
The Diets with No Heart Disease or Cancer
7 Traditional peoples and their diets with no heart disease or cancer, and the cancer record that first set Dr. Esselstyn looking for help for his breast cancer patients and then his most severe cardiac patients.
Dr. Kevin Ham, MD
“Three quarters of the people on this planet had no heart disease. The same peoples carried almost no breast cancer. What were they eating, to the gram, and what does that inform us to eat to be free of our modern day diseases?”
Dr. Kevin Ham
Before Dr. Caldwell Esselstyn became a doctor who prevented and reversed heart disease in the most severe cases at the Cleveland Clinic from 1986 onwards, he was a breast cancer surgeon, and 11 years into that work at the Cleveland Clinic, he grew restless. What unsettled him most was a single fact he could not put down. Roughly three-quarters of the human beings alive had no heart disease at all, and the same people carried strikingly little of the breast cancer he was cutting out of women every week. The common thread was neither a gene nor a drug. It was the food. He himself had a family history of heart attacks, and so he decided to go on this whole plant-based, low-fat diet himself to prevent his own potential demise from a heart attack. His wife went on this diet shortly thereafter when her sister was diagnosed with breast cancer. They are 92 and 90 years old, respectively.
Esselstyn saw that each of these traditional diets had total cholesterol under 150 mg/dL. Below that line, he argued, coronary disease is essentially nonexistent, and he named the people who lived beneath it: central Africa, the highlands of New Guinea, the Tarahumara of northern Mexico, and rural China. Scott Grundy had put the companion figure on the record, that with a blood pressure of 110/70 and a cholesterol under 150, roughly 90% of heart attacks could be avoided. No one has really educated the public well about the plate that would get them there.
I have spent the last year living inside this kind of diet. My own carotid plaque reversed completely in just 3 months on the Esselstyn diet protocol, along with my own first-principles-based layered fasting, and the 5,000 kilometres I ride each year. So this week I went looking for the people Esselstyn pointed at, not for the slogan but for the arithmetic. What did they actually eat, to the gram? Did anyone open their chests and look? And since Esselstyn came to all of this through the breast, what did these same people leave on the cancer record? Seven witnesses answer. Some you will find surprising but definitely informative points of reference to highly consider each time you put something into your mouth.
7 Witnesses For Your Plate
“Eat food. Not too much. Mostly plants.”
Michael Pollan, In Defense of Food
The dietary surveys are old, most of them from the 1950s through the 1990s, the last decades when people still ate the food their grandparents grew before the supermarket reached them. The food we eat today is not the same as what our grandparents grew up with. My father said he ate meat once a year, even though he worked on a farm. Korea went through colonial rule by Japan from 1910 to 1945 and then the Korean War, 1950-1953, where the land and people were ravaged. My father was born in 1936. He is now 90 years old. Now he has a belly with visceral fat due to eating too much and not enough movement, as walking becomes difficult. I have him on two meals a day to reduce his visceral fat; the third meal is really a stored form of high-energy energy in his liver, pancreas, and other organs.
The studies are cross-sectional, and the diagnostic tools were those of their era. No single one of them proves a thing for certain, but it is the convergence, seven peoples on 3 continents arriving at the same place from different foods, that carries the weight.
The First. The Tarahumara of the Sierra Madre.
“The customary diet of the Tarahumaras is hypolipidemic and presumably antiatherogenic.” —William Connor
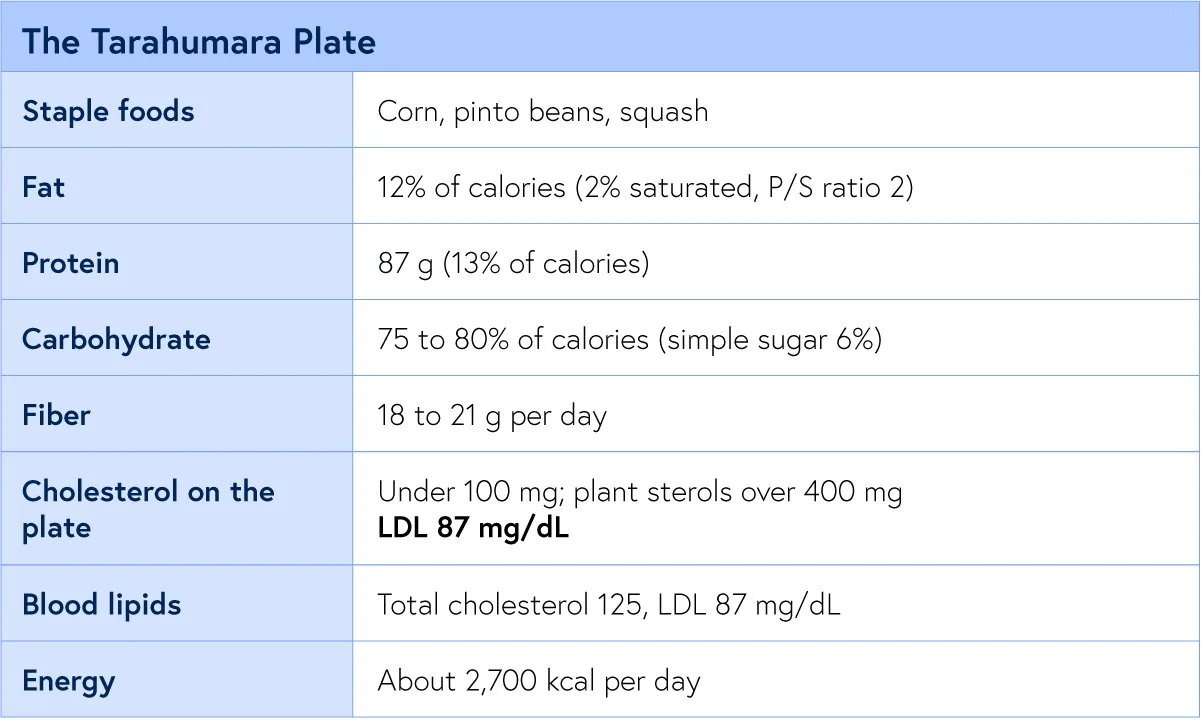
William Connor and his colleagues spent 4 years in the Sierra Madre measuring a people famous for running footraces over distances that would hospitalize most of us. Their plate was corn, pinto beans, and squash, almost no fat and almost no animal food. Their cholesterol ran far below any line a Western clinic draws, and theirs was among the first human populations in which plasma cholesterol could be shown to rise and fall directly with the food on the plate.
