
Compounding Wisdom
Plaque Progression, Arrest or Reversal?
Plaque regression needs the necessary environment, much of this arising from lifestyle with nuances.
Plaque regression needs the necessary environment, much of this arising from lifestyle with nuances.
Dr. Kevin Ham, MD
I just came back from a two week vacation in Kauai, my first time there. The island was so lush and green, like a rain forest, which meant it rained every single day, although like tropical rainstorms that came just as quickly as they left. My goal was to ground or earth daily, get lots of sunshine for Vitamin D and my eyes and repay my 12.5 hour sleep debt. Mission accomplished. It also left me time to ponder my past year of healthy living, going vegan or rather whole food plant-based, low fat.
I asked myself, am I truly whole food plant-based? I was eating lots of sourdough bread (half whole grain), but when I went out or travelled, pastas and pizzas, which are refined flour. I sampled cookies (oatmeal raisin sourdough cookies) twice a month and occasionally ate white rice when there were no other options, about twice a month. Refined carbs instead of whole foods or whole grains. My oatmeal, although they were steel cut, I deemed still as whole grains, although technically oat groats would be better.
In August 2025 my apolipoprotein B was 45. My LDL cholesterol was 61, HDL 62, triglycerides 61. That was the window in which my carotid intima media thickness fell from 1.8 and 1.6 millimeters to 0.84 and 0.86 and all of my carotid plaque regressed.Regression was not a theory in that window. It was a measurement. I had been on the Esselstyn protocol for 3 months, and I was following it without negotiation. This was from an LDL of 186 in just 12 weeks!
Since then I have run experiments on myself based on studies. Three walnuts a day. Three olives a day.
I also started eating a whole pomegranate daily on top of an already generous berry load. Each addition was small. None of them felt like a departure. Over the following 12 months my LDL has run between 67 and 80, my ApoB between the mid 60s and low 70s, and my triglycerides touched a high of 103. My HDL is stable. That combination is not a random drift. It is a signature where plaque grows steadily.
When ApoB rises, triglycerides rise, and HDL stays flat, the liver is telling you it is exporting more very low density lipoprotein than it used to. That is a carbohydrate and energy handling pattern, not a dietary cholesterol pattern. And it matters more than the LDL number alone suggests, because ApoB counts particles. One ApoB molecule sits on every atherogenic particle, and it is particles, not the cholesterol they happen to be carrying, that lodge in the arterial wall. Going from 45 to 71 is not a 26 point inconvenience. It is ~50% more atherogenic particles arriving at the endothelium every hour of every day for a year.
Because I knew pomegranate juice was so beneficial, I drank 100 ml twice a day instead of my usual 50 ml and I added a whole pomegranate fruit a day. In Jan 2026, my triglycerides spiked from 61 all the way up to 103, still normal, but high TG lead to more very low density lipoproteins (VLDL), which lead to more LDL, especially the smaller kind that carries less cholesterol and more ApoB. I’ve since stopped the whole pomegranate fruit and my TG as of June is 83. I’ve regressed too much in my discipline to be in plaque reversal mode.
So I’ve decided to go back to how disciplined I was in my first three months from May 9 to August 31, 2025. Simple whole foods. I cut out almost all my supplements that I added and just keeping Spirulina and nattokinase with occasional Omega 3 and likely will add back Vitamin D in the winter.
I will also swap out wheat for barley, which will remove bread and pizza. I will try the occasional cauliflower pizza crust vegan pizza (no oils). Then test my labs Aug 4 for new baseline and early to mid September to see the effects in 4-6 weeks and then again at week 8 and then week 12.
I also reflected on Dr. Esselstyn’s star case of Dr. Joe Crowe. Which brings me to the number I actually want. Joe Crowe was 44 when his distal LAD occluded beyond the reach of a stent or a graft. He declined a statin, went on the 10 percent fat whole food plant based protocol, brought his total cholesterol to 98 and his LDL to 38, and his follow up angiogram showed the vessel filling again just 30 months (2.5 years) later. Those two angiograms sit side by side in Esselstyn's book and they are, to me, the most consequential pair of images in cardiology.
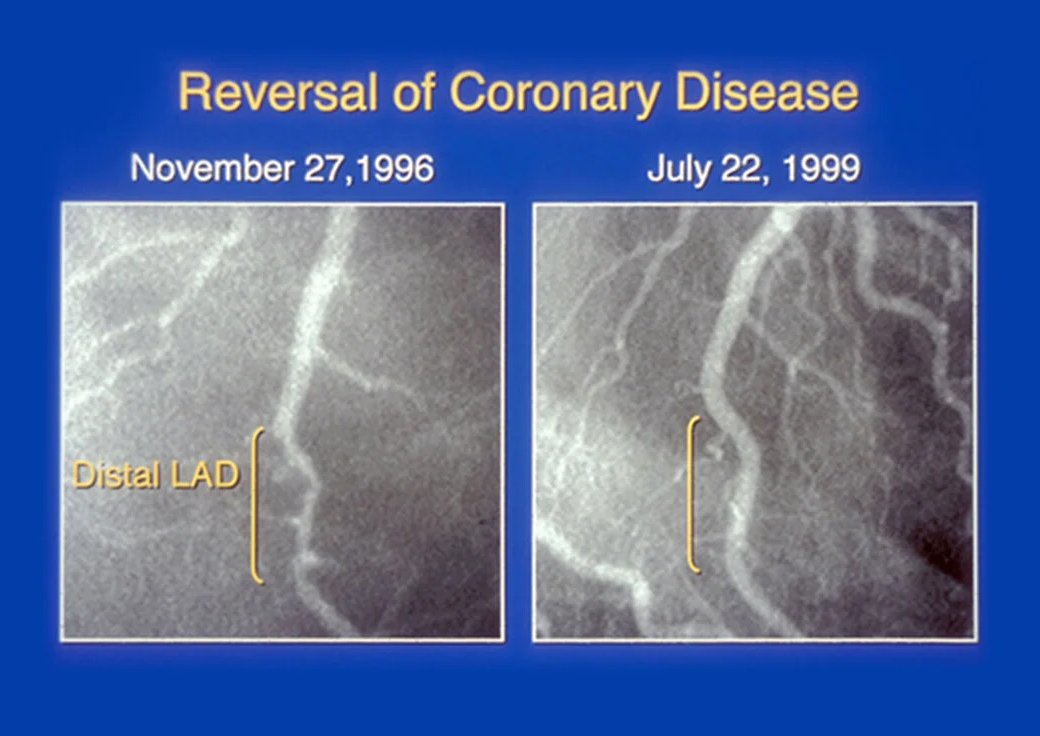
I would like LDL 38. At maximal adherence in 2025 I reached 61, not 38. Crowe reached a total cholesterol of 98 on diet alone, which places him in genuine hyper responder territory. He was 44 with an acute lesion. I am 55 with a calcium score of 505, multi vessel disease, and plaque that is older, more fibrous, and 1/3 calcified. Calcified plaque does not regress easily. Roughly two thirds of my burden is non calcified, and that fraction is the part still in play. So let’s see what the next three months show in my labs. I’ve deeply pondered and researched what it would take to get my LDL < 55 and closer to 40.
Bread and Bile Acids
“Oat bran measurably stimulated bile acid synthesis within 8 hours of a single meal.”
Andersson, Ellegard and Andersson. American Journal of Clinical Nutrition, 2002
Beta glucan is a soluble fiber built from glucose units joined in a mixed pattern of beta 1,3 and beta 1,4 linkages. That mixed linkage is the whole story. A pure beta 1,4 chain is cellulose, which packs into rigid crystalline fibers and dissolves in nothing. Scatter beta 1,3 bonds through the chain and the molecule can no longer pack. It becomes irregular, hydrated, and enormously viscous in water. Beta glucan does not lower cholesterol because it is fiber. It lowers cholesterol because it is thick.
In the small intestine that viscosity slows the mixing of bile acids with the food they are meant to emulsify. Bile acids are the body's detergent, synthesized in the liver directly from cholesterol, secreted into the gut, and then reclaimed. Under normal conditions roughly 95 percent of the bile acid pool is reabsorbed in the terminal ileum (last part of the small intestine) and shipped back to the liver. It is one of the most efficient recycling systems in human physiology. Viscous beta glucan interferes with that recovery, trapping bile acids in the gel phase and carrying them out in the stool.
The liver notices immediately. Losing bile acids means losing the negative feedback signal that normally restrains their production, so the enzyme cholesterol 7 alpha hydroxylase, CYP7A1, is upregulated and the liver begins converting more cholesterol into bile acids to rebuild the pool. That draws down the hepatic free cholesterol pool. A depleted hepatic cholesterol pool activates SREBP-2, which upregulates the LDL receptor on the liver surface. More LDL receptors means more LDL and more ApoB particles pulled out of the bloodstream and cleared. This is precisely the mechanism of the bile acid sequestrant drug class (Cholestyramine), and it is downstream of the same receptor that statins and PCSK9 inhibitors act on from a different angle.
There is a second mechanism operating further down. Beta glucan that survives to the colon is fermented by gut bacteria into short chain fatty acids, particularly propionate. Propionate is absorbed into the portal vein and delivered straight to the liver, where evidence suggests it dampens hepatic cholesterol synthesis. The bile acid mechanism is the dominant one and the best documented. The fermentation mechanism is real, additive, and slower to show up.
3g of Beta Glucan
“Across 14 randomized trials, barley beta glucan lowered LDL cholesterol, non HDL cholesterol and apolipoprotein B.”
Ho, Sievenpiper, Zurbau and colleagues. European Journal of Clinical Nutrition, 2016.
The regulatory threshold on both sides of the Atlantic is 3 grams of beta glucan per day, and the trial evidence supports it. The 2014 meta analysis by Whitehead and colleagues pooled 28 randomized controlled trials of oat beta glucan at or above 3 grams daily and found LDL cholesterol reduced by about 0.25 millimoles per liter, on the order of 4 to 5 percent. The 2016 barley meta analysis by Ho and colleagues found a comparable LDL reduction of about 0.25 millimoles per liter, and it did something the older literature mostly did not. It measured ApoB. Barley beta glucan reduced apolipoprotein B by roughly 15 mg/dL, which is the endpoint I actually care about.
