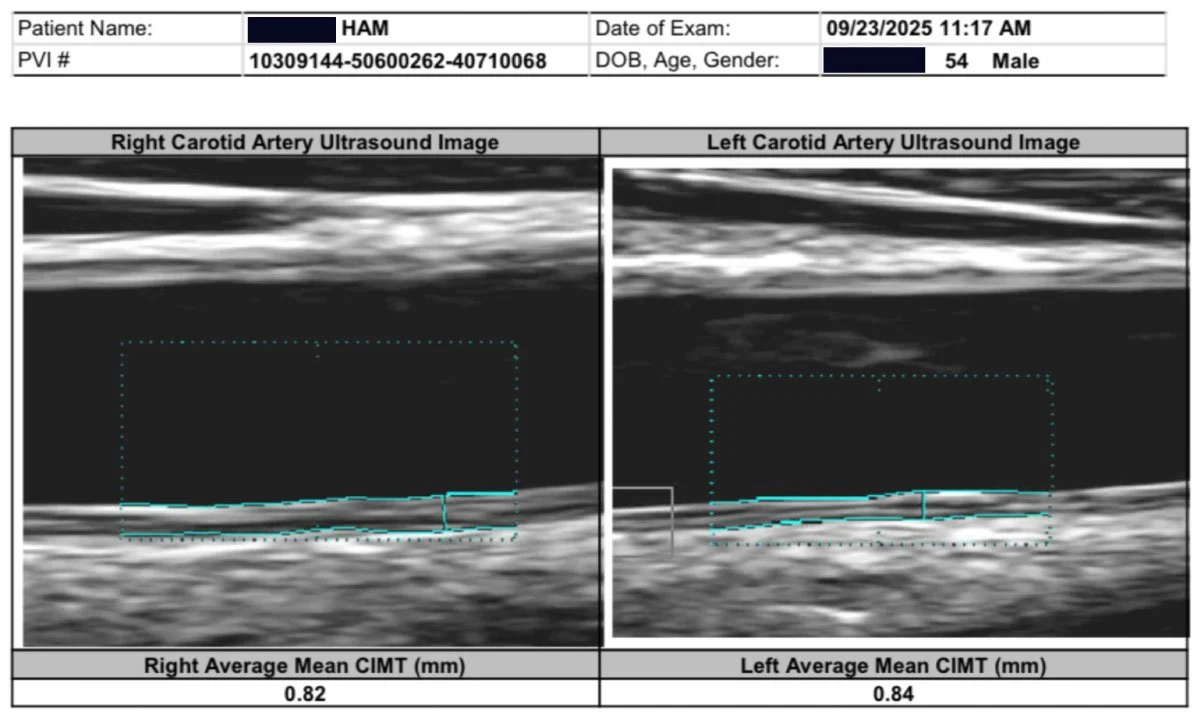
After: Plaque remodeling and reversal. B-mode ultrasound imaging of the carotid artery. Kevin Ham, MD, 2025. Three months on the CAST protocol: WFPB diet, high-intensity cycling, structured fasting, targeted supplementation.
The CAST Protocol
“Cast by removing the causes. Add the healers. Support and strengthen. Track and measure. Stop the damage, add what heals, strengthen the blood vessels, and track the results.”
Kevin Ham, MD
Four moves, in order. One sentence: stop the damage by removing the causes, add what heals, strengthen the blood vessels, and track the results.
C: Cast by Removing the Causes. Like a cast on a broken bone. Fractured arteries. Fractured endothelium. Fractured retina. Fractured health. Before any healing element can work, you must first stop the damage: processed food, oxidized lipids, sedentary life, and chronic stress. Cast it first, hold it still, and let the body begin its work.
A: Add the Healers. Healing foods that generate nitric oxide and reverse endothelial dysfunction. High-intensity exercise that drives macrophages toward the anti-inflammatory M2 phenotype. Fasting that activates autophagy and resets the immune system. These are not supplements to an otherwise unchanged life. They are the intervention.
S: Support and Strengthen. Build the three pillars as permanent lifestyle habits:
Diet. The Esselstyn whole food plant-based protocol. Total fat below 25 grams daily. No oils. No animal products. Greens six times a day, chewed thoroughly so the nitrates convert to nitric oxide, the molecule that protects your endothelium around the clock. Nattokinase at 6,000 FU. Aged garlic at 2,000 milligrams. Pomegranate juice. Curcumin. Spirulina. Algae-sourced EPA and DHA. Balsamic vinegar. A medicine cabinet made of food.