The proof that this was the food and not the bloodline came when the same investigators took 13 Tarahumara and fed them a 4,100 kcal affluent diet, heavy in fat and cholesterol, for 5 weeks. Their lipid levels and body weight increased on schedule. The artery follows the plate, in either direction.
The Second. Rural China.
“A good diet is the most powerful weapon we have against disease and sickness.” —T. Colin Campbell, The China Study
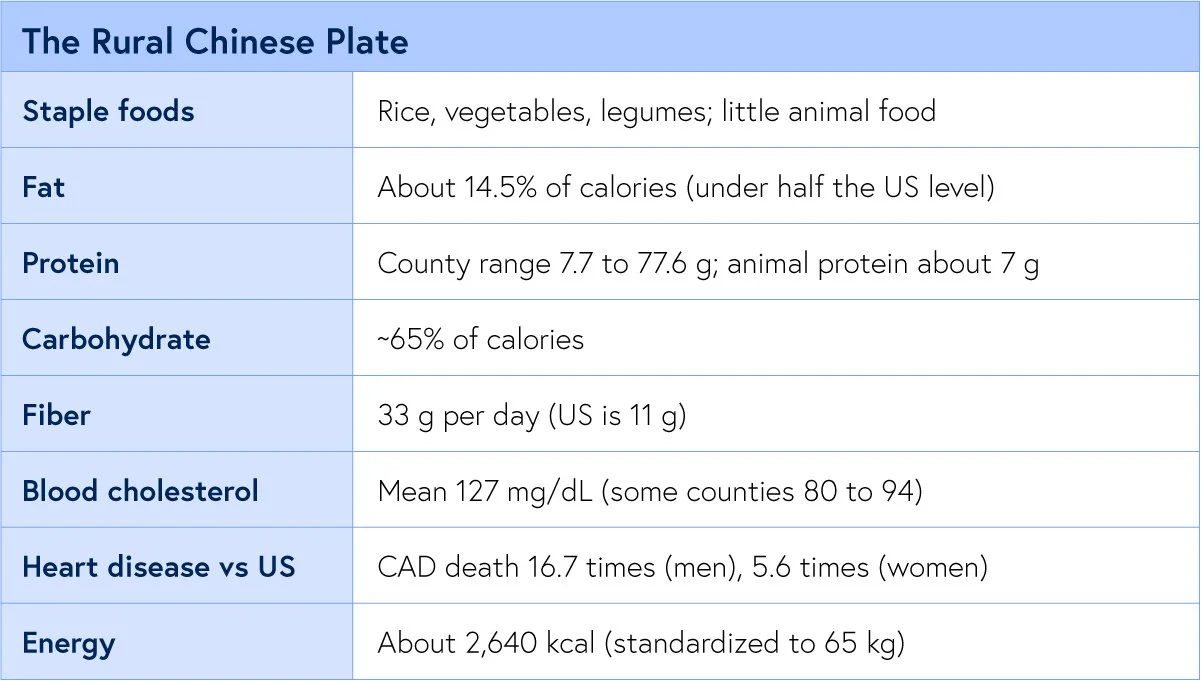
The Cornell-Oxford-China Project remains one of the largest nutritional surveys ever run, collecting blood, food, and mortality data across sixty-five counties. The rural plate carried a fraction of the American fat, several times its fibre, and a tenth of its animal protein. Coronary disease killed American men at many times the rural Chinese rate, and the cholesterol there sat far beneath ours.
This is also the dataset that tied the lipid number to cancer. As cholesterol fell across the counties, so did cancer of the liver, colon, breast, and stomach, and rural breast cancer has climbed since as the villages Westernized. The disease tracks the diet, in real time. The strongest protective signal ran with green vegetables and legumes, the same foods the other six witnesses describe in their own tongues.
The Third. The New Guinea Highlands.
“Ischemic heart disease was rare if not absent as indicated by resting and post-exercise electrocardiograms.” —Sinnett
It’s based on ECG, which is not definitive for atherosclerosis as we now know it, but back then that was what they mistakenly thought was a clean bill of heart health. Even today, it is the exercise stress test and ECG changes that indicate ischemia, but you could have 80-90% blockages and have no positive ECG changes, like my friend Rob who died suddenly of a heart attack. Even I, with 77%, 51%, etc., blockages, had a normal exercise stress test.
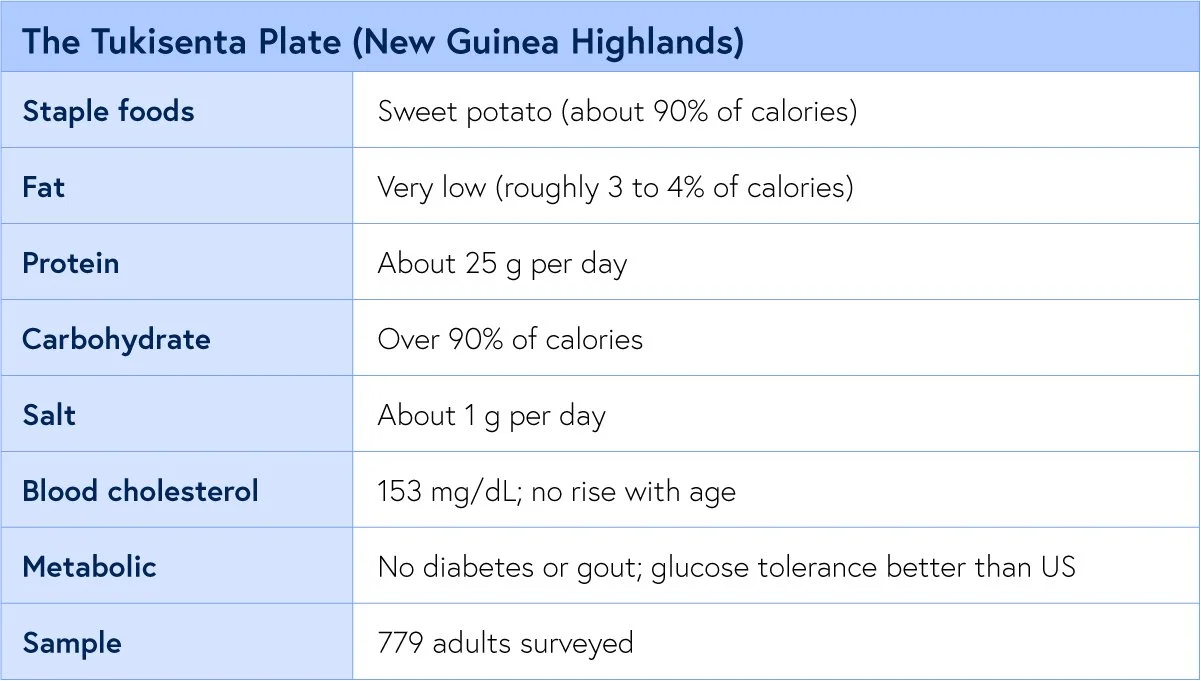
In 1973, Sinnett and Whyte surveyed an entire highland population at Tukisenta and recorded the most extreme diet in the literature, with almost all (90%) of it sweet potato, with fat nearly absent. By every modern reflex it should have wrecked them. Instead, there was no rise with age in blood pressure, cholesterol, blood sugar, or body fat; no diabetes, no gout; and ischemic heart disease was essentially absent. Their glucose tolerance, by the same test used on Americans, was better than ours.
