
Reversing the Disease Flywheel
First Principles on Reversing the Biology of Disease
Dr. Kevin Ham, MD
The Architecture of a Cure
“Some people think that the plant-based, whole foods diet is extreme. Half a million people a year will have their chests opened up and a vein taken from their leg and sewn onto their coronary artery. Some people would call that extreme.”
Caldwell Esselstyn Jr., MD. Cleveland Clinic.
I am a physician turned entrepreneur. Twenty-five years of building companies taught me mental models that have nothing to do with balance sheets and everything to do with how complex systems actually work. When my heart scan came back, I did what I always do when I do not know something. I studied. I studied the data, the mechanistic pathways, the constraints and the 80/20 levers. And I applied the same four principles to heart disease that I have used in business. This is the methodology behind my results.
Principle 1: The Flywheel
“The flywheel effect is not the result of one defining action, one grand program, one killer innovation, one solitary lucky break. It comes from the cumulative effect of pushing the flywheel forward, turn after turn, building momentum until a point of breakthrough and beyond.”
Jim Collins. Good to Great.
A flywheel is a rotating mass that stores momentum. In physics, it is the heavy disc on an engine that keeps the crankshaft turning smoothly between combustion strokes. The critical property of a flywheel is this: it resists change in both directions. It is hard to accelerate from rest. But once it is spinning, it is equally hard to stop.
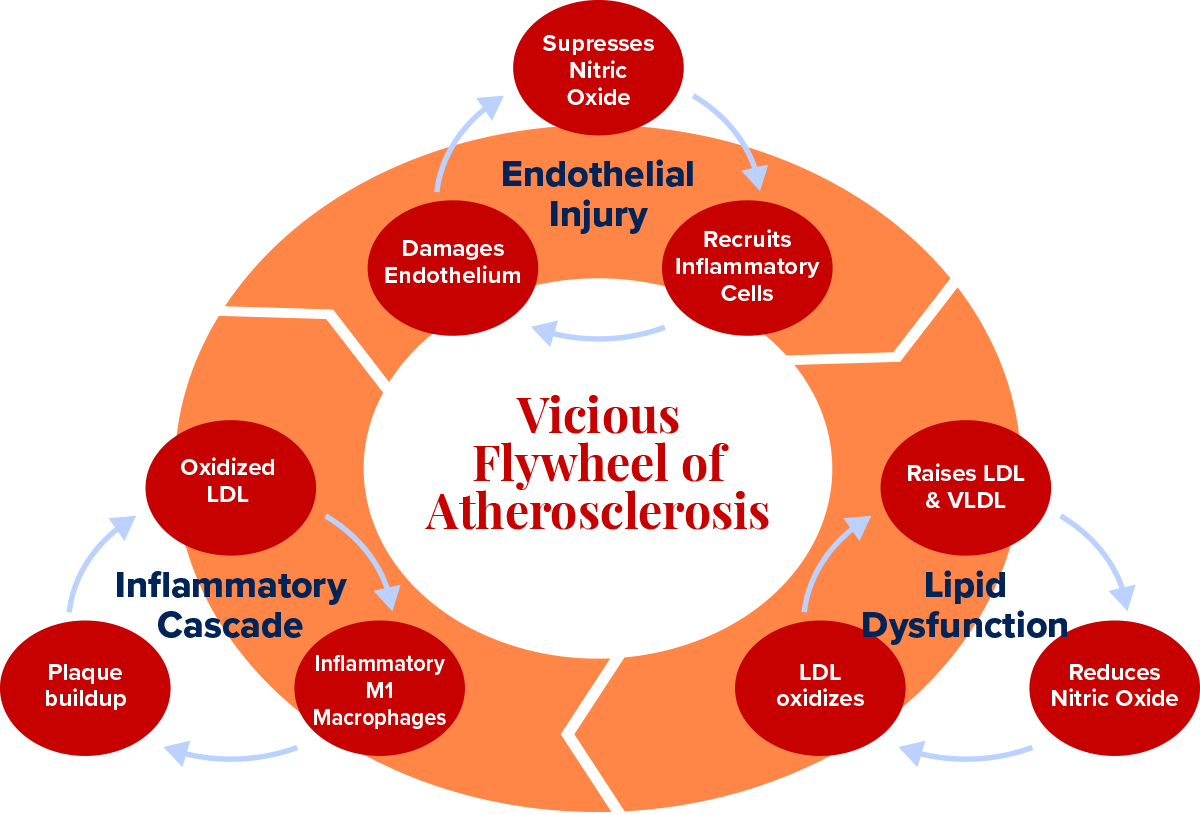
Disease is a flywheel. Not a sudden event. Not bad luck. A self-reinforcing vicious cycle that builds speed over the course of many years, each revolution making the next one faster and harder to interrupt. Endothelial damage invites oxidized LDL. Oxidized LDL triggers inflammation. Inflammation damages the endothelium further. The cycle closes, tightens, and accelerates. This is the vicious flywheel, running in the dark for decades before it announces itself.
Health is also a flywheel, turning in the right direction. A healthy endothelium produces nitric oxide. Nitric oxide blocks LDL oxidation and suppresses the adhesion molecules that recruit inflammatory cells. With less inflammation, the endothelium can repair itself. A repaired endothelium produces more nitric oxide. Each revolution reinforces the next. This is the virtuous flywheel.