Exercise. HIIT: High Intensity Interval Training. Out-of-breath pace for 30 seconds to four minutes, then recover for 4 minutes. Repeat 1 to 4 times. Walk fast, jog, run, cycle, swim, squats, or jump rope. Whatever gets your heart rate up and blood flowing with good sheer force. This is nitric oxide-producing, artery-protecting exercise. Think of it as a good pressure wash for your arteries. High-intensity aerobic effort quiets the inflammatory fire inside the arterial wall. This is one of the most powerful prescriptions I have ever written.
Fasting. I fast to activate what 300,000 years of evolutionary biology encoded in every cell. Autophagy dismantles damaged cellular machinery. Extended fasting triggers hematopoietic stem cell activation, which gives rise to immune system precursors. My protocol: daily 16:8, one OMAD day per week, one extended fast of two to three days per month. Not asceticism. Seasonality. The ancient rhythm, reclaimed deliberately.
T: Track and Measure. Carotid IMT, CT-FFR, and coronary CT angiogram every six months. Lipid profile and metabolic profile every 30 to 45 days until you hit your targets, then every quarter. Without measurement, you are making changes into the void. Every image is a report from the front line.
Diet. Exercise. Fasting. The Ancient Flywheel.
“I am not fasting to lose weight. I am fasting to activate an ancient system of survival in our bodies. Autophagy. Stem cells. Immune cells reset. Regeneration. The power of our famine and feast seasonality.”
Kevin Ham, MD
I finally understand. Once I understood heart disease, I finally understood my eye disease. And almost all of the modern diseases of our civilization today. Including, I believe, an elementary understanding of how to begin dealing with cancer, understood as a metabolic and vascular disease with the same upstream roots.
These three levers, diet, exercise, and fasting, are not a wellness routine. They are a biological intervention targeting the upstream causes of the number one killer on earth. The protocol in the section above tells you what to take. These three pillars tell you how to live.
“The three together are not additive. They are multiplicative. A force multiplier. A flywheel that, once set in motion, compounds on itself.”
One Disease. Many Organs. One Protocol.
“I was surprised all of a sudden with wet macular degeneration. To me they are the same disease, just different organs. I am reversing both, so help me God.”
Kevin Ham, MD
I am the doctor who became the patient. And because I became the patient, I began to see what I could not see from the other side of the room.
I was diagnosed with severe wet macular degeneration in both eyes on the morning of May 10, 2020. I was only 50 years old. It announced itself suddenly: a straight line bent, vision distorted, fluid beneath the retina. Wet AMD is a disease of the 70s and 80s. I was 20 to 30 years too young for this diagnosis. Even if I lived a long life, I was told it would likely be in blindness—no cure yet known. And no one could explain why it had arrived so early. But I could. When I looked at the biology, I saw the same driving mechanism as coronary artery disease: endothelial dysfunction in the microvasculature. The same inflammatory cascade. The same oxidized lipid injury. The same nitric oxide deficiency. The retina was simply the first organ that made the disease visible. My arteries had been telling the same story for years. It is the same disease presenting in a different organ.
Wet macular degeneration. Coronary artery disease. Type 2 diabetes. Hypertension. Non-alcoholic fatty liver disease. And I believe, in due time, certain autoimmune diseases. Cancer is understood as a metabolic disease.
These are not separate diseases coexisting in the same aging body. They are expressions of one underlying condition: chronic metabolic inflammation driving endothelial dysfunction across different organ systems. Medicine treats each in a separate department, with a different specialist, and a different drug. But the root is the same root. And if the root is the same, the protocol that addresses the root addresses them all.
Circumcise Your Heart
“Circumcise yourselves to the LORD; remove the foreskin of your heart.”
Jeremiah 4:4
The command to circumcise the heart runs through Scripture like a surgical instruction. In Ezekiel 36, God promises not merely to command this change but to perform it: I will remove the heart of stone from your flesh and give you a heart of flesh. The surgery is divine. The rock does not yield on its own. It requires an instrument applied from outside the system. The same is true in biology.
The circumcision of the heart is the cutting away of what covers and hardens the living tissue underneath. The removal of the calcified layer of habit and assumption that prevents the blood of grace from flowing freely. In both dimensions, spiritual and biological, the grammar is identical: remove the cause, restore the inhibitors, allow the program of reversal to run. What was rock yields water. What was rigid becomes responsive. What was closed becomes open to flow.