The Fourth. Central Africa.
“In the African population of Uganda coronary heart disease is almost non-existent. This statement is confirmed by adequate necropsy evidence.” —Shaper
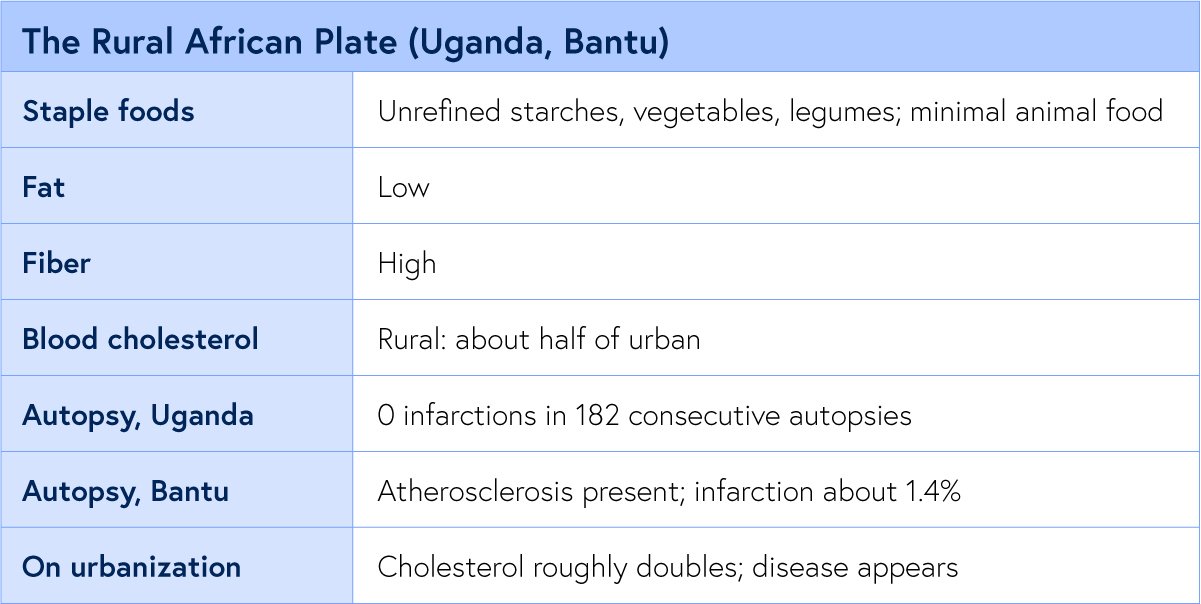
Here the evidence is not a questionnaire. It is the autopsy table, which is why this witness matters most. When pathologists in Uganda opened 182 consecutive bodies, they found not one heart attack. The plate was low in fat, unrefined starch and fibre, plantains, sweet potatoes, millet, vegetables, and almost entirely plant protein.
In the South African Bantu, atherosclerosis in the aorta and fatty streaks in the coronary arteries did occur, sometimes severely in the aorta, yet the fatal infarct stayed rare.
Heart disease appeared on cue wherever Africa urbanized to the Western diet.
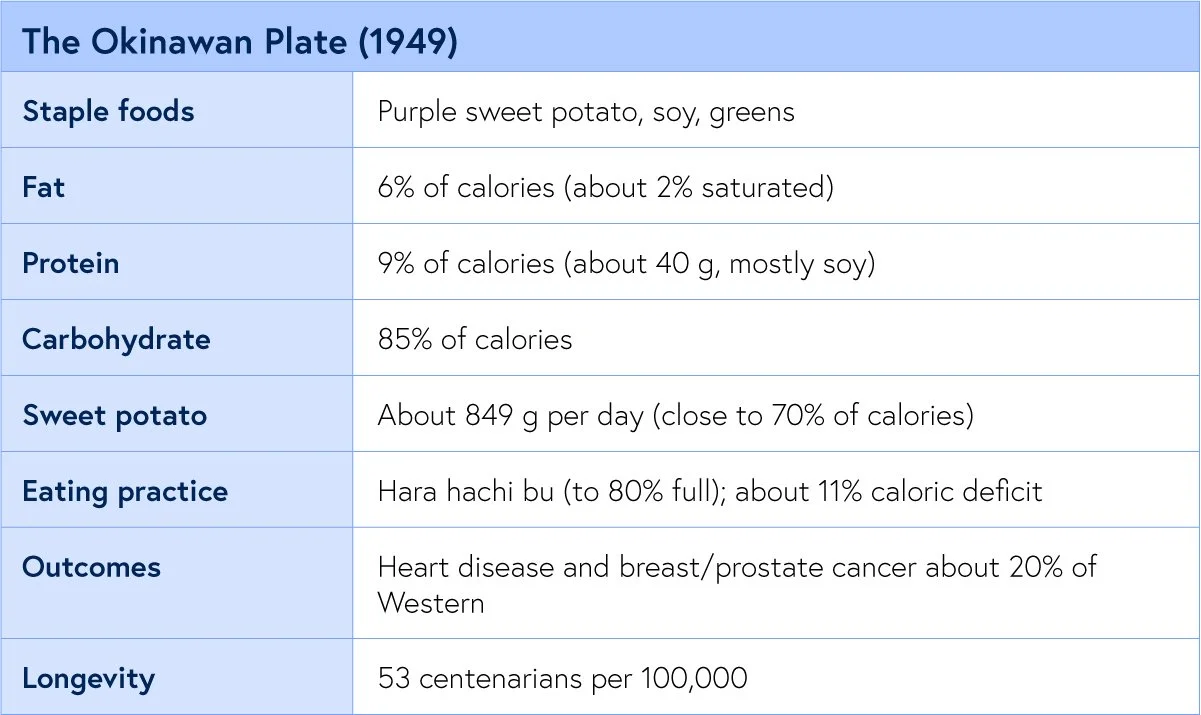
The Fifth. Okinawa, 1949.