The central question of my protocol is not: what supplements should I take? It is: how do I stop the vicious flywheel and start the virtuous one? Because the biology of the flywheel tells you something important. You do not need to fix everything simultaneously. You need sufficient force, applied at the right entry point, and the system will do the rest. Get the flywheel turning in the right direction, and it gains its own momentum.
Principle 2: The Judo Strategy
“The goal of judo is not to defeat your opponent. It is to understand the principles of life itself. Maximum efficiency with minimum effort. Mutual welfare and benefit. Yield to win.”
Jigoro Kano. Founder of Kodokan Judo. 1882.
In judo, strength is irrelevant. The principle is leverage: you use your opponent’s own force against them. When they push, you pull in the same direction, adding your force to theirs, and suddenly their own momentum carries them off balance. Then you use your body as a lever, redirect the energy, and throw them with a fraction of the effort it would take in a direct confrontation. When they pull, you push, and the same geometry applies. The opponent’s strength becomes your weapon.
I apply this to disease with one question: what forces is the disease already using, and how do I redirect them? In atherosclerosis, the immune system recruits macrophages into the arterial wall to clear oxidized LDL. In a chronically inflamed environment, those macrophages become overloaded, switch to a destructive M1 phenotype, and begin releasing enzymes that digest the fibrous cap of existing plaque from within. The very system designed to protect you is now accelerating your destruction.
The judo move is not to suppress the immune system. It is to shift the macrophage phenotype from M1 to M2, from inflammatory to healing, so that the same cells that were building disease begin participating in its reversal. Polyphenols, exercise, and fasting all apply force at this exact switch. You are not fighting your immune system. You are redirecting it. The opposition’s strength becomes your treatment.
Principle 3: The Fractal 80/20
“The 80/20 principle says that a minority of causes, inputs or effort usually leads to a majority of results, outputs or rewards. Taken to its logical conclusion, it means that a great deal of what we do is of low value and a little of what we do is of high value. The more we can concentrate on the high-value activities, the more effective we become.”
Richard Koch. The 80/20 Principle.
Vilfredo Pareto noticed in 1896 that 20 percent of the peapods in his garden produced 80 percent of the peas. The same ratio appeared in land ownership across Italy. Economists found it in income distribution. Engineers found it in software defects. Athletes find it in training adaptation. The specific numbers vary. The underlying principle does not: inputs are not created equal. A small number of causes drive the vast majority of effects.
In medicine, this means that among the hundreds of factors that might contribute to your cardiovascular disease, roughly 20 are responsible for 80 percent of what is happening. The other 80 contribute the remaining 20 percent. If you pursue all of them with equal effort, you are dramatically misallocating your time and energy. The 80/20 principle is not an excuse for laziness. It is a demand for precision. Find the 20 that matter most and address those first.
But here is where it becomes remarkable, and where most people stop too soon: the 80/20 principle is fractal. It repeats inside itself, at every level of magnification, like a coastline that shows the same jagged complexity whether you view it from a satellite or from a clifftop or from your knees in the sand.
Take those top 20 factors, the ones producing 80 percent of your disease. Apply the 80/20 lens to that group alone. Twenty percent of those 20 factors, which is 4 factors, will produce 80 percent of that 80 percent of results. Run the arithmetic: 4 things account for 64 percent of your total disease burden. You have gone from 100 inputs to 4 and captured nearly two-thirds of the problem.
Apply the fractal one more time. Of those 4 high-leverage factors, one accounts for 80 percent of that 64 percent. Which means: one single factor accounts for roughly 51 percent of the total. One thing. Half the problem. If you can identify it and remove it, you have done more than any other single intervention could possibly achieve. This is not a shortcut. It is the highest form of strategic thinking: the relentless reduction of complexity until the single most powerful lever is visible.
In cardiovascular disease, that one thing is endothelial dysfunction. The endothelium is the initiating event. It is the gate that, when compromised, lets the Trojan horse through. It is the surface that, when inflamed, becomes a magnet for plaque formation. It is the organ that, when healthy, produces nitric oxide, which prevents nearly every downstream step in the cascade.
Heal the endothelium, and you have addressed 51 percent of the disease through a single biological mechanism. Every other intervention in my protocol is downstream of this one.
Find the one thing.
In disease: it is the cause. Remove the cause and you remove half the disease.
In health: it is the highest-leverage intervention. Find it and you gain half the results.
The fractal 80/20 is not a formula. It is a philosophy of precision.
Principle 4: The Theory of Constraints
“An hour lost at a bottleneck is an hour lost for the entire system. An hour saved at a non-bottleneck is a mirage. It saves nothing. It changes nothing. Only the constraint matters.”
Eliyahu Goldratt, PhD. The Goal.
Eliyahu Goldratt introduced this framework in manufacturing. Every production system has a bottleneck, a single point that limits the throughput of the entire process more than any other. You can optimize every other step to perfection, but if the bottleneck remains, overall output does not improve. The constraint governs everything. The only productive action is to find it, elevate it, and then look for the next constraint.
In cardiovascular disease, the bottleneck is blood flow. Specifically, its interruption. Heart attacks occur when a clot or a ruptured plaque causes sudden, complete obstruction of a coronary artery. Strokes occur when the same happens in cerebral circulation or when a vessel ruptures. The common thread is not the size of the blockage. It is the stability of the plaque and the thrombogenicity of its contents. A 90 percent stenosis with a thick fibrous cap and a quiescent inflammatory environment may never rupture. A 30 percent stenosis with a thin cap and an activated immune infiltrate can kill you on a Tuesday morning.