Strike the rock.
“I will give you a new heart and put a new spirit within you; I will remove the heart of stone from your flesh and give you a heart of flesh.”
Ezekiel 36:26
Your Questions
Questions worth sitting with.
One action. In the next 24 hours, book a CT calcium score or a Carotid IMT ultrasound. Call your doctor today and ask for it by name. That single image will tell you more about your arterial health than every blood test you have ever had.
1. Is there someone in your life whose sudden death you would not recover from? Do they know what is building inside their arterial wall?
Rob Thompson's wife stood at his memorial and said: he had a stress test every day. Every workout, every climb. He passed everyone. And then he died. She asked every person in that room to get a CT calcium score. You can give someone you love the gift that Rob's wife was never able to give Rob. Send them this. Ten seconds
2. If 91 percent of people over 50 have measurable plaque right now, and most of them have never been told, what are the odds that you are the exception?
You are probably not the exception. Neither was Rob. Neither was I. The imaging that would tell you the truth about your arterial wall takes 30 minutes and is available in most cities. The question is not whether you can afford to find out. The question is whether you can afford not to.
3. When is the last time you ate a meal that was designed to heal your endothelium rather than injure it?
Every meal is a vote: either for the endothelium that keeps plaque from starting, or against it. Dr. Esselstyn kept the worst heart patients alive for 12 years with just diet. No surgery. No procedure. No prescription. Just food chosen deliberately. That power is available to you at the next meal.
4. If your body has the biological machinery to reverse this, what is the one thing you are willing to change today to let it begin?
Not everything. Just one thing. Today. I started the whole food plant-based diet on May 9, 2025, the morning after I saw my calcium score of 505. Within three months, my carotid plaque was gone. One meal in the right direction is the beginning of fracture healing. Start there.
Someone You Love
“The greatest single threat to the cardiac health of each individual is his own coronary arteries. And the greatest threat is not that we lack the knowledge to prevent the disease. It is that we lack the will to act on what we already know.”
Paul Dudley White, MD Presidential physician, founder of the American Heart Association, 1956
You thought of someone while reading this. Their name came to you. Maybe it is the person who has never had arterial imaging. Maybe it is the one who was told their cholesterol is fine and sent home with nothing else. Maybe it is you. Rob Thompson passed every stress test he ever took. His LDL was normal. And on February 10, 2025, he died of a process that had been building for forty years inside a wall that no standard test was looking at. The gift Rob's wife never got to give him takes ten seconds to send.
This is my ministry. This is my gospel of your heart.Send this to the person you thought of. Better late than never.
Strike the rock. I pray that the rock yields its waters for you.
MORE READINGS YOU’LL ENJOY
Health
Watch: The 2 Foods That Reverse Heart Plaque (Half a Million Views)
Reversing My 77% Heart Plaques
Stats Say You Likely Have Heart Plaque
The Healing Power of Food: Nitric Oxide
Wealth
The Power of the Compound Effect
Relentless Iteration to Mastery
Meaning
The Courage to Your Magnum Opus
APPENDIX
The ten studies that anchor the science in this newsletter.
1. Esselstyn CB Jr, et al. A Strategy to Arrest and Reverse Coronary Artery Disease: A 5-Year Longitudinal Study. J Fam Pract. 1995;41:560-568.
The foundational study. Severe coronary disease arrested and reversed in human patients through plant-based diet alone. The study medicine still does not know what to do with.
"Heart disease isn't some great mystery. We are empowered to take control of it. Patients are often furious that they were not made aware of this option earlier." — Caldwell B. Esselstyn Jr., MD
2. Esselstyn CB Jr. Updating a 12-Year Experience With Arrest and Reversal Therapy for Coronary Heart Disease. Am J Cardiol. 1999;84:339-341.
Twelve-year follow-up of the original 24-patient cohort: one cardiac event among adherent patients versus thirteen among those who returned to standard care.
"Coronary artery disease need not exist, and if it does exist, it need not progress. We have documented not merely the arrest but the reversal of this disease in human beings." — Caldwell B. Esselstyn Jr., MD
3. Ihle-Hansen H, et al. Prevalence of Carotid Plaque in a 63 to 65-Year-Old Norwegian Cohort: The ACE 1950 Study. J Am Heart Assoc. 2018;7:e008562.