Notice the size of that effect honestly. This is not a statin. A 4 to 7 percent LDL reduction from my current 66 to 80 range moves me a few points, not 20. It is worth having, it is free, it stacks with everything else, and it is the wrong thing to build a strategy around by itself. The larger prize in this issue is what comes out of the diet, not what goes in.
The practical question is how much food 3 grams represents. Most people assume a bowl of oatmeal covers it. It does not, quite, and barley varies more than the packaging suggests.
Table 1 Reaching 3 grams of beta glucan per day
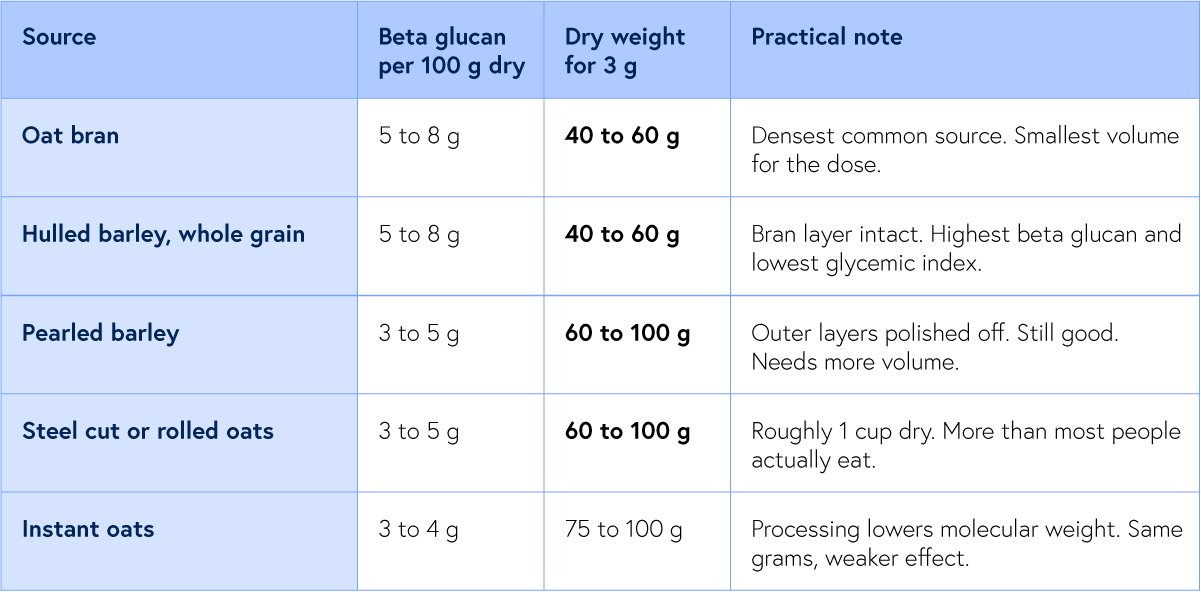
Ranges reflect genuine varietal and analytical variation. Barley cultivars bred for high beta glucan run considerably higher. Weigh dry, not cooked.
One detail in the literature deserves more attention than it gets. Wolever and colleagues showed in a randomized trial that the molecular weight of the beta glucan, not just the quantity, determines how much LDL comes down. High molecular weight beta glucan performed substantially better than the same gram dose after the polymer had been degraded. Grams on a label are not the active dose. Intact viscous polymer is the active dose. Extrusion, fine milling, and prolonged high heat all shorten the chains and thin the gel. This is the same principle that makes an apple different from apple juice, expressed at the level of a single polysaccharide.
The instruction that follows is unglamorous. Cook whole hulled barley or steel cut oats. Do not buy a beta glucan supplement, do not use instant products, and do not blend the finished porridge into a smoothie under the impression you are improving it.
How to make more Resistant Starch
“Cooling cooked white rice raised its resistant starch content and lowered the glycemic response when it was reheated.”
Sonia, Witjaksono and Ridwan. Asia Pacific Journal of Clinical Nutrition, 2015.
Beta glucan is not the only fermentable fraction in a bowl of barley. A portion of the starch itself escapes digestion in the small intestine entirely and arrives in the colon intact, where bacteria ferment it into short chain fatty acids. This fraction is called resistant starch, and it is classified as a carbohydrate on the label while behaving in the body like fermentable soluble fiber. It yields roughly 2 kilocalories per gram rather than 4. Resistant starch is the part of a starchy food that never becomes glucose.
The classification devised by Englyst and Cummings divides it into 4 types, and the distinction is practical rather than academic, because 2 of the 4 are things I can deliberately create or destroy in my own kitchen.
Table 2 The 4 types of resistant starch
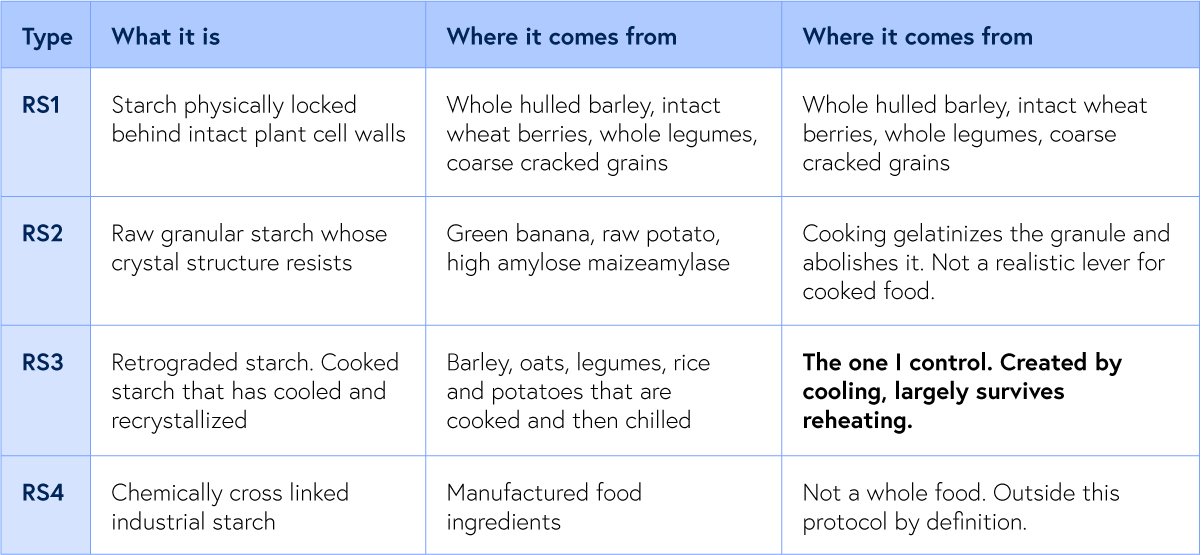
Legumes carry both RS1 and RS3 and are the densest whole food source. Lentils, black beans and chickpeas are already doing this work.
Colonic bacteria convert resistant starch chiefly into butyrate, acetate and propionate. Butyrate is the preferred fuel of the colonocyte and is anti inflammatory locally. Propionate is absorbed into the portal vein and delivered directly to the liver, where the evidence suggests it restrains hepatic cholesterol synthesis. That is the same secondary pathway I described for beta glucan fermentation. Whole hulled barley delivers viscosity and fermentable substrate from a single food, which is why it is the specific grain I am adding to my diet in addition to the steelcut oatmeal that I already eat.
The cook and cool instruction is simple and worth doing precisely. Cook the barley normally, then refrigerate it for at least 12 hours, overnight. As the gelatinized starch cools, amylose chains realign into tight crystalline structures that amylase cannot open, and RS3 forms. The useful part is what happens next. Retrograded amylose has a considerably higher melting temperature than the original gelatinized granule, so ordinary reheating does not undo it. Cook a large batch on Sunday, refrigerate it, and reheat portions through the week. The cooling is the active step and it costs nothing but planning. The same applies to rice, potatoes and legumes, and it is the single easiest glycemic improvement available in a plant based kitchen.
The evidence for resistant starch is strong and consistent for postprandial glucose, insulin sensitivity and colonic health, and it is considerably weaker and less consistent for LDL cholesterol specifically. The 2019 meta analysis by Wang and colleagues found reliable effects on glucose and insulin measures and inconsistent effects on lipids. Typical intake in a Western diet runs 3 to 8 grams daily, while most benefit estimates sit nearer 15 to 20 grams. Treat resistant starch as a glycemic and colonic lever that supports the ApoB work indirectly. It is not a substitute for the 3 gram beta glucan target and it is not a lipid intervention in its own right.
Different Branches Make Different Starches
“Diets high in amylose produced lower glucose and insulin responses than diets high in amylopectin in human subjects.”
Behall, Scholfield and Hallfrisch. American Journal of Clinical Nutrition, 1988.
Starch is one word for two different molecules, and almost everything that matters about a grain metabolically comes down to the ratio between them.