The constraint in heart disease is not cholesterol. It is not even stenosis percentage. The constraint is the biology that makes a plaque vulnerable to rupture: inflammation, a thin fibrous cap, a large necrotic core, and the matrix metalloproteinases produced by M1 macrophages that digest the cap from within. Remove that constraint, and you remove the mechanism of the acute event, regardless of what is on your lipid panel.
These four principles are not independent ideas. They are a single system of thought.
The flywheel gives you the architecture of disease and health.
The judo strategy tells you how to redirect the disease’s own forces.
The fractal 80/20 tells you where to apply force first.
The theory of constraints tells you what to remove.
Together, they produced my protocol. And together they produced my results.
“Atherosclerosis is not a lipid storage disease. It is a chronic inflammatory disease of the arterial wall, initiated by injury to the endothelium.”
“Atherosclerosis is not a lipid storage disease. It is a chronic inflammatory disease of the arterial wall, initiated by injury to the endothelium.”
Russell Ross, MD. University of Washington. New England Journal of Medicine, 1999.
Your Blood Vessel Wall is Already Burning
“The lesion of atherosclerosis is the most common cause of death in Western societies. It is also, in principle, preventable. It begins not with cholesterol, but with injury. Remove the injury and you remove the disease.”
Russell Ross. New England Journal of Medicine, 1999.
Most people, when they think about heart disease, think about cholesterol. But cholesterol is an ingredient of plaque, not the cause. Think of the arterial wall as a fortified city. The endothelium is the city wall, the sentinel layer. If the wall is intact, the city is defended. When it is damaged, the Trojan horse gets through.
The man who proved this was Russell Ross, a pathologist at the University of Washington, working in 1973 on what most of his colleagues considered a settled question. Atherosclerosis, the prevailing view held, was essentially a passive process: cholesterol circulating in excess would simply seep through vessel walls and accumulate, like sediment settling at the bottom of a river. Ross did not believe it. He had been studying platelet-derived growth factor and noticed something that did not fit the sediment theory: the arterial lesions he was examining looked less like passive deposits and more like wound responses. The tissue was reacting. The wall was responding to something.
He published what he called the ‘response to injury’ hypothesis in 1973 and expanded it through two subsequent decades of work. The injury he meant was not a cut or a bruise. It was a molecular insult to the endothelium: the inner lining of the blood vessel, a structure so thin it had largely been treated as irrelevant scaffolding. Ross proposed that this single-cell layer was not passive scaffolding at all. It was an active, signalling, immunological frontier. Damage it, and you initiate a cascade that looks far more like chronic inflammation than passive lipid deposition. The medical establishment received this idea with the same generous skepticism it reserves for all ideas that require reconsidering everything. But Ross was right. And the cascade he described is the vicious flywheel.
The Trojan horse is LDL cholesterol. Once inside the damaged wall, LDL can oxidize. Oxidized LDL is a danger signal that summons the immune system. Monocytes flood in and become macrophages, tasked with cleaning up the mess. But in a chronically inflamed environment, they become overwhelmed. They shift to the M1 inflammatory phenotype, releasing cytokines that further damage the endothelium, allowing more LDL through, driving more oxidation, and recruiting more monocytes. The macrophages die, full of lipids, forming foam cells and the necrotic core of the growing plaque. And the cycle accelerates.
This flywheel runs on three pillars, each driving the next. Endothelial damage is where it begins:
saturated fat suppresses eNOS within hours of consumption,
hypertension shears the vessel wall at arterial branch points, and
oxidative stress depletes the antioxidant defences that protect the inner lining.
When the wall fails, LDL slips through. Once inside, in the changed chemical environment of the subendothelial space, it oxidizes. Oxidized LDL is a danger signal. It summons the immune system.
That summoning is the second pillar: chronic inflammation.
Monocytes migrate into the wall and become macrophages, tasked with neutralizing the oxidized LDL. In an acute situation, this works. In a chronic one, it fails catastrophically. The macrophages become overwhelmed, switch to the M1 inflammatory phenotype, and begin releasing cytokines, IL-6, TNF-alpha, and matrix metalloproteinases that dissolve the fibrous cap protecting the growing plaque from the bloodstream. They recruit more monocytes. More monocytes damage the endothelium further. The gate opens wider.
The third pillar is atherogenic lipoproteins, and the most important measure here is not LDL cholesterol but ApoB: one molecule per particle, present on every atherogenic lipoprotein in circulation, a direct count of the Trojan horses circling the arterial wall.
Saturated fat downregulates the hepatic receptors that clear these particles.
Insulin resistance drives the liver to overproduce VLDL.
The oxidized form of these particles, once inside the inflamed wall, is the direct trigger of the foam cell cascade that forms the necrotic core of plaque.
The most dangerous heart attack is not caused by the most obstructed artery. This shattered my prior intuition. The most dangerous lesion is a vulnerable plaque: a small to medium deposit with a large necrotic core, a thin fibrous cap, and a crown of activated M1 macrophages digesting the cap from within. When that cap ruptures, the contents contact circulating blood and trigger the explosive thrombosis that produces a heart attack within minutes. The most dangerous plaques are the most inflamed, not the largest.
The disease has been running its program for forty years. The flywheel is already spinning. The question is not whether it has started. The question is whether you will stop it.
“Our genes are not our fate. Even older adults with severe coronary artery disease can begin to reverse it. Not slow it. Reverse it. Within weeks, most patients feel so much better, so quickly, that these new behaviours become sustainable.”