“Hara hachi bu: eat until you are 80 percent full.” —Okinawan proverb
The Okinawan record is the best-reconstructed of all because Japan surveyed the islands just after the war. The purple sweet potato supplied most of the plate, soy most of the protein, and fat almost nothing.
And the Okinawans did something none of the other six did on purpose. They ate to about 80 percent fullness and lived in a mild caloric deficit. The result was the highest concentration of centenarians in the world, with heart disease and the hormonal cancers near a fifth of the Western rate.
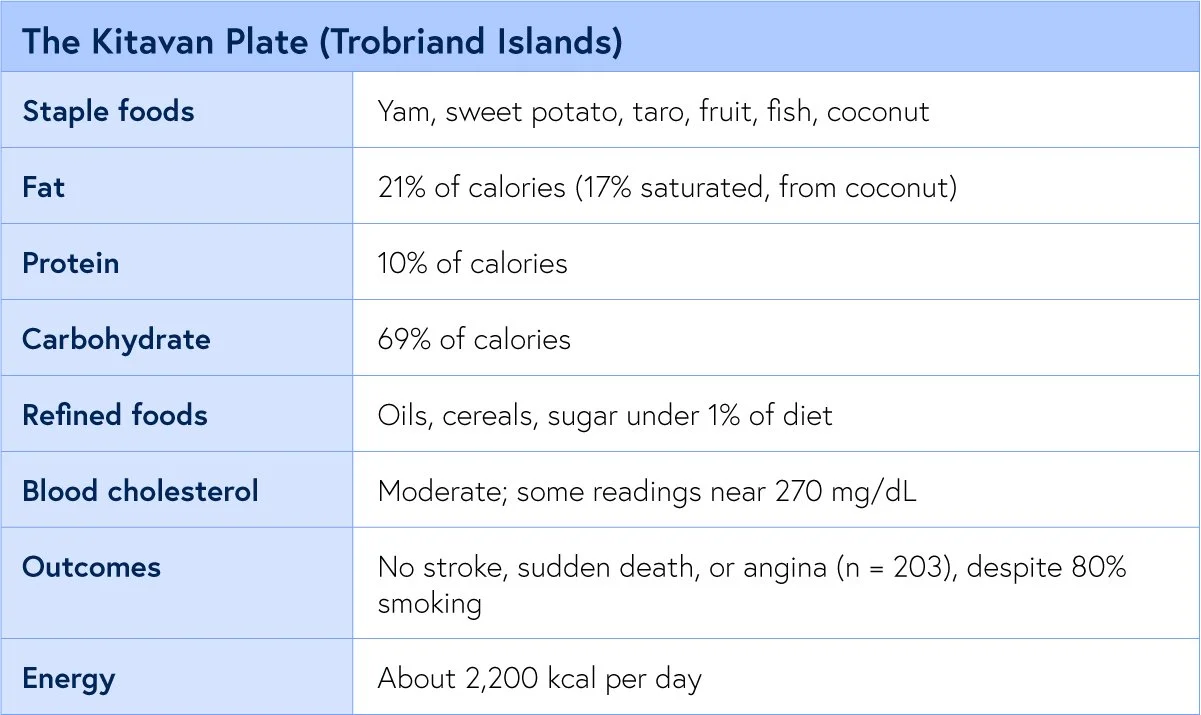
The Sixth. Kitava.
“Apparently free from stroke and ischaemic heart disease.” —Staffan Lindeberg, the Kitava Study
Staffan Lindeberg, the Kitava Study
Staffan Lindeberg spent years on Kitava measuring a people who still ate yam, sweet potato, taro, fruit, fish, and coconut, with refined food at well under one percent of the diet. Among the adults he followed into their nineties, not one case of stroke, sudden death, or angina was found, and this held even though most Kitavans smoked and the coconut pushed some cholesterol readings high. Lindeberg credited leanness and low blood pressure, not a low lipid number, with the protective work.
I have low blood pressure and am lean (BMI was 22)and had severe clogged arteries with LDL at 168mg/dL. Now LDL is 61, and my carotid plaque reversed fully, and CIMT is normal (from 1.8 mm to 0.83 mm in both carotids)
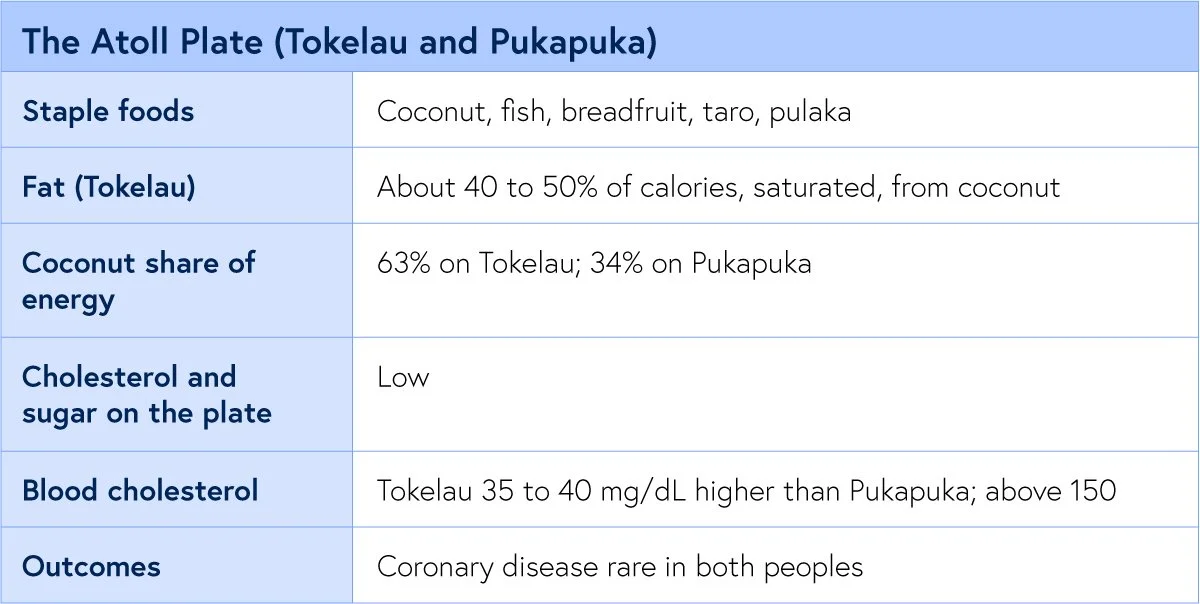
The Seventh. The Polynesian Atolls.