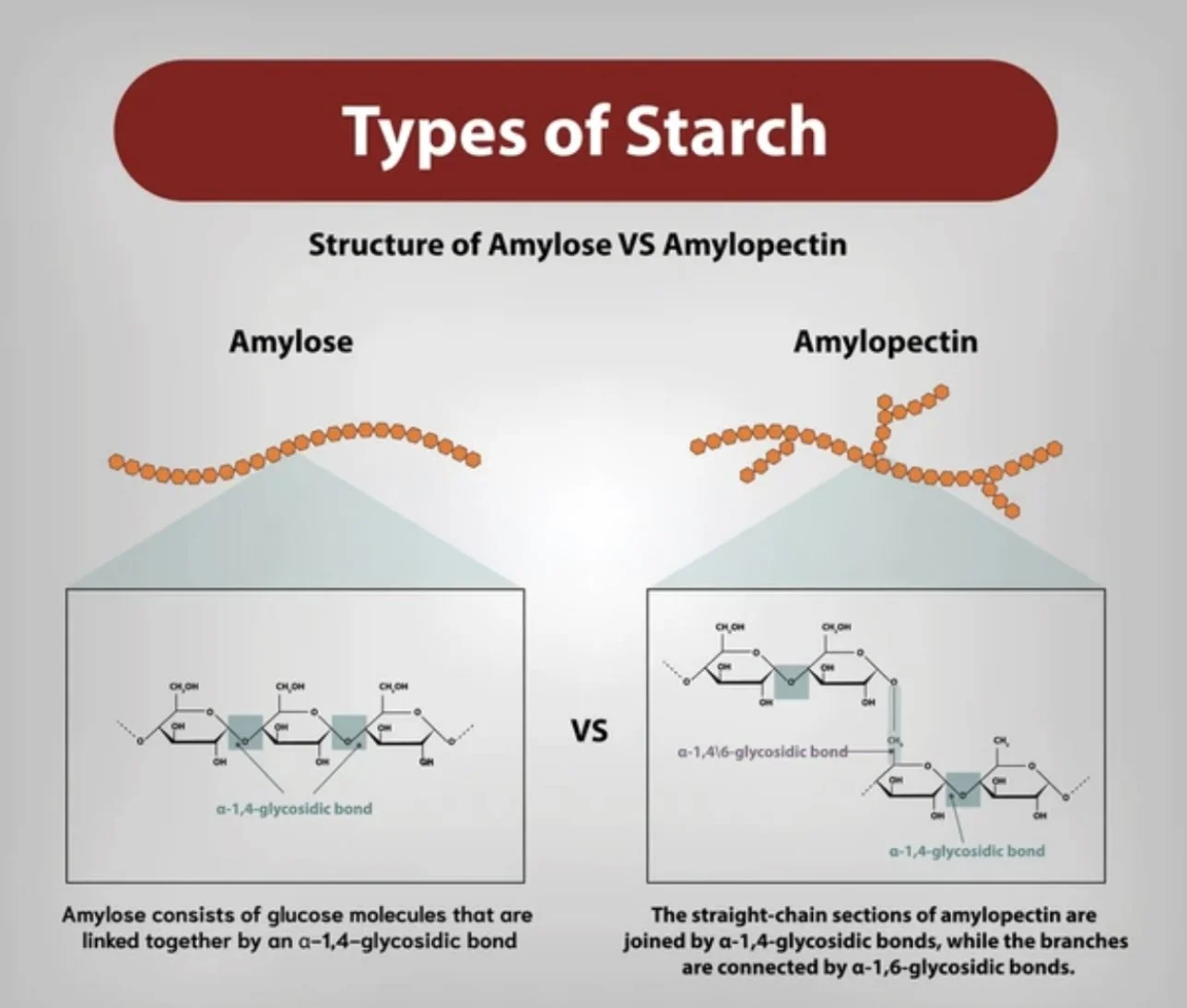
Amylose is a long, essentially linear chain of glucose units joined by alpha 1,4 bonds. It coils into a tight helix, packs closely with its neighbors, and resists the enzymes that want to take it apart. When cooked starch cools, amylose is the fraction that recrystallizes, a process called retrogradation, and the retrograded product is resistant starch type 3, which behaves in the colon more like fiber than like sugar.
Amylopectin is the same glucose backbone with a branch thrown off roughly every 24 to 30 units by an alpha 1,6 bond. Those branches make it enormous, bushy, and unable to pack. It is highly hydrated, gelatinizes readily under heat and water, and it presents a very large number of exposed chain ends. Every branch point creates another free end, and every free end is another site where amylase can begin cutting. Alpha amylase in saliva and pancreatic juice attacks internal alpha 1,4 bonds, and the brush border enzymes finish the job at the ends. A branched molecule is not digested faster because it is somehow weaker. It is digested faster because the enzymes can work on hundreds of sites at once instead of a few.
This is a structural fact with a clinical consequence. Behall and colleagues fed human subjects diets matched for total starch but differing in amylose to amylopectin ratio and found that the high amylose diets produced lower glucose and insulin responses acutely, and in longer feeding studies produced lower total and LDL cholesterol.The same number of grams of starch, arranged differently, produced different lipids.
Table 3 Starch architecture and glycemic behavior

Glycemic index values are population means with wide individual variation, drawn from the international glycemic index tables.
Whole wheat bread and intact wheat berries are chemically the same starch, and they behave 30 glycemic points apart. Nothing was added or removed except structure. This is the single most useful thing I have learned about grains, and it is why the word whole on a bread bag can lead you astray.
From Starch to Atherogenic Particle Count
“Human fatty acid synthesis is stimulated by a eucaloric low fat, high carbohydrate diet.””
Hudgins, Hellerstein, Seidman and colleagues. Journal of Clinical Investigation, 1996.
Very scientific and better illustrated by a diagram, but it makes so much sense to me now 🙂
Here is the bridge between a starch molecule and an ApoB number, and it runs through the liver.
Rapidly digested amylopectin from flour produces a fast, high glucose excursion and a correspondingly sharp insulin response. Insulin does far more than move glucose into cells. In the hepatocyte it activates the transcription factor SREBP-1c, which turns on the enzymes of de novo lipogenesis, chiefly acetyl CoA carboxylase and fatty acid synthase. The liver begins converting surplus carbohydrate into palmitate, esterifies it into triglyceride, packages that triglyceride with apolipoprotein B, and secretes it as very low density lipoprotein (VLDL).
That VLDL does not simply circulate and clear. In the plasma, cholesteryl ester transfer protein (CETP) swaps triglyceride out of VLDL in exchange for cholesteryl esters taken from LDL and HDL particles. The LDL particle that receives triglyceride is then acted on by hepatic lipase, which strips the triglyceride out and leaves behind a smaller, denser particle carrying less cholesterol. HDL undergoes the same exchange and the triglyceride enriched HDL is catabolized faster, which is why HDL falls in this pattern. The result is more particles, each carrying less cholesterol, which is exactly how ApoB can climb while LDL cholesterol looks tolerable.
Small dense LDL particles are also more atherogenic per particle. They penetrate the endothelium more readily, bind more avidly to arterial wall proteoglycans, resist receptor mediated clearance, and oxidize more easily. A drifting ApoB with rising triglycerides is therefore worse than the arithmetic looks, because both the number and the quality of the particles have moved in the wrong direction.
Now the part that a whole food plant based reader needs to sit with. Hudgins, Hellerstein and colleagues showed that a low fat, high carbohydrate diet fed at maintenance calories stimulates hepatic fatty acid synthesis. Cutting fat to under 25 grams a day does not protect me from carbohydrate driven VLDL production. If anything it removes the competing fuel and leaves that pathway more exposed. This is the trap hidden inside a well intentioned Esselstyn diet: the dietary fat lever is already pulled all the way down, so the carbohydrate quality lever is the only one left, and refined flour pulls it hard in the wrong direction. My triglyceride of 103 on a diet with almost no fat in it is not a paradox. It is the predicted outcome.
Fructose deserves a footnote here because it explains my fruit experiment. Fructose entering the liver bypasses phosphofructokinase, the main regulated checkpoint of glycolysis, which means it flows toward lipogenic substrate without the feedback control that glucose is subject to. That is why a large fruit load can raise triglycerides. It is also why I am not going to overcorrect. Fruit arrives with its fructose inside a fiber matrix and a large polyphenol load, and refined flour arrives with neither. The flour goes first. If triglycerides normalize, the berries stay.
What Milling Removes
“Higher intakes of dietary fiber and whole grains were associated with lower all cause and cardiovascular mortality across 185 prospective studies and 58 clinical trials.”
Reynolds, Mann, Cummings and colleagues. The Lancet, 2019.
Milling wheat into white flour removes the bran and the germ, and with them roughly 80 percent of the fiber, most of the magnesium, most of the B vitamins, and essentially all of the phytochemical content. That much is common knowledge and it is why enrichment exists. But the nutrient loss is not the main event metabolically.
The main event is the destruction of the cell wall. In an intact grain, starch granules are packaged inside plant cells whose walls are made of cellulose, arabinoxylan and beta glucan. Digestive enzymes cannot cross an intact cell wall. They have to wait for the wall to be breached mechanically or fermented microbially, and that waiting is what makes an intact grain slow. Milling is not a nutritional subtraction. It is the pre digestion of your food before you eat it.
Particle size compounds it. Enzyme activity happens at surfaces, and grinding a grain into flour increases available surface area by orders of magnitude. Then baking gelatinizes the starch, hydrating and unwinding the granules so the amylopectin is fully accessible. Flour, water and heat is an efficient protocol for making glucose available as fast as the small intestine can absorb it. Adding the bran back afterward, which is what whole wheat flour is, restores some fiber and some minerals. It does not restore the cell walls, and the glycemic index tables show it.
This is where I have to be honest about my own reading of the protocol. I have understood whole food plant based to mean plant based with attention to fat. It also means whole. Bread made from flour is a processed food no matter how many seeds are on the crust, and I have been eating it inside a protocol that formally excludes it while telling myself I was compliant. This is not vague theory, and neither is the mechanism.
The same logic disposes of the walnuts and the olives. It is not that 3 walnuts contain 6 grams of fat, although on a target under 25 grams that is a quarter of the daily allowance going to a food the protocol names specifically. It is that Esselstyn excludes nuts, seeds, avocado and olives from the protocol for patients with established coronary disease on endothelial grounds, and Joe Crowe, whose distal LAD refilled on angiography, was not eating them. I ran an experiment against a protocol whose only documented results come from people who did not run that experiment.
I wish to emulate Dr. Joe Crowe’s remarkable plaque reversal with LDL 38.
The target thresholds are worth stating plainly because they differ. The European and Canadian guidelines for very high risk secondary prevention put LDL under 1.4 or even <1.0 millimoles/L, which is about 55 mg/dl, with ApoB under 65. The American guidance sits near LDL 55 and ApoB 55. The cardiologist I spoke with prefers under 40, which is where Crowe landed. At 71, I am not in reversal territory by any of these standards. I am in maintenance territory at best.
If perfect adherence lands me in the low 50s in September, that is a real result and it is still short of 38. That is the point at which the PCSK9 inhibitor question stops being theoretical and becomes a decision to make with my cardiologist rather than a decision to defer. I would rather arrive at that conversation in September with a clean diet experiment behind me and know exactly what the food can and cannot do, than arrive at it having never run the experiment properly. The purpose of maximal dietary adherence is not only the LDL it produces. It is knowing the true size of the gap that remains.
The Discipline of a Single Change
There is a temptation in self experimentation to change 6 things at once because you want the number to move. It can work but it never truly teaches you the insight required. A year of small additions taught me that lesson in the other direction: I added 4 things gradually, none of them individually alarming, and I cannot now say which one cost me the most. What I can say is that the aggregate cost was 26 points of ApoB and the end of measurable regression.