Dean Ornish, MD. Lifestyle Heart Trial. The Lancet, 1990.
The Disease that Reverses
“Joy is a more powerful motivator than fear. In my experience, most people don't want to be told what to stop doing. They want to be told what they can start doing that will make them feel better right away.”
Dean Ornish’ Program for Reversing Heart Disease, 1990.
In the late 1980s, a young physician named Dean Ornish proposed something that the cardiological establishment found almost impolite. He wanted to know whether coronary artery disease could be reversed, not slowed, not stabilized, but actually reversed, through diet, exercise, stress management, and group support alone. No drugs. No surgery. No stents. The proposal drew skepticism that ranged from condescension to amusement. Coronary artery disease was a one-way street. Everyone knew that. Ornish apparently did not.
He ran the Lifestyle Heart Trial anyway. Twenty-eight patients with documented coronary artery disease were randomized to his intensive program. Twenty patients served as controls. Coronary angiography was performed at baseline and at one year, measuring the actual diameter of the coronary arteries, the same vessels in which plaque had been growing for decades. The results, published in The Lancet in 1990, were unambiguous: in the treatment group, arteries had grown wider. In the control group, following standard American Heart Association guidelines, they had continued to narrow. At five years, the divergence had increased. The patients who had reversed their disease most completely were the ones who had followed the protocol most strictly. The lifestyle intervention was dose-dependent, like a drug, except it had no patent and no sales force and required no prescription.
The medical community acknowledged the data and largely declined to change its practice. The mechanisms were not yet understood. The trial was small. The diet was extreme. These were the arguments. What they amounted to was: we believe you, but we are not ready to believe you. What Ornish had found, though neither he nor his contemporaries could fully name it in 1990, was the virtuous flywheel. Apply enough force at the right entry points, and the biology reverses its own direction.
The virtuous flywheel has the same architecture as the vicious one, but the direction of causation reverses. The three pillars now amplify healing instead of disease. I experienced this in three months. My carotid plaque: gone. My LDL is down 64%. My ApoB at 45. My D1 CT-FFR improved from 0.75 to 0.80, moving from functionally significant stenosis into the low-normal range. The virtuous flywheel is turning.
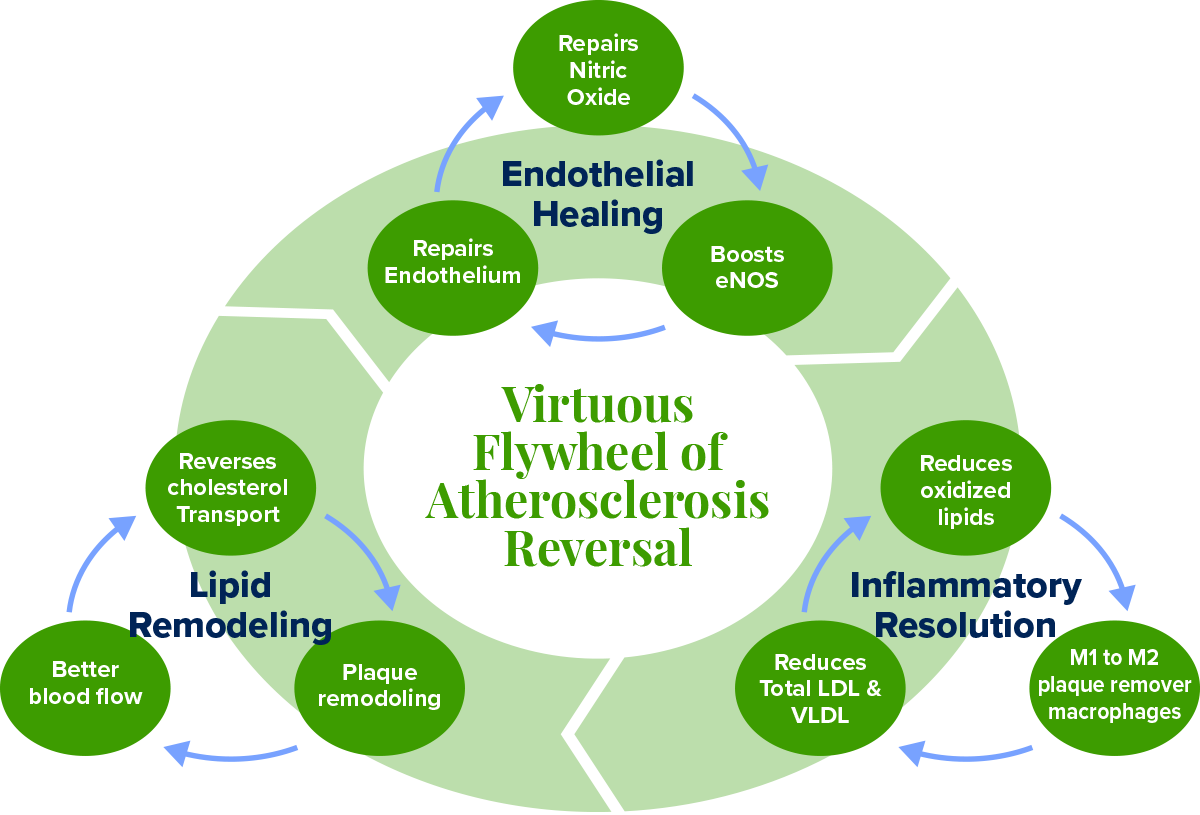
Figure 1. The Virtuous Flywheel of Atherosclerosis Reversal, running clockwise from Endothelial Healing through Lipid Remodeling to Inflammation Resolution. Each master node contains its own three-part sub-cycle.