“Vascular disease is uncommon in both populations.” — Ian Prior, 1981
Ian Prior studied two atoll peoples, the Tokelauans and the Pukapukans, in what he called a natural experiment. Coconut supplied most of their energy, so their saturated fat intake was enormous, and their cholesterol sat well above Esselstyn’s line. And yet coronary disease was rare in both. This is the witness that complicates the clean story, and the most instructive of the seven, which is exactly why I keep it in.
7 Traditional diets that frame the diets that have almost no heart disease or cancers. But what about the autopsy evidence?
What the Autopsies Show
“The easy objection is that these peoples were simply dying before the disease could show. The autopsy table answers it. They opened the chests, and the infarctions were not there.”
Dr. Kevin Ham
Every epidemiologist who has ever reported a healthy population hears the same rebuttal. The disease was there; you just missed it, because the people died young of something else or were never properly examined. It is a fair objection, and the African necropsy literature is the cleanest answer we have to it. You cannot miss a myocardial infarction on a body you have already opened. Among 182 consecutive Ugandan autopsies, there were none.
The Bantu series is even more valuable, because it refuses to flatter the thesis. Atherosclerosis was present in those hearts, sometimes badly in the aorta, in 1.4%. What was rare was the clinical event, the large infarct that kills. The plaque existed. It did not rupture, nor did it occlude the way it does in the West. That distinction between having atheroma and dying of it is the whole game, and it points beyond cholesterol alone toward what makes a plaque stable: leanness, low blood pressure, and an absence of refined foods that inflame a vessel wall.
The Kitavans, with their coconut-driven cholesterol near 270 and their cigarettes, and the Tokelauans with their 40 percent saturated fat, sit in exactly this territory. High numbers, quiet plaques, no events.
The age-of-onset data sharpen it. What the necropsy literature describes is not immunity to atheroma but a vessel wall under so little provocation that the lesion never matures into the thing that kills. Remove the provocation, and even an artery that carries plaque can hold it quiet for a lifetime.
Cancer Dietary Evidence
“Coronary disease is essentially non-existent while hypertension, Western malignancies ... are rarely encountered.”
Dr. Caldwell Esselstyn, MD, Preventive Cardiology, 2001
Because Esselstyn began as a breast surgeon, he never read these populations as a heart story alone. His own argument, laid out in his presidential address to the endocrine surgeons, was blunt. Nations that eat more fat per person carry the highest breast cancer mortality. When people migrate from a low-incidence country to a high one, their breast cancer rate climbs to meet the host country within 2 or 3 generations, which is the single cleanest proof that the cause is the food on the table and not the bloodline. And within one country the gradient holds: rural Japanese women on a low-fat plate had less breast cancer than urban Japanese women on more. The American figure he watched move in his own career, from one woman in 19.1 in 1961 to one in 9 by 1991.
His single most arresting figure is the prostate. In all of Japan in 1958, autopsies recorded just 18 prostate cancer deaths, a rate near 2 per 100,000 men, while American men were dying of it in the thousands. And Japanese men who settled in Hawaii developed far more prostate cancer than those who stayed home. The tumour was not in their genes. It was waiting on a Western plate.
The numbers across the seven hold the same shape. Breast cancer varies more than fivefold between nations and tracks per capita dietary fat closely, running about 7 times higher in the West than in Asia. Sub-Saharan Africa recorded a fraction of the North American breast and colon cancer; Okinawa’s sat near a fifth, and rural China’s fell as its cholesterol fell.
The mechanism that best fits the Asian data is not fat alone but what replaces it. Rural Japanese and Okinawan plates are dense in soy, and the isoflavones in soy, converted by gut bacteria into hormone-like molecules, appear to blunt the estrogen signalling that drives most breast tumours. Women in these populations excrete those compounds at many times the levels observed in Western populations. So the protective plate is doing two things at once: withholding the fat and animal protein that raise circulating hormones, and supplying the plant compounds that quiet them. Subtract the soy and the fibre, add the fat, and the hormonal environment of the Western breast is what remains.
I owe you the honest counterweight, the same one I owe myself on the exercise data. The large Western prospective cohorts, the ones that follow nurses and physicians for a decade, have mostly failed to find a strong link between dietary fat and breast cancer. But read the fine print. Those cohorts sample fat between fifteen and 45 percent of calories. Every protective person in this newsletter lived below 15 percent, with 2 to 3 times the fibre and almost no refined food. The cohorts never measured the place these people lived. You cannot find an effect in a range you never sampled.
Is it the Fat or the Protein?
“If the danger were only fat, the coconut eaters would be dead. The thread through all seven is not low fat alone. It is little animal protein.”
Dr. Kevin Ham
You will hear it argued that I have the wrong villain, that the driver is not fat but protein, and specifically animal protein. The argument has teeth. In a long series of experiments at Cornell, T. Colin Campbell dosed rats with a liver carcinogen and then fed them protein. On 20 percent casein, the protein of milk, the rats grew cancer; on 5 percent, almost none, and he could switch the tumours on and off by raising and lowering that animal protein. Plant proteins, soy and wheat, did not promote the tumours even at 20 percent.
The heart has its own version. When Stanley Hazen and his group at the Cleveland Clinic fed people meat, their gut bacteria turned its carnitine into a compound called TMAO that accelerates atherosclerosis in animals and predicts heart attack and stroke in people. Red and white meat raised it, non-meat protein did not, and the level of saturated fat made no difference at all. Vegetarians, lacking the microbes, barely made it.
I read this as neither a refutation of the fat story nor a footnote to it. Look again at the witnesses. Every one of them ate little fat and little animal protein at the same time, so no population on earth cleanly separates the two.
The protein work is also contested: critics note that Campbell’s low-protein rats may have died of the carcinogen before a tumour could form, and that fish raises TMAO yet protects the heart. My own read is plainer. The Western plate loads fat, animal protein, and refined carbohydrates together, and taking all three down at once empties a plaque. The seven witnesses never ran the controlled experiment. They simply lived the answer.
What the 7 Witnesses Say to Us
“There are always exceptions to the rule. It is the corollary to the rule. Humans are exceptional as is nature in harmony.”