The prudent sees danger and hides himself, but the simple go on and suffer for it. Proverbs 22:3. The verse is usually read as being about foresight, and it is, but there is something else in it. The simple person is not reckless. He is unobservant. He walks past the same warning repeatedly without registering it. My triglyceride of 103 was a warning. But it took months for me to correct my error.
Barley instead of bread is a small thing. It is a beta 1,3 linkage instead of an alpha 1,6 branch, a viscous gel instead of a gelatinized paste, a cell wall intact instead of a cell wall milled away. But the arteries do not respond to intention, and they do not grade on effort. They respond to the number of ApoB particles arriving at the endothelium, hour after hour, for years. Everything in this issue is an argument about how to make that number smaller and keep it there.
Labs on 4 August. Labs again in early September. I will publish both, including the result I do not want.
A Request
Each Friday, I upload a new Youtube video. Please like, comment and subscribe so I can help many others in your network and beyond, it’s my mission to help people avoid the same fate as Rob, the same fate as I could have had. Heart attack, stroke or sudden death.
https://www.youtube.com/@DrKevinHam
My latest video is going viral :) My #1 meal to unclog arterial plaque. Thank you.
Your Question
A question worth exercising with
For yourself. For someone you love. Answer this question in the quietness of your day.
When will you get the Lp(a) blood test if you haven’t already?
For Someone You Love
There is someone in your life running and falling. You thought of them. Send this to them. Your loved ones just need the information to act and a guide to help them.
Keep going. The race is long, the road is beautiful, and the body was built to heal.
Grace, strength and love to you.
MORE READINGS YOU’LL ENJOY
Health
Reversing My 77% Heart Plaques
Stats Say You Likely Have Heart Plaque
The Healing Power of Food: Nitric Oxide
Meaning
I pray you unlock your heart to reach the height of your full potential by discovering your calling.
Kevin Ham, MD
Appendix:
Studies and Sources
Beta glucan and viscous fiber
Whitehead A, Beck EJ, Tosh S, Wolever TMS. Cholesterol lowering effects of oat beta glucan: a meta analysis of randomized controlled trials. American Journal of Clinical Nutrition. 2014;100(6):1413 to 1421.
Pooled 28 randomized trials. At or above 3 grams of oat beta glucan daily, LDL cholesterol fell by approximately 0.25 mmol/L with no adverse effect on HDL or triglycerides. The trial base for the 3 gram threshold.
Ho HVT, Sievenpiper JL, Zurbau A, et al. The effect of oat beta glucan on LDL cholesterol, non HDL cholesterol and apoB for CVD risk reduction: a systematic review and meta analysis of randomised controlled trials. British Journal of Nutrition. 2016;116(8):1369 to 1382.
Fifty eight trials. Confirmed reductions in LDL and non HDL cholesterol and, importantly, in apolipoprotein B. One of the few fiber meta analyses to report a particle count endpoint.
Ho HVT, Sievenpiper JL, Zurbau A, et al. A systematic review and meta analysis of randomized controlled trials of the effect of barley beta glucan on LDL-C, non HDL-C and apoB for cardiovascular disease risk reduction. European Journal of Clinical Nutrition. 2016;70(11):1239 to 1245.
Fourteen trials of barley specifically. LDL fell approximately 0.25 mmol/L, non HDL approximately 0.32 mmol/L, and apoB approximately 0.15 g/L. The direct evidence for substituting barley for bread.
Wolever TMS, Tosh SM, Gibbs AL, et al. Physicochemical properties of oat beta glucan influence its ability to reduce serum LDL cholesterol in humans: a randomized clinical trial. American Journal of Clinical Nutrition. 2010;92(4):723 to 732.
Demonstrated that high molecular weight beta glucan lowered LDL substantially more than the same gram dose of depolymerized beta glucan. The basis for avoiding instant and extruded products.
Andersson M, Ellegard L, Andersson H. Oat bran stimulates bile acid synthesis within 8 hours as measured by 7 alpha hydroxy 4 cholesten 3 one. American Journal of Clinical Nutrition. 2002;76(5):1111 to 1116.
Direct human demonstration of the bile acid mechanism, showing measurable upregulation of hepatic bile acid synthesis within hours of a single oat bran meal.
Gunness P, Gidley MJ. Mechanisms underlying the cholesterol lowering properties of soluble dietary fibre polysaccharides. Food and Function. 2010;1(2):149 to 155.
Mechanistic review covering viscosity, bile acid sequestration, CYP7A1 upregulation and short chain fatty acid effects. The best single overview of how the pathway fits together.
Behall KM, Scholfield DJ, Hallfrisch J. Lipids significantly reduced by diets containing barley in moderately hypercholesterolemic men. Journal of the American College of Nutrition. 2004;23(1):55 to 62.
Controlled feeding study showing dose responsive reductions in total and LDL cholesterol as barley replaced other grains in the diet.
Starch structure, glycemic load and whole grains
Behall KM, Scholfield DJ, Hallfrisch J. Diets containing high amylose vs amylopectin starch: effects on metabolic variables in human subjects. American Journal of Clinical Nutrition. 1988;47(3):428 to 432.
The foundational human comparison of the two starch architectures at matched total starch intake. High amylose produced lower glucose and insulin responses.
Behall KM, Howe JC. Effect of long term consumption of amylose vs amylopectin starch on metabolic variables in human subjects. American Journal of Clinical Nutrition. 1995;61(2):334 to 340.
Extended the acute finding to a longer feeding period and reported improved lipid outcomes on the high amylose diet. Establishes that starch structure, not starch quantity, moved lipids.
Foster-Powell K, Holt SHA, Brand-Miller JC. International table of glycemic index and glycemic load values: 2002. American Journal of Clinical Nutrition. 2002;76(1):5 to 56.
The reference compilation for the glycemic index values in Table 3, including the gap between intact grains and their milled equivalents.
Reynolds A, Mann J, Cummings J, Winter N, Mete E, Te Morenga L. Carbohydrate quality and human health: a series of systematic reviews and meta analyses. The Lancet. 2019;393(10170):434 to 445.
Commissioned by the World Health Organization. Synthesized 185 prospective studies and 58 clinical trials, finding fiber intake and whole grain intake, not glycemic index alone, most strongly predicted reduced mortality.
Aune D, Keum N, Giovannucci E, et al. Whole grain consumption and risk of cardiovascular disease, cancer, and all cause and cause specific mortality: systematic review and dose response meta analysis of prospective studies. BMJ. 2016;353:i2716.
Dose response evidence for whole grain intake and cardiovascular mortality, with the effect concentrated in genuinely intact grains rather than in products labeled whole grain.
Liu S, Willett WC, Stampfer MJ, et al. A prospective study of dietary glycemic load, carbohydrate intake, and risk of coronary heart disease in US women. American Journal of Clinical Nutrition. 2000;71(6):1455 to 1461.
Nurses Health Study analysis linking high dietary glycemic load to coronary events, with the association strongest among those with higher body mass index.
Resistant starch and colonic fermentation
Englyst HN, Kingman SM, Cummings JH. Classification and measurement of nutritionally important starch fractions. European Journal of Clinical Nutrition. 1992;46 Suppl 2:S33 to S50.
The foundational classification paper defining rapidly digestible, slowly digestible and resistant starch, and establishing the RS1 through RS4 scheme used in Table 2.
Sonia S, Witjaksono F, Ridwan R. Effect of cooling of cooked white rice on resistant starch content and glycemic response. Asia Pacific Journal of Clinical Nutrition. 2015;24(4):620 to 625.
Direct human evidence for the cook and cool instruction. Cooling cooked rice raised resistant starch content and produced a lower glycemic response even after reheating.
Robertson MD, Bickerton AS, Dennis AL, Vidal H, Frayn KN. Insulin sensitizing effects of dietary resistant starch and effects on skeletal muscle and adipose tissue metabolism. American Journal of Clinical Nutrition. 2005;82(3):559 to 567.
Randomized crossover trial showing improved whole body insulin sensitivity after 4 weeks of supplemental resistant starch, with measurable changes in muscle and adipose substrate handling.
Wang Y, Chen J, Song YH, et al. Effects of the resistant starch on glucose, insulin, insulin resistance, and lipid parameters in overweight or obese adults: a systematic review and meta analysis. Nutrition and Diabetes. 2019;9(1):19.
The honest counterweight. Found consistent benefit for glucose and insulin measures and inconsistent, largely non significant effects on LDL and total cholesterol. The basis for not overselling resistant starch as a lipid intervention.
Cummings JH, Pomare EW, Branch WJ, Naylor CPE, Macfarlane GT. Short chain fatty acids in human large intestine, portal, hepatic and venous blood. Gut. 1987;28(10):1221 to 1227.
The classic human study mapping short chain fatty acid concentrations across the portal circulation, establishing that propionate produced in the colon is delivered directly to the liver.
De novo lipogenesis, VLDL and apolipoprotein B
Hudgins LC, Hellerstein M, Seidman C, Neese R, Diakun J, Hirsch J. Human fatty acid synthesis is stimulated by a eucaloric low fat, high carbohydrate diet. Journal of Clinical Investigation. 1996;97(9):2081 to 2091.
Isotopic tracer study demonstrating that hepatic de novo lipogenesis is switched on by a low fat high carbohydrate diet even without excess calories. The essential caveat for anyone running an ultra low fat protocol.
Parks EJ, Hellerstein MK. Carbohydrate induced hypertriacylglycerolemia: historical perspective and review of biological mechanisms. American Journal of Clinical Nutrition. 2000;71(2):412 to 433.
The definitive review of how carbohydrate load raises triglycerides through hepatic VLDL overproduction, and why the effect depends on carbohydrate type and on the time course of adaptation.
Sniderman AD, Thanassoulis G, Glavinovic T, et al. Apolipoprotein B particles and cardiovascular disease: a narrative review. JAMA Cardiology. 2019;4(12):1287 to 1295.
The case for apoB as the primary measure of atherogenic risk, superior to LDL cholesterol when the two diverge. Directly relevant to reading a drifting apoB against a stable LDL.
Ference BA, Ginsberg HN, Graham I, et al. Low density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. European Heart Journal. 2017;38(32):2459 to 2472.