1. Endothelial Healing. The endothelium does not heal passively. It heals through nitric oxide production, eNOS activation, and endothelial progenitor cell repair. These three mechanisms form their own sub-cycle:
Nitric oxide relaxes the vessel wall and reduces shear-induced injury;
Reduced injury preserves eNOS coupling so it produces more nitric oxide rather than superoxide;
More nitric oxide mobilizes bone-marrow endothelial progenitor cells that replace dead cells and close the breach.
Exercise upregulates eNOS through pulsatile blood flow.
Dietary nitrates from leafy greens feed the oral-gastric pathway, an eNOS-independent route to nitric oxide that works all day as long as you keep eating greens.
Deep sleep pulses growth hormone that drives progenitor cell mobilization overnight.
2. Lipid Remodelling. The right target is not LDL-C but ApoB: the count of every atherogenic particle capable of entering the arterial wall. And the real goal is not merely reducing entry but activating reverse cholesterol transport (RCT): the ABCA1-mediated extraction of cholesterol from foam cells inside the plaque, loaded onto HDL particles, returned to the liver for excretion. This is the mechanism of plaque regression.
Eliminating saturated fat upregulates hepatic LDL receptors.
Exercise activates lipoprotein lipase and improves HDL function.
Intermittent fasting reduces intrahepatic fat and VLDL overproduction.
When efflux exceeds influx, the necrotic core shrinks, and the fibrous cap thickens.
Two upstream drivers of this node are almost never discussed in standard cardiology.
The first is HbA1c. Hyperglycemia glycates LDL particles, and glycated LDL is taken up by macrophages at a far higher rate than native LDL, accelerating foam cell formation regardless of your ApoB count. It also generates advanced glycation end products that cross-link collagen in the arterial wall, stiffening it and making the endothelium less responsive to nitric oxide. Insulin resistance simultaneously drives hepatic VLDL overproduction, directly raising ApoB burden. Target HbA1c for cardiovascular protection is below 5.4%, well below the conventional pre-diabetes threshold of 5.7.
The whole food plant-based diet and
16:8 fasting are the two most powerful interventions.
The post-meal walk serves the same purpose acutely, clearing glucose from circulation before it can glycate anything.
The second overlooked driver is Vitamin K2 (MK-7).
Without sufficient K2, calcium that circulates in the bloodstream deposits into arterial walls and inside existing plaque, hardening the necrotic core and converting soft, potentially reversible plaque into fixed calcified lesions. K2 activates Matrix Gla Protein (MGP), the most potent known inhibitor of vascular calcification, which redirects that calcium back into bone instead. The Rotterdam Study demonstrated that K2 specifically, not K1, significantly reduced cardiovascular mortality and aortic calcification. The natto I already eat as an MK-7 source does double duty: the nattokinase degrades fibrin and the K2 inhibits calcification. These are distinct mechanisms from the same food, and worth tracking separately in any serious protocol.
3. Inflammation Resolution. The CANTOS trial proved that targeting inflammation alone, with no lipid lowering whatsoever, reduced major cardiovascular events by 15%. This is co-primary biology. The judo move is to shift macrophages from the M1 (inflammatory, cap-degrading) phenotype to the M2 (healing, collagen-depositing) phenotype.
Curcumin suppresses NF-kB and drives M2 polarization.
EGCG from high-catechin green tea reduces foam cell formation.
Ellagitannins from pomegranate juice upregulate ABCA1 expression in macrophages, directly increasing their capacity for cholesterol efflux.
Exercise myokines shift the immune environment toward M2.
Intermittent fasting activates autophagy to clear permanently inflamed senescent macrophages that no diet can repolarize.
The direct blood readout of this node is hs-CRP. High-sensitivity C-reactive protein is produced by the liver in response to IL-6, which is secreted by activated M1 macrophages and visceral adipose tissue. It is the most accessible systemic signal of whether your inflammatory node is moving in the right direction. Target is below 1.0 mg/L for optimal cardiovascular protection. Your polyphenol stack, your HIIT sessions, and your fasting protocol all suppress IL-6 at the source, and hs-CRP should track downward as a consequence. I measure it quarterly alongside ApoB and HbA1c as the three primary biomarker proxies for flywheel direction.
“Nitric oxide is arguably the most important molecule in the cardiovascular system. It is the endothelium’s primary defence against virtually every step in the development of atherosclerosis. You want more of it. Almost everything about modern life gives you less.”
Louis J. Ignarro, PhD. Nobel Laureate in Physiology or Medicine, 1998.
The Polluted Gas is Your Saviour
“I spent my career studying a gas that everyone assumed was just a pollutant. It turned out to be the most important signaling molecule the body makes. The lesson is: never assume you know what something is before you study it.”
Louis Ignarro, PhD. Nobel Laureate, 1998.
In 1980, before statin drugs were approved in 1987, a pharmacologist named Robert Furchgott was running experiments on strips of rabbit aorta in his laboratory at the State University of New York. He was studying how the blood vessel relaxed in response to acetylcholine, a signalling molecule that, according to the textbooks, should cause smooth muscle to dilate. It did. Except that sometimes it did not. Sometimes it caused contraction instead. Furchgott could not account for the inconsistency, and inconsistency in a careful scientist’s data is not noise to be discarded. It is a signal to be followed.