Dr. Kevin Ham
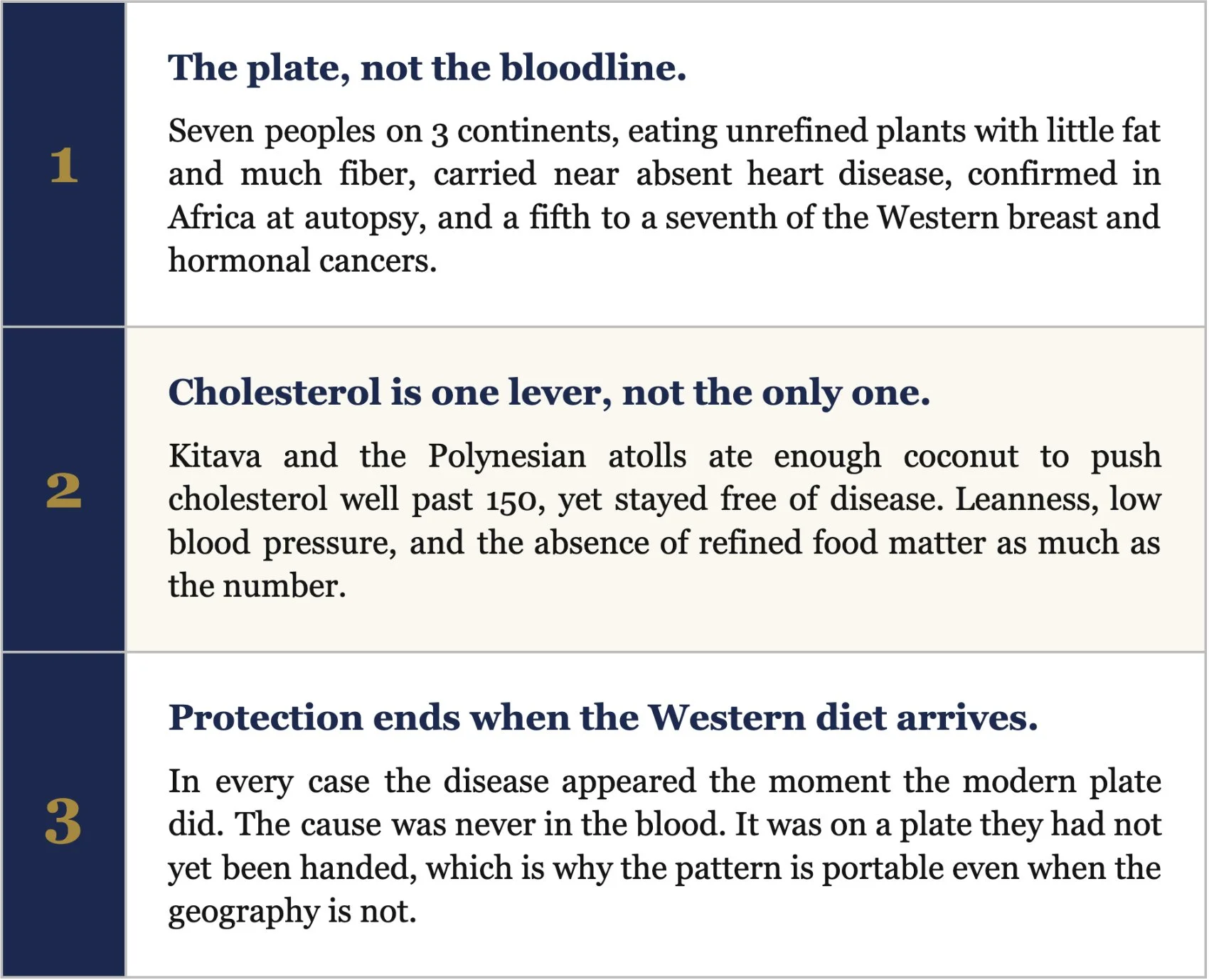
Lay the seven side by side and the pattern is almost monotonous. Six of them sit between 6 and 21% of calories from fat, 9 to 13% protein, fibre at 2 to 3 times the Western intake, refined sugar and oil at or near zero, with lean bodies and a full day of physical work. Those six carry near-absent clinical heart disease, confirmed in Africa on the autopsy table, and roughly a fifth to a seventh of the Western rates of breast and the other hormone-driven cancers.
The two that seem to break the rule, Kitava and the atolls, are the ones I find most clarifying. Both ate enough coconut to carry a cholesterol that would alarm any Western clinic, and both stayed free of heart disease. What they kept is everything else: leanness, low blood pressure, no refined carbohydrate, constant movement. So the line Esselstyn drew at 150 is real and powerful, but it is not the only lever. Leanness is a lever. Blood pressure is a lever. The absence of the refined, oil-soaked, sugar-saturated food that defines our own plate is a lever. The plaque answers to all of them.
And there is the one fact that ties all the witnesses together and shifts the argument from correlation to causation. Each of these peoples lost its protection the moment the Western diet arrived. The Tarahumara fed an affluent plate for 5 weeks. The African who moved to the city. The Okinawan whose mortality advantage vanished as the island Westernized. The disease was never in their blood. It was on a plate they had not yet been handed. That is the whole claim, and it is the reason I ride, and fast, and eat the way I do. The witnesses are unanimous.
3 Things the 7 Teach
“There are always exceptions to the rule. It is the corollary to the rule. Humans are exceptional as is nature in harmony.”
Dr. Kevin Ham
The instruction is plain.
Build the day from whole plants, the grains and beans and tubers and greens that carried all seven of these peoples.
Keep fat low and unrefined.
Drive the cholesterol under the 150 floor that Esselstyn drew, and the LDL well below it, because the lower the lipid drive the faster a plaque empties.
Then add the two levers that Kitava and the atolls prove matter as much as the number. Stay lean. Move every day.
The vessel will follow the plate, and it will follow it in 3 months, not 30 years.
That is the claim I am living, one CT angiogram at a time. The seven witnesses arrived there without trying. We have to choose it.
A Question to Meditate On This Week
“If the healthiest hearts that ever lived were built by what people ate on an ordinary day, then what is the one thing on my own plate that these 7 peoples never touched, and what would change in me if I set it down, starting with my very next meal?”
You do not have to move to the Sierra Madre or remake your whole life by Sunday. You only have to choose one plate, and then the next one. So this week, name the single food on your table that belongs to the modern diet and not to the witnesses: the added oil, the refined sugar, the processed meat, and set it down. Then watch how fast your body answers. The artery is listening; it reverses in months and not decades, and it does not care how small that first meal looks. These 7 peoples inherited their pattern without choosing it. You get to choose yours, one plate at a time, beginning with the very next time you sit down to eat. Start there. Start today.