European Atherosclerosis Society consensus establishing causality and the cumulative exposure model: the burden is particle concentration multiplied by years of exposure.
Jenkins DJA, Jones PJH, Lamarche B, et al. Effect of a dietary portfolio of cholesterol lowering foods given at 2 levels of intensity of dietary advice on serum lipids in hyperlipidemia: a randomized controlled trial. JAMA. 2011;306(8):831 to 839.
Demonstrated that combining viscous fiber, plant sterols, soy protein and nuts produced LDL reductions substantially larger than any single component. The precedent for stacking dietary levers.
Clinical protocol and lipid targets
Esselstyn CB Jr. Prevent and Reverse Heart Disease. Avery, 2007.
Source of the Joe Crowe angiographic sequence and of the protocol excluding all added oil, nuts, seeds, avocado and olives for patients with established coronary disease.
Esselstyn CB Jr, Gendy G, Doyle J, Golubic M, Roizen MF. A way to reverse CAD? Journal of Family Practice. 2014;63(7):356 to 364b.
Follow up of 198 consecutive patients with established cardiovascular disease counseled on a whole food plant based diet. Adherent patients had a markedly lower rate of subsequent events than non adherent patients.
Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias. European Heart Journal. 2020;41(1):111 to 188.
Source of the European very high risk targets of LDL under 1.4 mmol/L and apoB under 65 mg/dL, and of the recommendation for at least a 50 percent reduction from baseline.
Pearson GJ, Thanassoulis G, Anderson TJ, et al. 2021 Canadian Cardiovascular Society Guidelines for the Management of Dyslipidemia. Canadian Journal of Cardiology. 2021;37(8):1129 to 1150.
Canadian thresholds, including the endorsement of apoB as an alternative primary target rather than a secondary measure.
Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC Guideline on the Management of Blood Cholesterol. Circulation. 2019;139(25):e1082 to e1143.
Source of the American thresholds referenced in the text, including the LDL 70 mg/dL threshold for intensification in secondary prevention.
This issue describes a single physician's self experiment and the published evidence behind it. It is not medical advice. Decisions about lipid lowering therapy, dietary protocols and imaging surveillance belong in a conversation with your own physician.
Subscribe to my Compounding Wisdom newsletter and start transforming your life. ham.com
Subscribe to my YouTube channel @DrKevinHamfor videos on how I reversed my clogged arteries in 3 months, the top foods that clear your arteries, and the first principles of health that can save your life. Like, share and subscribe — it could save the life of someone you love.
The Silent Golden Hour
Why sleep builds or dissolves plaque while you sleep
Why sleep builds or dissolves plaque while you sleep
One hour can be life or death
Dr. Kevin Ham, MD
I hosted 54 Ham relatives from 7 cities and three countries last week. It was so touching to have four generations of Hams in one place. We spoke from the heart, each of us asked to give their life moments, their experience of this gathering and their life dreams. From my 90 year old father to his four siblings, 88, 86, 83, 74, I was so touched hearing how they struggled through poverty. My oldest aunt was 78 before she was taught to read Korean at her church. That was mind blowing for me to hear. My cousin said he never ate white rice until he was 19. My uncle and his wife had little education. Somehow my father had the courage to venture out of his small hometown of just under 1400 people to a larger village to be trained as a miner. He then got a lottery selection to go to Germany as a miner and for three years worked deep in the mines and watched his fellow miners die from accidents. He decided he needed another job and found his way to Canada, London Ontario and got a job at the Ford factory there. London was where I was born in 1970. My older cousin became an engineer and ended up getting a job in a managerial position at the same Ford factory in London, where he met some of my father’s coworkers from long ago. I went to London to do my medical residency for two years and my daughter was born there. I realized that life is not only a linear story but also circular.
I realized last year after visiting my Ham relatives in my father’s home region, where 20 of us gathered, that time was passing so quickly and so I had an idea to invite all my direct Ham relatives to Vancouver and host them. It would be a once in a lifetime event as many of them are older and reunite my aunts, uncle and father in their old age. My uncle in Toronto had only seen his sister once in 70 years! My father left Korea in 1965. Through God’s grace, and our collective hearts, the Ham gathering was so heart touching and endearing. Each of us touched one another’s hearts and we are eternally grateful for this experience to live, sleep, travel together to Whistler, Victoria and most of all at a camp where we spent three days fully together. I hope each of you reading will have the opportunity to do this with your families and extended families.
I gave a special ad hoc talk on health and how to prevent and reverse heart disease, stroke, cancer and our common metabolic diseases including cancer (gallbladder) which my mom perished from in 2006 at age 68. I asked my older aunts to read the Bible and find the secrets of life within it.
But I am now in Kauai for two weeks, focused on my sleep. I realized that high LDL in the past (186 mg/dL or 4.33 mM) was not my only risk factor. After researching sleep, I realized lack of sleep is an independent risk factor for heart attacks. I knew this but didn’t realize the severe impact it has played in my life.
Since I was a teenager, I didn’t sleep a lot. 4-6 hours. Med school didn’t help while holding three jobs to pay for med school plus helping my father’s dry cleaning businesses. After my carotid plaque reversed, I went back to my old ways of being extremely busy, full of stress and so when I opened my eyes, as a light sleeper, my brain would be thinking of all the things I needed to do. I would average under 6 hours of sleep.
Here is a log of my total sleep, deep sleep and REM in the last two weeks.
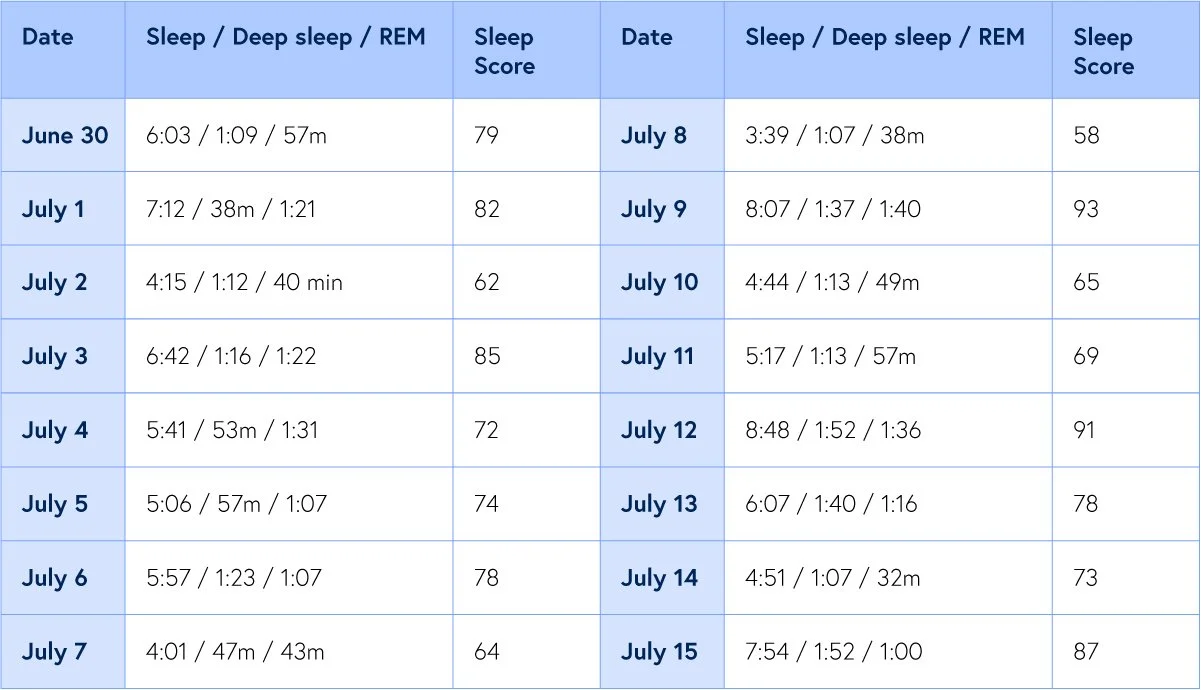
My Sleep Data (Oura ring)
July 3-13 is when my relatives came. July 14 is when I travelled. Today I slept 8:37 with 1:38 of deep sleep and 1:33 of REM. My sleep score? An astounding 94 (only my third time cracking the 90+ score on my Oura ring in six months).
Deep sleep is when the body restores and rejuvenates. REM is when the mind, subsconscious make sense of the world. Heart rate variability is another measure to look at but that’s another topic. My goal is a sleep score above 80, sleep more than 7 hours and 1 hour+ deep sleep and REM.
Let’s dive into how important sleep is to heart disease (and almost any disease including cancer, autoimmune, metabolic disease and psychosocial).
The Golden Lost Hour
“One hour shorter or longer is the chasm between life and death.”
Dr. Kevin Ham
Twice a year, without a consent form or a control group, an entire nation runs a medical experiment on itself. In spring we push the clocks forward and quietly rob 300 million people of a single hour of sleep. The Monday that follows, emergency rooms see more heart attacks. In autumn we hand the hour back, and heart attacks fall. Same people, same diets, same cholesterol, same medications, same everything. The only variable that moved was 1 hour of sleep.
That so slight a thing can tilt so grave an outcome should unsettle us, because it exposes a blind spot the clinic has been slow to admit. We measure cholesterol to the decimal and counsel against tobacco with something close to religious zeal, yet we have long treated sleep as a luxury rather than a lever. It is time to correct the ledger. Sleep is one of the most powerful cardiac interventions you will ever have, and it is free.
We are perhaps the first generation to treat the night as negotiable. The electric bulb, the glowing screen, the always-open economy, each has taught us to borrow against the dark as though it were interest-free. It is not. The arteries keep the account, and they charge, patiently, in plaque.
The Reward We Mistook for a Cause
“The shorter your sleep, the shorter your life span.”