He eventually traced the discrepancy to a preparation error. When his laboratory assistants accidentally scraped the inner surface of the aorta during dissection, stripping away the single-cell endothelial lining, the acetylcholine caused contraction. When the endothelium was intact, it caused relaxation. The endothelium, he concluded, was producing something: a chemical messenger that told the smooth muscle underneath it to relax and let blood flow freely. He had no idea what it was. He called it EDRF: Endothelium-Derived Relaxing Factor. The name was a placeholder for a mystery.
It took seven more years to solve it. Louis Ignarro in California and Ferid Murad in Texas, working independently and sometimes in competition, converged on the same answer: EDRF was nitric oxide. A gas. A molecule of one nitrogen atom and one oxygen atom. In the brain, it acts as a neurotransmitter, in the immune system, it can kill cancer cells, and in the blood vessels, it can dilate them and prevent platelet aggregation and plaques.
At the time, nitric oxide was known primarily as an atmospheric pollutant and a component of smog. The idea that the human body was producing it deliberately, in the precise inner lining of every blood vessel, and using it to regulate blood flow, prevent clotting, suppress inflammation, and protect the arterial wall from disease, was received as implausible. It was implausible in the way that the best biological discoveries always are: it seemed impossible until the moment it seemed obvious. In 1998, Furchgott, Ignarro, and Murad shared the Nobel Prize in Physiology or Medicine. The molecule they had discovered was not a drug. It was a birthright. And most people are running chronically deficient in it because of what they eat.
I sat across from Dr. Caldwell B. Esselstyn Jr. on a Zoom call two weeks ago. 92 years old. Sharp as a blade. He had reversed heart disease in patients so severe they could not shave without triggering angina. His oldest patient, Stanley, came to him at age 87 on his last days of life due to severe heart disease requiring a bypass which would most likely end his life, changed to the Esselstyn diet protocol. Stanley called him at 103 to say thank you. Esselstyn leaned forward into the screen and said four words that reorganized everything I thought I knew about diet: “You need to revive your endothelium. There is an enzyme in the endothelial cells called eNOS, endothelial nitric oxide synthase, that produces nitric oxide. This is the miracle gas that will revive your endothelium.”
The pathway is simpler than any drug. Leafy greens carry dietary nitrates. The bacteria in your mouth convert those nitrates to nitrites. Stomach acid converts nitrites to nitric oxide, the same molecule your endothelium desperately needs, delivered directly to your circulation for hours after every meal. This is why Dr. Esselstyn prescribes greens six times daily, balsamic vinegar to amplify the conversion, and the removal of antiseptic mouthwash and antacids, both of which destroy the biological machinery that runs this pathway. “So your blood vessels are anointed with nitric oxide all day long.” Say YES to NO (nitric oxide). It is the simplest, most powerful cardiovascular intervention available to you today, and it requires no prescription.
“We have been measuring the wrong things. Cholesterol is the fuel. Inflammation is the fire. You can reduce the fuel all you want, but if the fire is still burning, the house still burns down.”
Paul Ridker, MD. Brigham and Women’s Hospital.
My Health Reversal Flywheel
“The doctor of the future will give no medicine, but will interest patients in the care of the human frame, in diet, and in the cause and prevention of disease.”
Thomas Edison, 1903. He was 123 years early.
I want to be specific, because the gap between principle and practice is where most protocols fail. So here is exactly what I do, and why each piece is there.
Diet is the foundation, and I follow Dr. Esselstyn’s whole food plant-based protocol without modification:
No saturated fats, which removes the primary dietary suppressor of eNOS and the main driver of ApoB particle production.
Leafy greens six times daily, boiled briefly and eaten with balsamic vinegar or lemon juice, which fuels the oral-gastric nitrate pathway continuously throughout the day.
50 millilitres of pomegranate juice with each meal, for the ellagitannins that upregulate ABCA1 in macrophages and directly support reverse cholesterol transport.
No antiseptic mouthwash, no antacids, because both destroy the biological machinery, the oral bacteria and gastric acid, that converts dietary nitrates into nitric oxide.
15-30 minute walk after each meal to activate lipoprotein lipase before triglyceride-rich particles can oxidize and reduce post-meal glucose spikes.
Exercise is non-negotiable and irreplaceable. I do HIIT three times weekly at 60 to 80 percent of my maximum heart rate for at least 1 hour. I keep the 4 x 4 minute High Intensity protocol in mind, but I do this for three reps up hills on my bicycle. I often wonder exactly what is happening to the blood flow and my heart blockages every time I go up that hill during these efforts. Theoretically, I know they are helping, but I often wonder.
This is not aesthetics. Pulsatile blood flow during sustained aerobic work is the most potent physiological stimulus for eNOS upregulation that exists. A single bout measurably improves endothelial function within hours. Sustained over months,
it upregulates eNOS expression,
mobilizes endothelial progenitor cells from bone marrow,
produces M2-polarizing myokines, and
improves both LDL receptor activity and
lipoprotein lipase-mediated triglyceride clearance.
No drug achieves this breadth of mechanism simultaneously.
I fast 16 hours daily, eating within an 8-hour window. This is not primarily about weight.
Fasting suppresses mTOR, the molecular driver of the M1 inflammatory macrophage phenotype.
It activates autophagy, the cellular recycling process that clears the senescent, permanently inflamed macrophages that no dietary intervention can repolarize.
It reduces intrahepatic fat, the primary driver of VLDL overproduction, and
reliably lowers fasting triglycerides.
Combined with the dietary protocol, it shifts the entire lipoprotein landscape.