Therefore choose life, that you and your offspring may live.
Deuteronomy 30:19
A Request
Each Friday, I upload a new YouTube video. Please like, comment and subscribe so I can help many others in your network and beyond. It’s my mission to help people avoid the same fate as Rob, the same fate as I could have had. Heart attack, stroke or sudden death.
https://www.youtube.com/@DrKevinHam
My latest video is going viral :) My #1 meal to unclog arterial plaque. Thank you.
For Someone You Love
There is someone in your life running and falling. You thought of them. Send this to them. Your loved ones just need the information to act and a guide to help them.
Keep going. The race is long, the road is beautiful, and the body was built to heal.
Grace, strength and love to you.
MORE READINGS YOU’LL ENJOY
Health
Reversing My 77% Heart Plaques
Stats Say You Likely Have Heart Plaque
The Healing Power of Food: Nitric Oxide
Meaning
I pray you unlock your heart to reach the height of your full potential by discovering your calling.
Kevin Ham, MD
Appendix
The summary of the referred exercise studies:
The dietary surveys, the autopsy series, and the cancer and protein evidence behind this issue, each with a brief synopsis.
1. Connor WE, Cerqueira MT, Connor RW, et al. The plasma lipids, lipoproteins, and diet of the Tarahumara Indians of Mexico. Am J Clin Nutr. 1978;31:1131 to 1142.
Cross sectional survey of 523 Tarahumara aged 5 to 70, sampled across 4 years in the Sierra Madre, with plasma lipids and lipoproteins measured against detailed dietary records. Mean total cholesterol 125 mg/dL, LDL 87, VLDL 21, HDL 25, triglyceride 120; children averaged 116. Total cholesterol tracked directly with the small amount of cholesterol on the plate, among the first such dose response relationships shown in a free living people. Established the corn, bean, and squash diet as hypolipidemic and antiatherogenic, and the Tarahumara as a living low cholesterol reference population.
2. Cerqueira MT, Fry MM, Connor WE. The food and nutrient intakes of the Tarahumara Indians of Mexico. Am J Clin Nutr. 1979;32:905 to 915.
Detailed weighed and recall dietary survey of 372 Tarahumara. To the gram: protein 87 g (13% of energy), fat 12% (saturated 2%, polyunsaturated 5%, P/S ratio 2), carbohydrate 75 to 80% with simple sugar only 6%, crude fiber 18 to 21 g, dietary cholesterol under 100 mg, plant sterols over 400 mg, sodium a moderate 5 to 8 g, on about 2,700 kcal. The most granular macro portrait we have of a traditional very low fat plate, and the companion to the 1978 lipid data.
3. McMurry MP, Cerqueira MT, Connor SL, Connor WE. Changes in lipid and lipoprotein levels and body weight in Tarahumara Indians after consumption of an affluent diet. N Engl J Med. 1991;325:1704 to 1708.
Controlled feeding experiment. Thirteen Tarahumara were moved from their habitual plate of about 2,700 kcal to a calorie dense 4,100 kcal affluent diet rich in saturated fat and cholesterol for 5 weeks. Total cholesterol rose roughly 31% and LDL about 39%, with measurable gains in body weight, triglycerides, and VLDL. The protective profile collapsed in 5 weeks, proving the Tarahumara lipid pattern was diet dependent rather than a fixed genetic trait.
4. Campbell TC, Parpia B, Chen J. Diet, lifestyle, and the etiology of coronary artery disease: the Cornell China Study. Am J Cardiol. 1998;82:18T to 21T.
Ecological study across 65 mostly rural Chinese counties correlating county level diet, blood biomarkers, and cause specific mortality. Mean serum cholesterol 127 mg/dL against 203 in the United States, fat under half the US level, fiber roughly three times higher, animal protein near a tenth; coronary mortality 16.7 times higher in US men and 5.6 times in US women. Cancer mortality at several sites, including breast, fell as county cholesterol declined from about 170 toward 90, with green vegetables and legumes the strongest protective correlates. The largest dataset tying a low cholesterol, plant rich diet to low rates of both heart disease and cancer.
5. Sinnett PF, Whyte HM. Epidemiological studies in a total highland population, Tukisenta, New Guinea. J Chronic Dis. 1973;26:265 to 290.
Total population epidemiologic survey of 779 highlanders over age 15 at Tukisenta, New Guinea. Diet over 90% carbohydrate from sweet potato, protein about 25 g and salt about 1 g daily; no age related rise in blood pressure, serum cholesterol, fasting glucose, or adiposity; no diabetes or gout; glucose tolerance superior to the American Tecumseh cohort tested by the same method. An extreme high carbohydrate, very low fat diet coexisting with metabolic health and essentially absent ischemic heart disease in a lean, active people.
6. Shaper AG, Jones KW. Serum cholesterol, diet, and coronary heart disease in Africans and Asians in Uganda (1959). Reprinted Int J Epidemiol. 2012;41:1221 to 1225.
Clinical and dietary study of African and Asian communities in Uganda, supported by autopsy evidence. Coronary heart disease was almost nonexistent among the rural Africans, contrasted with the rising disease seen in more urban, Westernized groups. A landmark of cardiovascular geography, reprinted in 2012, and one of the four populations Esselstyn names as living below the disease threshold.
7. Higginson J, Pepler WJ. Fat intake, serum cholesterol concentration, and atherosclerosis in the South African Bantu. J Clin Invest. 1954;33:1366 to 1371.
Combined necropsy and biochemical study of the South African Bantu. Coronary atherosclerosis was present and occasionally severe, yet proved myocardial infarction occurred in only about 1.4% of cases, far below contemporaneous European and American figures, with hearts showing small infarcts and patchy fibrosis rather than large transmural infarction; serum cholesterol and fat intake were both low. A cornerstone of the argument that low fat traditional diets blunt the clinical expression of atheroma even when some plaque is present.
8. Florentin RA, Lee KT, Daoud AS, et al. Geographic pathology of atherosclerosis (Uganda autopsy series); with Shaper AG on the Samburu.
Consecutive autopsy series and field cardiology. Among 182 consecutively examined Ugandan autopsies, no myocardial infarctions were found; Shaper separately examined 100 Samburu elders by physical examination and electrocardiography and found no coronary artery disease, despite their pastoralist milk and meat intake. Closes the loophole that the disease was simply undiagnosed, since infarction cannot be missed on an opened heart, and points to leanness and lifelong activity as decisive.