Matthew Walker, Why We Sleep
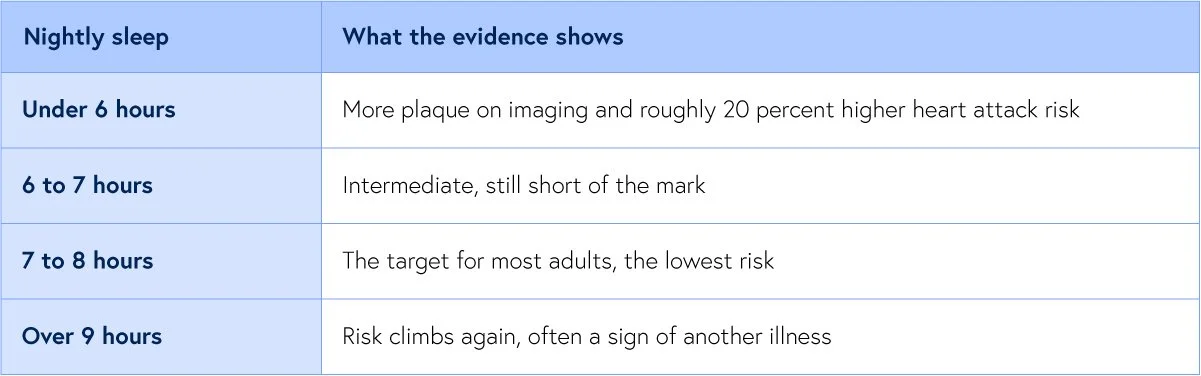
For most of the modern era we regarded sleep as the reward for a healthy life rather than a cause of one. The evidence has since inverted that belief. The most careful look came from the PESA study, where investigators fitted nearly 4,000 healthy middle-aged adults with motion trackers for 7 nights, measuring not what people claimed but what their bodies actually did, and then imaged their arteries from the neck to the groin. They sorted the sleepers into 4 groups: under 6 hours, 6 to 7, a reference band of 7 to 8, and over 8. The result was sobering. Those sleeping under 6 hours carried roughly 30 percent higher odds of the heaviest plaque burden in the body, and the association survived every adjustment for the usual suspects, the cholesterol and the blood pressure and the rest.
One detail deserves a second look, because it overturns a common comfort. The extra plaque in the short sleepers appeared on ultrasound even when their coronary calcium score read a reassuring zero. A calcium score of zero is widely taken as an all clear. In these men and women it was nothing of the kind. Short sleep was laying down the soft, young, rupture-prone plaque that calcium scans cannot see, the very kind that kills before it ever turns to stone.
Nor is more sleep simply better. Both ends of the spectrum carry risk, a shallow U whose floor sits at 7 to 8 hours of true sleep for most adults. Below 6, plaque and events climb. Beyond 9, risk rises again, though there the long sleep tends to be the shadow of some other illness rather than its author. The number to aim for is not heroic. It is ordinary, and most of us miss it: more than a third of adults routinely sleep less than the 7 hours the heart asks for, which makes this not a fringe risk but a mass exposure, quietly shaping the arteries of tens of millions who believe themselves well.
The Sleep Ladder
I wonder whether 7 nights to assess the cardiac plaque is adequate and wondered what a longer term study would show after a month or three months but realize that this is a study that an Oura ring or other study could possibly be used to conduct and then do serial measures of carotid artery ultrasounds or even coronary arteries by CT with contrast after six months and a year.
What the Night Builds
“If sleep does not serve an absolutely vital function, then it is the biggest mistake the evolutionary process has ever made.”
Allan Rechtschaffen
Why should the hours you spend unconscious reach into the wall of an artery at all? The most elegant answer came from a laboratory, where researchers broke the sleep of mice night after night and watched their plaques grow. Tracing the chain backward, they found its first link in the brain. Fragmented sleep lowered a signal called hypocretin, made in the hypothalamus, and the fall in hypocretin instructed the bone marrow to release a flood of inflammatory white cells, the very monocytes that infiltrate the artery wall and build plaque. More broken nights meant more of these cells, and larger lesions. And their cholesterol never moved.
That last fact is the heart of the matter, and it answers a question I am asked often. Can plaque still advance when your LDL is low and your inflammation looks quiet? It can. Sleep does not build plaque by raising your cholesterol; it builds it through the brain and the marrow, along a road that runs parallel to LDL and independent of it. You can do everything right on the lipid panel and still lose ground in the artery if you are stealing from sleep.
In the human body the insults stack higher still. Deprived of sleep, your blood pressure fails to dip at night as it should, your stress nervous system stays switched on, cortisol runs high, blood sugar control frays, and the smooth lining of your vessels loses its ability to relax. And sleep loss lights the same fire we track in the blood: restrict healthy adults to 4 hours in bed for a few nights and their C-reactive protein climbs. So short sleep is not a single risk factor in one disguise. It is a whole cascade, pulling blood pressure, blood sugar, and inflammation in the wrong direction at once.
The metabolic toll compounds the vascular one. A short night loosens insulin control of blood sugar within days, and it scrambles the hormones of appetite, lowering the satiety signal leptin and raising the hunger signal ghrelin, so the sleep-starved eat more and store it, preferentially, as the deep visceral fat that is itself an engine of inflammation. Sleep loss thus feeds the very fire it also ignites, and the two tighten into a loop across the years.
A brief warning here, since many who read this letter also fast. A fast is a mild stress, and it raises cortisol; short sleep raises cortisol too, and lifts inflammation on its own. Layer a fast upon a poor night and you gather all the strain of both with the reward of neither. Fast on your rested days, never on your ragged ones.
These are the cascading effects of lifestyle decisions and I have realized that the right strategies require careful thought and consideration. I’m focused on sleep above 7 hours and removing stress by a default “No, sorry I can’t at this time.” and removing white flour from my diet when I travel. Mostly greens and beans with some fruits and some whole grains.
The Proof in the Clocks and the Genes
“Unhealthy sleep, unhealthy heart.”
Matthew Walker, Why We Sleep
Return to that twice-yearly experiment, because it remains the cleanest natural proof we own. When researchers in Michigan counted heart attacks around the clock changes, the Monday after the spring shift, when the hour is stolen, brought about a 24 percent rise, some 8 additional heart attacks in a single hospital system in a single day. The Tuesday after the autumn shift, when the hour is returned, brought about a 21 percent fall. And here is the tell that rules out coincidence: the total across the whole week did not change. The lost hour did not manufacture new disease. It shoved the already-vulnerable over the edge a little sooner, and the gift of an hour drew a few of them back.
Why should a solitary hour affect the heart so much? The likeliest answer is timing rather than mere quantity. The spring shift does not only shorten sleep; it wrenches the body internal clock out of step with the external one, and that misalignment sends a surge of stress hormones and a rise in blood pressure through the vulnerable early morning, exactly when heart attacks already gather.
This is not an aberration of just one city. Swedish national records, spanning an entire country, show the same spring spike in the first days after the change. More recent data from Indiana find heart attacks elevated for roughly 2 full weeks after the spring transition. Different populations, different decades, one recurring signature: sleep.
But does too little sleep cause heart attacks, or merely travel in bad company? To settle it, researchers turned to nearly half a million adults and used the genes people are born with as a natural experiment, a design that can separate cause from mere association. The arrow pointed at cause. Short sleepers carried about 20 percent higher risk of a heart attack, and the effect held even when nothing else was amiss. Then came the line that should change how you think forever: a healthy sleep duration lowered heart attack risk even among those dealt the very worst genetic hand for heart disease. You cannot choose your DNA. You can choose your bedtime, and your bedtime determines the result.
Where Sleep Sits Among the Giants
How heavy is this lever, set beside the giants of heart disease factors? Honesty requires proportion. Pooling nearly half a million people, short sleep raised the risk of developing or dying of coronary disease by about 48 percent. That is real and it is meaningful, but it is not the magnitude of smoking, which roughly triples the odds of a heart attack, nor of a lifetime of high apolipoprotein B, which by the best global estimates underlies nearly half of all first heart attacks. Sleep belongs in the second rank of cardiac risk, a genuine and modifiable hazard rather than the single largest one.
Yet its rank understates its reach, for two reasons. Much of sleep harm is delivered through the very giants it stands beside, worsening blood pressure, blood sugar, weight, and inflammation, so that mending sleep quietly improves them all at once. And unlike your age or your genes, sleep is a lever you take hold of every single night. In 2022 the American Heart Association formally added sleep duration to its 8 essential measures of cardiovascular health, seating it beside cholesterol and blood pressure, because the weight of evidence had at last earned it the chair.
There is a further reason to take it seriously. Unlike C-reactive protein, which predicts disease powerfully yet appears to be more a marker than a cause, the genetic evidence marks short sleep as a genuine cause of heart attacks. That distinction matters, because a cause is worth changing, and this one begins to change tonight.
Which raises the question I am asked most by the health-conscious. What if sleep is the one thing I get wrong, my diet clean and my numbers pristine, but my nights only 5 hours? The data are unsentimental. Short sleep raised risk even after every other factor was stripped away, so a single broken habit is enough to bend the curve. The consolation rides beside the warning: because sleep is causal, and because it is yours to command, repairing it pays back even a person who has done everything else right.
This is my biggest risk factor and has been for decades. It explains why my wife’s calcium score is 0, my younger brother who I grew up with has a calcium score of just 7. I am in the 96% percentile for my age for calcium score. Not a good thing. I am very high risk. So I need to focus heavily on sleep and stress. Hence the reason I came to Kauai instead of going to Korea for my annual summer Bible pilgrimage, where I would get little sleep, have jet lag and meet a lot of people. I had to weigh the consequences on my heart vessels.
The Ladder, the Apnea, and the Prescription
“Why had I not heard of Vitamin K2 until ten years ago? Dr. Weston Price called it Factor X. How many other marvelous things do I yet not know?”
Dr. Kevin Ham
Duration is only half the story; quality is the other. Fragmented sleep injured the arteries in PESA even when the total hours looked adequate, and the clinic sees the same pattern in its patients. Difficulty falling asleep raises cardiovascular risk by roughly a fifth; unrefreshing sleep and trouble staying asleep carry their own smaller penalties. A night in bed is not the same as a night asleep.
The numbers put colour on this. In pooled studies, nonrestful sleep carried about a 16 percent higher cardiovascular risk, difficulty staying asleep about 14 percent, and difficulty falling asleep about 22 percent. None of these makes a headline, yet layered across decades and across a whole population they sum to a great deal of disease that a better night would have prevented.
I have very little sleep latency and fall asleep easily. Likely because I am already tired and also my exercise routines. But I do get up at night and oftentimes have a hard time falling back asleep. I’ve also doubled to tripled the amount of deep sleep I get. I have some hacks that have shown this consistently but this also is another newsletter topic.