Sleep is my acknowledged weak point, and I am correcting it. During slow-wave sleep, the pituitary releases growth hormone in pulses that drive endothelial progenitor cell mobilization. Every night of disrupted sleep is a night without the repair crew. I optimize for deep sleep duration before any other sleep metric.
My supplement stack is built around mechanism, not marketing. Every item has a specific address in the flywheel:
Nattokinase 6,000 FU: fibrin degradation, microvascular flow, thrombotic risk reduction
Aged garlic extract 2,000mg: most human-trial-validated natural agent for endothelial function and eNOS support
Algae-derived EPA and DHA: ABCA1 upregulation, M2 macrophage polarization, no oxidized fat burden of fish oil
Curcumin: direct NF-κB inhibition, M1-to-M2 macrophage shift
Vitamin C 1 to 3g daily: nitric oxide stabilization, antioxidant protection of eNOS coupling
Spirulina: phycocyanin for eNOS upregulation and anti-inflammatory activity
From natto and green tea
Vitamin K2 as MK-7 (from natto): activates Matrix Gla Protein to block vascular calcification and redirect calcium to bone
High-EGCG green tea tablets: foam cell reduction, eNOS activation, NF-κB suppression
The three biomarkers I track quarterly as flywheel proxies are
ApoB (lipid remodelling node),
hs-CRP (inflammation resolution node), and
HbA1c (upstream metabolic driver of both lipid and inflammation nodes).
Together, they tell you which direction each sub-cycle is turning without waiting for the next imaging study.
The results, in five months of this protocol:
D1 stenosis of 77%: CT-FFR improved from 0.75 to 0.80, moving from functionally significant into the low-normal range.
Bilateral carotid CIMT reduced by 53 percent in the first three months.
All carotid plaque (~20%): gone.
LDL down 64 percent. ApoB at 45. In 12 weeks
My physician friends use the word ‘unbelievable.’ What they mean is: I don’t truly believe it.
Rob Thompson did not have this wisdom. He had a cup of tea on a February morning and an arterial wall that had been accumulating evidence against him for forty years. You have what Rob did not have. I pray you do something with this wisdom for you and your loved ones.
Your Questions
Questions worth sitting with. Answer them honestly.
1. Which flywheel are you on right now?
Not as a metaphor. Mechanically. Is your endothelium being damaged by what you eat and how you sleep, or is it being repaired? Are your macrophages in M1 inflammatory mode or shifting toward M2? The flywheel does not pause while you decide. It is spinning right now, in one direction or the other. The fractal 80/20 says you do not need to fix everything. You need to find your one thing. For most people reading this, that one thing is what they eat for breakfast.
2. What is your number one constraint?
In the theory of constraints, identifying the bottleneck is the entire game. For your cardiovascular health specifically, is it diet, and you know it? Is it sleep, which you have been meaning to address for two years? Is it that you have never had imaging and are operating on assumptions? The constraint you do not name is the one that governs everything. Name it. Then remove it. Everything else is secondary until that one is solved.
3. What is the one action you will take this week that your endothelium will thank you for?
Not a lifestyle overhaul. One thing. Order a CT calcium scan if you have never had one. Replace one saturated-fat meal with leafy greens and balsamic vinegar. Start a post-dinner walk. Ask your doctor for an ApoB measurement at your next appointment. The virtuous flywheel does not require a dramatic first push. It requires a real one. Small, specific, this week.
Someone You Love
There is someone in your life with this right now.
You thought of them somewhere in this story.
Maybe it is you.
Send this to the person you thought of while reading it. Ten seconds. It may matter more than either of you knows.
MORE READINGS YOU’LL ENJOY
Health
Reversing My 77% Heart Plaques
Stats Say You Likely Have Heart Plaque
The Healing Power of Food: Nitric Oxide
Wealth
The Power of the Compound Effect
Relentless Iteration to Mastery
Meaning
The Courage to Your Magnum Opus
APPENDIX
Key Studies in Atherosclerosis, Reversal and Cardiovascular Biology
All studies cited are peer-reviewed publications. Human trial data is prioritized throughout. This appendix reflects the evidentiary basis of the REVERSAL Protocol.
Foundational Science: The Inflammatory Basis of Atherosclerosis
1. Ross R. (1999). Atherosclerosis: an inflammatory disease. New England Journal of Medicine. Established the foundational framework that atherosclerosis is a chronic inflammatory disease of the arterial wall, not a lipid storage disorder.
2. Libby P, Ridker PM, Maseri A. (2002). Inflammation and atherosclerosis. Circulation. Detailed the molecular mechanisms by which inflammatory pathways drive every stage of plaque formation, from initial endothelial activation through vulnerable plaque and rupture.
3. Tabas I. (2010). Macrophage death and defective inflammation resolution in atherosclerosis. Nature Reviews Immunology. Demonstrated that macrophage apoptosis and defective efferocytosis drive the formation of the necrotic core that makes plaques vulnerable to rupture, independent of lipid accumulation.
4. Ridker PM et al. (2017). Antiinflammatory therapy with canakinumab for atherosclerotic disease (CANTOS Trial). New England Journal of Medicine. Proved that targeting IL-1 beta reduced cardiovascular events independent of any lipid lowering, establishing vascular inflammation as a standalone therapeutic target.
Endothelial Biology and Nitric Oxide
5. Lundberg JO, Weitzberg E, Gladwin MT. (2008). The nitrate-nitrite-nitric oxide pathway in physiology and therapeutics. Nature Reviews Drug Discovery. Established the oral-gastric dietary nitrate pathway as a clinically significant, eNOS-independent source of nitric oxide directly activated by leafy green vegetable consumption.