9. Willcox BJ, Willcox DC, Suzuki M. The Okinawa Centenarian Study; with the 1949 Okinawan dietary survey.
The 1949 Okinawan dietary survey paired with the long running Okinawa Centenarian Study. 1949 macros of 85% carbohydrate, 9% protein, and 6% fat, with purple sweet potato near 70% of calories at about 849 g per day and soy the main protein; intake ran about 11% below energy expenditure, reinforced by the practice of hara hachi bu. The cohort later showed about 53 centenarians per 100,000 and heart disease and hormone dependent cancers at roughly a fifth of Western rates. The best documented case of caloric restriction layered on a very low fat plant plate, and of the advantage eroding as the diet Westernized.
10. Lindeberg S, Lundh B. Apparent absence of stroke and ischaemic heart disease in a traditional Melanesian island: Kitava. J Intern Med. 1993;233:269 to 275. With Lindeberg S, et al. Am J Clin Nutr. 1997;66:845 to 852.
Clinical and dietary field study of the Melanesian island of Kitava, largely untouched by Western food. Diet 69% carbohydrate, 21% fat (17% saturated, from coconut), 10% protein, about 2,200 kcal, with oils, cereals, refined fat, sugar, and alcohol together under 1% of energy; among 203 adults aged 20 to 96, interview and examination found no stroke, sudden cardiac death, or exertional angina, despite about 80% being daily smokers, in a strikingly lean population with low diastolic blood pressure. Protection persisting at a coconut driven cholesterol and in the presence of heavy smoking, attributed chiefly to leanness and blood pressure rather than to a low lipid number.
11. Prior IA, Davidson F, Salmond CE, Czochanska Z. Cholesterol, coconuts, and diet on Polynesian atolls: the Pukapuka and Tokelau Island studies. Am J Clin Nutr. 1981;34:1552 to 1561.
Comparative natural experiment between two Polynesian atoll peoples differing in coconut intake. Coconut supplied 63% of energy on Tokelau and 34% on Pukapuka, so saturated fat intake was very high while dietary cholesterol and sucrose stayed low; Tokelauan serum cholesterol ran 35 to 40 mg/dL higher than Pukapukan, attributed to the saturated fat, yet coronary heart disease was uncommon in both. The cleanest demonstration that very high saturated fat from whole coconut did not carry the expected cardiovascular penalty in lean, active peoples free of refined food.
12. Esselstyn CB Jr. American Association of Endocrine Surgeons presidential address: beyond surgery.
A surgeon's synthesis of the international and migration epidemiology of breast cancer, delivered as a presidential address to the American Association of Endocrine Surgeons. Nations with higher per capita fat carry higher breast cancer mortality; migrants from low to high incidence countries reach the host rate within 2 or 3 generations; rural Japanese women on low fat diets have less breast cancer than urban Japanese women; US breast cancer rose from one woman in 19.1 in 1961 to one in 9 by 1991. The origin of Esselstyn's conviction that a 10 to 15% fat plant based diet prevents both the Western cancers and coronary disease.
13. Esselstyn CB Jr. Resolving the coronary artery disease epidemic through plant based nutrition. Prev Cardiol. 2001;4:171 to 177.
Clinical review and argument from Esselstyn's coronary reversal practice. Sets total cholesterol under 150 mg/dL as the level observed in cultures where coronary disease is essentially nonexistent, naming central Africa, the New Guinea Highlands, the Tarahumara, and rural China, and reports halting and reversal of disease in patients held below that line. Frames heart disease and the hormone dependent cancers as twin expressions of the same diet, and supplies the under 150 target this newsletter is built around.
14. International ecological and migration evidence on dietary fat and breast cancer (Carroll; Prentice; Aoki; Boyd).
The body of ecological and migration epidemiology on dietary fat and breast cancer. Incidence varies more than fivefold between nations and correlates with per capita dietary fat at roughly r = 0.8 to 0.9, running about 7 times higher in northern Europe and North America than in much of Asia; Western prospective cohorts sampling fat between 15 and 45% of calories find weaker within population associations. The apparent conflict resolves once you note the protective populations lived below 15% fat, a range the cohorts never sampled.
15. Esselstyn CB Jr (prostate); Annual of Pathological Autopsy Cases in Japan; Akazaki K, Stemmermann GN. Comparative study of latent carcinoma of the prostate among Japanese in Japan and Hawaii.
Esselstyn’s figure traces to Japan’s national pathological autopsy record, which for 1958 logged just 18 autopsy-proven prostate cancer deaths in the entire nation, a rate near 2 per 100,000 men. Akazaki and Stemmermann’s comparative autopsy study found latent prostate carcinoma markedly more common among Japanese men in Hawaii than among those in Japan. Together they argue the prostate tumor is environmental and dietary rather than genetic, since the same gene pool expressed far more disease on a Western plate.
16. Campbell TC and colleagues. Dietary protein level and aflatoxin B1-induced preneoplastic hepatic lesions in the rat. J Nutr. 1987; with Nutrition and Cancer. 1982.
A long series of controlled Cornell experiments in which rats were dosed with the liver carcinogen aflatoxin, then fed differing levels of casein, the protein of milk. Rats on 20 percent casein developed extensive preneoplastic liver lesions while those on 5 percent showed about 75 percent fewer, and tumor promotion could be switched on and off by raising and lowering the animal protein; plant proteins such as soy and wheat did not promote the lesions even at 20 percent. The experimental foundation of the claim that animal protein, not plant protein, drives cancer promotion; the work is contested, since very low protein may let the carcinogen kill cells before tumors can form.
17. Koeth RA, Wang Z, Hazen SL, et al. Intestinal microbiota metabolism of L-carnitine, a nutrient in red meat, promotes atherosclerosis. Nat Med. 2013;19:576 to 585.
Human and mouse study of carnitine, a compound abundant in red meat, and its conversion by gut bacteria into TMAO. Carnitine feeding accelerated atherosclerosis in mice through gut microbes, omnivores produced far more TMAO than vegetarians or vegans, and plasma markers predicted heart attack, stroke, and death across nearly 2,600 patients; later work showed red and white meat raised TMAO while non-meat protein and the level of saturated fat did not. A mechanism by which animal protein, independent of dietary fat, may injure the artery, though the causal weight of TMAO in humans remains debated.
Subscribe to my Compounding Wisdom newsletter and start transforming your life. ham.com
Subscribe to my YouTube channel @DrKevinHamfor videos on how I reversed my clogged arteries in 3 months, the top foods that clear your arteries, and the first principles of health that can save your life. Like, share and subscribe — it could save the life of someone you love.