The clock also cares about consistency as much as quantity. Newer work suggests that an irregular schedule, the bedtime that wanders by hours from one night to the next, predicts cardiovascular trouble on its own, apart from how long you sleep. The body is a creature of rhythm, and it pays a tax on chaos.
And there is a thief of quality that hides in plain sight: obstructive sleep apnea, in which the airway collapses and breathing stops dozens of times an hour, all night, every night. It is broken sleep and starved oxygen in the same stroke, and it drives high blood pressure, atrial fibrillation, and coronary disease. Its prevalence among people who carry those very conditions runs as high as 40 to 80 percent, and far too much of it goes undiagnosed. If you snore, gasp, wake unrefreshed, or carry stubborn high blood pressure or a fib, be tested. Treating apnea may be the single highest-yield sleep intervention a cardiac patient can make.
The prescription, then, writes itself, and none of it is exotic. Aim for 7 to 8 hours actually asleep, which means a little more than that in bed. Hold a steady wake time, weekends included, because regularity may matter as much as duration. Court morning light, keep the bedroom cool and dark, and move alcohol well away from bedtime, since it is among the most reliable fragmenters of sleep there is. And around the spring clock change, protect that vulnerable week by shifting your bedtime earlier for several nights, so you do not hand your heart the lost hour all at once.
I’ve added dark out curtains instead of just blinds in the bedroom. A very dark room and not too hot enables better sleep.
Guarding the Night
Measure it, too, because what is tracked improves. A wearable that estimates your sleep and your resting heart rate will not be perfect, but it will tell you the truth your memory flatters over: how often the night is broken, how the late glass of wine shortens deep sleep, how a hard block of training or a bright screen delays it. The number on the band is a mirror, and mirrors change behavior.
I am trying to guard my own sleep the way I guard a hard training session, because I have come to see them as the same discipline. Every night the wall of every artery is being either built or cleared, and while I sleep that ledger is being written without me. I have failed to protect my sleep and in the first few months, when I did, I saw a huge payoff, but in the last year, as I let sleep fall, its affected both my mental and physical resilience. I am back on track, learning the life lessons through experience rather than wisdom.
So I urge you to protect your sleep. Not because a physician instructs you to, but because the quietest hours you will ever spend are doing the loudest work you will ever ask of your body and your mind. Sleep long enough, sleep deeply enough, and sleep on a schedule, and let the mending that only darkness permits do, one night upon the next, what no pill can fully replace.
A Request
Each Friday, I upload a new YouTube video. Please like, comment and subscribe so I can help many others in your network and beyond. It’s my mission to help people avoid the same fate as Rob, the same fate as I could have had. Heart attack, stroke or sudden death.
https://www.youtube.com/@DrKevinHam
During the summer, I am only writing two newsletters a month and posting one video a week. I find it is a great cadence for myself. How is this cadence for you?
What to Start Now
Set some rules for your sleep. Bedtime, presleep routine, wake up, hours in bed, target sleep hours.
Get things off your plate that cause you the most stress. How can you do that?
Default to the important and urgent matters and be okay with the sandwich matters of life to settle.
A Question & Action For This Week
Questions worth exercising with
For yourself. For someone you love. Answer this question in the quietness of your day.
What changes will you do to ensure a consistent night of deep rejuvenating sleep? Let me know. Especially if you are great at sleeping.
For Someone You Love
There is someone in your life running and falling. You thought of them. Send this to them. Your loved ones just need the information to act and a guide to help them.
Keep going. The race is long, the road is beautiful, and the body was built to heal.
MORE READINGS YOU’LL ENJOY
Health
Reversing My 77% Heart Plaques
Stats Say You Likely Have Heart Plaque
The Healing Power of Food: Nitric Oxide
Meaning
I pray you unlock your heart to reach the height of your full potential by discovering your calling.
Kevin Ham, MD
Appendix: Sources
Dominguez F, Fuster V, et al. Sleep Duration and Quality With Subclinical Atherosclerosis (PESA). J Am Coll Cardiol 2019;73:134.
In nearly 4,000 adults measured by actigraphy, sleeping under 6 hours or fragmented sleep was independently linked to more atherosclerotic plaque, present even when the calcium score was zero.
https://www.jacc.org/doi/10.1016/j.jacc.2018.10.060
McAlpine CS, et al. Sleep modulates haematopoiesis and protects against atherosclerosis. Nature 2019;566:383.
Fragmented sleep lowered brain hypocretin, drove the marrow to release inflammatory cells, and grew larger plaques in mice, with no change in cholesterol.
https://www.nature.com/articles/s41586-019-0948-2
Cappuccio FP, et al. Sleep duration predicts cardiovascular outcomes: a systematic review and meta-analysis. Eur Heart J 2011;32:1484.
Pooling about 475,000 people, short sleep raised coronary heart disease risk about 48 percent, and long sleep about 38 percent, a U-shaped relationship.
https://academic.oup.com/eurheartj/article/32/12/1484/502022
Daghlas I, et al. Sleep Duration and Myocardial Infarction. J Am Coll Cardiol 2019;74:1304.
In 461,347 adults, short sleep raised heart attack risk about 20 percent, genetic analysis supported cause, and healthy sleep lowered risk even at the highest genetic risk.
https://www.jacc.org/doi/10.1016/j.jacc.2019.07.022
Sandhu A, et al. Daylight savings time and myocardial infarction. Open Heart 2014 (ACC report).
Heart attacks rose about 24 percent the Monday after springing forward and fell about 21 percent the Tuesday after falling back, with the weekly total unchanged.
https://www.acc.org/About-ACC/Press-Releases/2014/03/29/09/16/Sandhu-Daylight-Saving
Janszky I, Ljung R. Shifts to and from Daylight Saving Time and Incidence of Myocardial Infarction. N Engl J Med 2008;359:1966.
Swedish national data showed heart attacks increased in the first days after springing forward and decreased after falling back.
https://www.nejm.org/doi/full/10.1056/NEJMc0807104
Sleep and Cardiovascular Health. American College of Cardiology, 2025.
A clinical review linking short sleep, insomnia symptoms, and obstructive sleep apnea to hypertension, atrial fibrillation, and coronary disease.
Redefining Cardiovascular Health to Include Sleep (MESA Sleep Study). J Am Heart Assoc 2022.
Support for sleep as an eighth pillar of cardiovascular health, consistent with the American Heart Association adding sleep duration in 2022.
https://www.ahajournals.org/doi/10.1161/JAHA.122.025252
Subscribe to my Compounding Wisdom newsletter and start transforming your life. ham.com
Subscribe to my YouTube channel @DrKevinHamfor videos on how I reversed my clogged arteries in 3 months, the top foods that clear your arteries, and the first principles of health that can save your life. Like, share and subscribe — it could save the life of someone you love.
Can Vitamins Reverse Plaque?
A field guide to 6 vitamins and the human heart, Vitamin C, D, K2, Niacin, E, and A
A field guide to 6 vitamins and the human heart, Vitamin C, D, K2, Niacin, E, and A, with the studies, the doses, and the one rule that separates hope from hype.
Dr. Kevin Ham, MD
“The first principle is that you must not fool yourself.”
Richard Feynman, physicist
The Artery That Lost Its Weight
“Eat food. Not too much. Mostly plants.”
Michael Pollan, In Defense of Food
A year ago a machine handed my heart a number, a coronary calcium score of 505. It is the mineral residue of decades, an artery quietly turning to stone, and in everything my training taught me it is supposed to do only one thing across a life. Climb.
Three months later an ultrasound of my neck showed something my education had filed under impossible. My carotid plaque had measurably regressed. Not slowed. Moved backward. I had changed how I ate, how I moved, and how I fasted, and the arteries started letting go of its plaques..
Which raises the question that now follows me everywhere. If plaque can move backward, what moves it? And close behind, the one that fills supplement bottles, can a vitamin do it? This week I read the human and animal evidence on six, vitamin C, D, K2, and niacin, plus the two you asked me to add, vitamin E and vitamin A. I read the trials and the mouse and guinea pig studies until a pattern surfaced, and the pattern is more useful than either the believers or the cynics will admit. Some of what you have been told is real science, and some is hope wearing a lab coat.
Two Kinds of Truth
“Seek truth and nothing but the truth with wisdom and understanding. So help me God.”
Dr. Kevin Ham
One idea makes the rest legible, and most of the supplement industry survives on the confusion around it. There are two completely different kinds of evidence in this field. The first is a surrogate marker, a photograph of the artery, the thickness of the wall on ultrasound, the calcium on a CT scan, and pictures can be coaxed into looking better across a year or two, which is why nearly every vitamin study measures them. The second is a hard outcome, the only thing that has ever truly mattered to a living person, the heart attack that never came, the stroke that never arrived, the grandchild you met because you were still here to meet them.
Here’s the trap, and a famous vitamin is about to fall into it. A treatment can make the photograph prettier and do nothing for the person holding it, or even harm them somewhere the camera was not pointed. So every time you hear that something reverses plaque, ask the second question. Reversed it on a scan, or kept a human being alive and whole?
How Vitamins Travel and Where It Originates
“I find the idea of vitamins fascinating but like a cloud ephemeral and transient.”
Dr. Kevin Ham
Two facts about each vitamin keep returning. The first is whether it dissolves in water or in fat, because water soluble vitamins flush away while fat soluble vitamins accumulate, and accumulation is where the danger of overdose lives. The second is whether your body can make the vitamin at all, or whether you depend on the outside world to supply it (termed essential vitamin). The full chemistry, the chemical formulas, the doses, and the food amounts sit in the field guide tables at the end.
Vitamin C, the Architecture of the Wall
“Discovery consists of seeing what everybody has seen and thinking what nobody has thought.”
Albert Szent-Gyorgyi, who isolated vitamin C and won the Nobel Prize
Vitamin C, ascorbic acid, C6H8O6, begins with a humbling fact. You cannot make it, and so you must eat it. The gene for the final enzyme broke somewhere in our past, and we have carried the ruin since. The guinea pig and the fruit bat share the defect, which is why they become the witnesses in vitamin C's trial. It is water soluble, so you need a fresh supply often, and you get it from bright plants.