Carotid ultrasound of 3,683 generally healthy adults: plaque in 87 percent overall, 92 percent of men. The 91 percent figure cited in this newsletter.
"Atherosclerotic carotid plaques were present in 87% of the participants. The carotid plaque score was more strongly associated with incident ischemic stroke than established cardiovascular risk scores." — Ihle-Hansen H, et al.
4. Enos WF, Holmes RH, Beyer J. Coronary disease among United States soldiers killed in action in Korea. JAMA. 1953;158:912-914.
Autopsies of 300 soldiers, average age 22. Gross atherosclerosis in 77.3 percent. The study that should have tipped in 1953 and did not.
"Gross evidence of coronary arteriosclerosis was found in 77.3 percent of 300 American soldiers killed in Korea, average age 22. It is no wonder that at the time of death the process was far advanced." — Enos WF, Holmes RH, Beyer J.
5. Han D, Torii S, et al. Quantitative measurement of lipid rich plaque: correlation of histology in sudden cardiac death. Atherosclerosis. 2018;275:426-433.
Post-mortem CT correlation with histology in sudden cardiac death hearts: mean ruptured lipid-rich plaque area of 0.34 square millimeters. A whisper of tissue. Sufficient to kill.
"Mean lipid-rich plaque area per coronary cross-section in sudden cardiac death hearts: 0.34 square millimeters. A whisper of vulnerable tissue sufficient to kill." — Han D, Torii S, et al.
6. Williams MC, et al. Low-Attenuation Noncalcified Plaque Predicts Myocardial Infarction: SCOT-HEART Trial. Circulation. 2020;141:1452-1462.
1,769 patients followed for nearly five years. Low-attenuation plaque burden outperformed every other predictor of heart attack: better than calcium score, risk scores, and stenosis severity combined.
"An increased burden of low-attenuation plaque is the principal predictor of increased coronary events, above and beyond other established classic markers of cardiovascular risk." — Williams MC, et al.
7. Schurgers LJ, Cranenburg ECM, Vermeer C. Matrix Gla-protein: the calcification inhibitor in need of vitamin K. Thromb Haemost. 2008;100:593-603.
Established Matrix Gla Protein, activated by vitamin K2, as the dominant inhibitor of arterial calcification. High vitamin K intake not only prevents but regresses existing vascular calcium.
"There seems to be no effective alternative mechanism for calcification inhibition in the vasculature. High vitamin K intake not only prevents calcification, but even regresses arterial calcifications." — Leon J. Schurgers, PhD
8. Xu Z, et al. Osteoclastogenesis and Osteoblastogenesis in Vascular Calcification. Front Cardiovasc Med. 2021;8:639740.
Demonstrated that arterial calcification is reversible: osteoclast-like cells can resorb mineral from the arterial wall, establishing the cellular basis for the reversal documented in this newsletter.
"Arterial calcification is a cell-mediated, reversible and actively regulated process. Tilting the balance toward osteoclast-like cells may be a promising therapeutic strategy." — Xu Z, et al.
9. Banach M, et al. Atherosclerotic coronary plaque regression from lipid-lowering therapies: a meta-analysis. Atherosclerosis Plus. 2024.
Meta-analysis of 51 studies and 9,113 patients. Plaque regression is real, reproducible, and documented. The question is no longer whether it happens. It is how aggressively we pursue it.
"The evidence for plaque regression is now robust. The question is no longer whether plaque regresses, but how aggressively we pursue the conditions that allow it." — Banach M, et al.
10. Longo VD, Mattson MP. Fasting: molecular mechanisms and clinical applications. Cell Metab. 2014;19:181-192.
The molecular mechanism review behind the fasting component of the CAST protocol: autophagy, apoptosis of damaged cells, and stem cell activation. The most extensive cellular renewal process available to the human body.
"During prolonged fasting, the body survives by eliminating unnecessary cells. These cells will be replaced when food becomes available. This regeneration process, the most extensive since birth, is a powerful feature of prolonged fasting." — Valter D. Longo, PhD
I pray you unlock your heart to reach the height of your full potential by discovering your calling.
Kevin Ham, MD
Subscribe to my Compounding Wisdom newsletter and start transforming your life. ham.com
Subscribe to my YouTube channel @DrKevinHamfor videos on how I reversed my clogged arteries in 3 months, the top foods that clear your arteries, and the first principles of health that can save your life. Like, share and subscribe — it could save the life of someone you love.