6. Fukai T, Ushio-Fukai M. (2011). Superoxide dismutases: role in redox signaling, vascular function and diseases. Antioxidants and Redox Signaling. Explained how oxidative stress uncouples eNOS, converting it from a nitric oxide producer to a superoxide generator that accelerates endothelial injury.
7. Werner N et al. (2003). Intravenous transfusion of endothelial progenitor cells reduces neointima formation after vascular injury. Circulation Research. Demonstrated that endothelial progenitor cells actively repair damaged vessel walls and that exercise is a primary driver of their mobilization from bone marrow.
Diet and Plaque Reversal
8. Ornish D et al. (1998). Intensive lifestyle changes for reversal of coronary heart disease (Lifestyle Heart Trial). JAMA. Showed measurable angiographic coronary artery disease regression in 82% of participants at one year and continued regression at five years, without lipid-lowering drugs.
9. Esselstyn CB Jr et al. (2014). A way to reverse CAD?. Journal of Family Practice. Found that 99.4% of compliant patients with established, angiographically confirmed coronary artery disease avoided major cardiovascular events over 3.7 years on a whole food plant-based diet.
10. Estruch R et al. (2013). Primary prevention of cardiovascular disease with a Mediterranean diet (PREDIMED Trial). New England Journal of Medicine. Demonstrated that a Mediterranean dietary pattern significantly reduced major cardiovascular events, particularly stroke, compared to a low-fat control diet.
11. Aviram M et al. (2004). Pomegranate juice consumption for 3 years by patients with carotid artery stenosis. Clinical Nutrition. Showed a 35% reduction in carotid intima-media thickness and significantly reduced LDL oxidation and blood pressure over three years of pomegranate juice consumption in a human trial.
12. Mensink RP, Katan MB. (1992). Effect of dietary fatty acids on serum lipids and lipoproteins. Arteriosclerosis and Thrombosis. Established the quantitative relationship between saturated fatty acid intake and LDL receptor downregulation, explaining the mechanistic link between dietary saturated fat and elevated ApoB particle count.
Exercise and Cardiovascular Reversal
13. Hambrecht R et al. (2004). Percutaneous coronary angioplasty compared with exercise training in patients with stable coronary artery disease. Circulation. Showed in a randomized trial that regular aerobic exercise was superior to PCI in preventing death and recurrent MI at 12 months in patients with stable coronary artery disease.
14. Pedersen BK, Febbraio MA. (2012). Muscles, exercise and obesity: skeletal muscle as a secretory organ. Nature Reviews Endocrinology. Described the myokine system by which contracting skeletal muscle releases anti-inflammatory signals including IL-10 that polarize macrophages toward the M2 healing phenotype.
15. Tall AR. (2008). Cholesterol efflux pathways and other potential mechanisms involved in the link between HDL and antiatherosclerotic effects. Journal of Internal Medicine. Reviewed ABCA1-mediated cholesterol efflux from macrophages as the rate-limiting step in reverse cholesterol transport and plaque regression, establishing why HDL function matters more than HDL-C level.
Fasting, Macrophage Biology and Polyphenols
16. Longo VD, Mattson MP. (2014). Fasting: molecular mechanisms and clinical applications. Cell Metabolism. Summarized the molecular effects of intermittent fasting including mTOR suppression, autophagy induction, and reduction of inflammatory markers relevant to macrophage phenotype and plaque stability.
17. Mantovani A et al. (2004). The chemokine system in diverse forms of macrophage activation and polarization. Trends in Immunology. Established the M1/M2 macrophage polarization framework and the cytokine environments that drive each phenotype, providing the mechanistic basis for dietary and exercise interventions targeting inflammatory macrophage behavior.
Epidemiology and Imaging
18. Enos WF, Holmes RH, Beyer J. (1953). Coronary disease among United States soldiers killed in action in Korea. JAMA. Found gross atherosclerosis in 77% of 300 American combat soldiers with an average age of 22 years, establishing that coronary artery disease begins in youth.
19. Detrano R et al. (2008). Coronary calcium as a predictor of coronary events in four racial or ethnic groups (MESA Study). New England Journal of Medicine. Demonstrated that coronary artery calcium score independently predicted cardiovascular events across diverse populations, validating CT calcium scoring as a primary risk stratification tool.
20. Fuster V et al. (2014). Progression of Early Subclinical Atherosclerosis (PESA) study design. Journal of the American College of Cardiology. Found measurable atherosclerotic plaque in 49.7% of middle-aged adults with no conventional risk factors, demonstrating that standard clinical thresholds vastly underestimate subclinical disease burden.
21. Loree HM et al. (1992). Effects of fibrous cap thickness on peak circumferential stress in model atherosclerotic vessels. Circulation Research. Established the biomechanical basis for why thin-capped, inflamed plaques rupture at low stenosis percentages, explaining why inflammation control is more important than stenosis reduction in preventing acute events.
I pray you unlock your heart to reach the height of your full potential by discovering your calling.
Kevin Ham, MD
Subscribe to my Compounding Wisdom newsletter and start transforming your life. ham.com
Subscribe to my YouTube channel @DrKevinHam for videos on how I reversed my clogged arteries in 3 months, the top foods that clear your arteries, and the first principles of health that can save your life. Like, share and subscribe — it could save the life of someone you love.