Inside an artery it does two things. It is the required cofactor for the enzymes that build collagen, the protein the vessel wall is made of, so deficiency leaves the wall fragile and prone to leak. And it is a frontline antioxidant that shields LDL from the oxidation that turns it dangerous, while helping the vessel lining make nitric oxide, the molecule that keeps an artery open.
Severe deficiency is scurvy, the terror of the old sailing fleets, a body coming apart at the seams, bleeding gums, wounds that will not close, and blood vessels that grow fragile and weep. Half a century ago, guinea pigs made scorbutic grew arterial lesions that looked under the microscope almost indistinguishable from atherosclerosis, and feeding them ascorbate (Vitamin C) healed those lesions. That single old observation is the seed from which this whole question grew.
So does extra vitamin C reverse plaque in people? Honestly, no. Vitamin C from food is linked to slower thickening, not reversal. The ASAP trial slowed carotid thickening by about a third in men, and population data tie higher intake to thinner walls. But the finding nobody quotes keeps me honest. In the Los Angeles Atherosclerosis Study, vitamin C from supplements was tied to faster thickening, dose by dose, while vitamin C from food was not. An orange and a pill are not the same object.
The animal evidence is cleaner. Mice and guinea pigs deprived of vitamin C grow more plaque, and crucially more unstable plaque, the kind that ruptures and kills, and vitamin C protects guinea pigs from the arterial injury of cigarette smoke. Low vitamin C makes atherosclerosis worse. What does not survive into humans is the claim that piling extra on top of sufficiency pulls plaque back out. Bottom line, never be deficient, take it from plants and not a jar, and leave the megadose alone.
Vitamin D, the Hormone You Build From Light
“The dose makes the poison.”
Paracelsus, founder of toxicology
Vitamin D, cholecalciferol, C27H44O, is barely a vitamin. It is fat soluble and really a prohormone your skin makes when ultraviolet light strikes a cholesterol like molecule, after which the liver and kidney finish the job. So your body makes it, but only with sunlight, which is why deficiency haunts winter, high latitudes, the indoor life, and darker skin. This is the one vitamin where the plant eater genuinely struggles, since plants carry almost none. Sunlight is the real source, with ultraviolet exposed mushrooms and fortified foods a distant second. The requirement is 600 international units, 800 after 70, and the safe ceiling is 4,000.
The mechanism is almost too good. Vitamin D receptors sit on nearly every cell involved in atherosclerosis, calming inflammation, supporting the vessel lining, steering the immune traffic toward the calming, regulatory cells. And deficient people do carry more plaque, consistently. But association is a trickster. Low vitamin D may be the shadow of an unhealthy life rather than its cause, a symptom rather than an origin.
So we ran the experiment, and the result was deflating. The large trials are clearly negative. VITAL, with about 25,000 people, found no reduction in heart attacks or strokes, ViDA found nothing, and pooling 134,000 across 29 trials the verdict holds. Correcting a real deficiency is good medicine. Expecting the supplement to reverse plaque is not. The animal work adds a warning, in mouse arteries both too little and too much vitamin D increased calcification. The relationship is a U, not a slope, and more is not better.
The bottom line is moderation in the exact, Paracelsian sense. Fix a genuine deficiency, aim for a healthy level, get honest sun, and do not megadose. Vitamin D is a foundation nutrient your body was built to make, not a drug that dissolves plaque. It points straight at the next vitamin, because what decides where all that calcium goes is vitamin K2.
Vitamin K2, the Traffic Controller of Calcium
“Why had I not heard of Vitamin K2 until ten years ago? Dr. Weston Price called it Factor X. How many other marvelous things do I yet not know?”
Dr. Kevin Ham
K2 is fat soluble, and your body makes it only partly, from gut bacteria and by converting K1. And here is the distinction at the heart of the confusion. Vitamin K1 and vitamin K2 are not the same vitamin.
K1, phylloquinone, C31H46O2, is the form in leafy greens, and the liver grabs most of it to run blood clotting, absorbing only 10 to 15 percent.
K2, the menaquinones, includes MK-4, which is short lived, and MK-7, C46H64O2, the form in natto that lingers for days and reaches the arteries and bones. That long reach is why fermented foods, not your salad, are the practical source of the K2 your arteries use. Among plants, natto is essentially the only rich source, and there is no separate requirement for K2, only a general vitamin K target near 120 micrograms for men and 90 for women.
The mechanism is the most elegant of all. K2 switches on Matrix Gla Protein, the most powerful natural inhibitor of arterial calcification you possess. Active, it escorts calcium out of the artery wall and locks it into bone. Absent, calcium drifts unsupervised into the vessel. This is the eerie calcium paradox, fragile bones and stiff arteries at the same time. The proof is a drug. Warfarin, the common blood thinner, blocks vitamin K, and long term warfarin users show measurably more arterial calcification. Block vitamin K, and arteries harden.
And here is the closest thing to plaque reversing before our eyes. In a landmark 2007 rat study, scientists first drove calcification into the arteries, then fed a diet rich in vitamin K, and the calcification regressed, the mineral leaving the wall, the vessels regaining elasticity, reversing a process we were taught was a one way street.
For actual reversal of calcification, K2 holds the strongest preclinical evidence here. But in humans the dream has only partly come true. The Rotterdam study linked high K2 intake to less heart disease and less aortic calcification, while K1 showed no such link. Yet the randomized trials, using MK-7 around 180 micrograms a day, mostly improved the biomarker without significantly slowing coronary calcium, though a 2025 trial was more hopeful.
So K2 is, of all these, the most biologically promising for calcification and the least proven in people. Eat fermented foods, and if you take vitamin D, pair it with K2, since vitamin D raises the calcium in circulation and K2 decides whether it builds your bones or your blockages. And do not touch supplemental vitamin K with a blood thinner without your doctor, because the same biology that protects your arteries can quietly undo your medication.
Niacin, the Cautionary Tale
“Extraordinary claims require extraordinary evidence.”
Carl Sagan, astronomer
Niacin, vitamin B3, nicotinic acid, C6H5NO2, is the most important lesson here, because it is where the prettier picture trap snaps shut. It is water soluble, and you make some from tryptophan, so food covers your need easily, and its deficiency disease, pellagra, is a nutritional disorder, not a plaque disorder. But the niacin meant to fight heart disease was never the vitamin. It was the drug, dosed at 1,000 to 2,000 milligrams, hundreds of times the requirement. At that altitude it is a pharmaceutical, with a pharmaceutical's power to harm.
At drug doses it does everything you would want, lowering LDL, triglycerides, and lipoprotein little a, raising HDL more than any other agent, calming inflammation. And on the scans it delivered. Combined with a statin, niacin shrank coronary narrowings in the FATS, HATS, and CLAS trials and reversed carotid thickening in the ARBITER studies. If I stopped here you would buy niacin tonight. So remember Sagan. Extraordinary claims demand that we look at the outcome, not the image.
Medicine looked, and the picture collapsed. In AIM-HIGH, more than 3,400 patients already well treated with statins, niacin prevented no net heart attack or stroke, and the trial was halted early for futility, with a worrying flicker on the side of harm. Then came HPS2 THRIVE, more than 25,000 patients, the largest niacin trial ever conducted, which found no benefit on top of statins and real, measurable harm, more new diabetes, infection, and bleeding. The National Lipid Association advised pulling back from routine use.
The animal biology, in fairness, is genuine, niacin cuts mouse plaque by up to about 78 percent and stabilizes it, but it did not rescue real people layered on modern statins, and the risks arrived from the direction the camera was not facing.
That is the gap between mechanism and outcome, the most expensive gap in medicine. Niacin reverses plaque on a scan and fails people in the trials that count. Do not start it without a physician and a reason. A better picture is not a longer life.
Two Other Fat Soluble Vitamins
“Vitamins are just the alphabet of life.”
Dr. Kevin Ham
You asked me to add vitamin E and vitamin A, and I am glad you did, because together they deliver the cleanest proof of the rule this newsletter keeps circling. Both are antioxidants the artery seems to want, both look magnificent on paper, and both, as isolated high dose supplements, have failed, and in some cases harmed, the very people who hoped for protection. They are not the stars of this story. They are its final and most sobering witnesses.
Vitamin E, the Antioxidant?
“So much promise, yet does not deliver as expected. There must be more to E than meets the I.”
Dr. Kevin Ham
Vitamin E, alpha tocopherol, C29H50O2, is fat soluble and not made by the body. You get it from nuts, seeds, and their oils. On paper it is the antioxidant the artery begs for, dissolving into cell membranes and into the LDL particle to block oxidation. For years it was a great hope. Then the trials arrived and the hope did not survive them. Large studies found no reduction in heart attacks or strokes, a hint of more heart failure, and, pooled together, a small but real rise in death from any cause above the recommended amount, while one antioxidant cocktail even blunted the benefit of a statin and niacin. Genuine deficiency is rare. Bottom line, get it from a handful of nuts and seeds, and leave the capsule on the shelf.
Vitamin A, the Paradox
“Always first but the first becomes the last in serving and greatness.”
Dr. Kevin Ham
Vitamin A is the most paradoxical, because the plant eater does not eat it directly. True vitamin A, retinol, C20H30O, is found preformed only in animal foods. Plants give the raw material, the carotenoids, above all beta carotene, C40H56, which the body converts into retinol as needed, so you make your own from the pigments in bright vegetables, sweet potato, spinach, carrots. Vitamin A's real work is in vision, in the skin and the linings of the body, and in the immune system. Its link to atherosclerosis is thin, and there is no evidence it reverses plaque.
But it carries the most chilling cautionary tale in the field. When researchers gave high dose beta carotene to smokers to prevent lung cancer, in the ATBC and CARET trials, it did the opposite, more lung cancer and more death, and one trial was stopped early. The same beta carotene harmless in a carrot became dangerous as a megadose in a smoker's blood. Preformed vitamin A is the other hazard, toxic to the liver in excess and a known cause of birth defects, which is why pregnant women are warned away from high doses. Bottom line, eat the bright vegetables freely, since beta carotene from food cannot poison you, but never take high dose beta carotene, above all if you smoke, and never megadose preformed vitamin A.
Solo or Team work?
“Life is a silent symphony, invisible to the naked eye but delighting the eye of God.”
Dr. Kevin Ham
Mostly they work independently, so calling them a team oversells it. Vitamin C builds the wall, niacin works on lipids and inflammation, vitamin A keeps to vision. There is even a caution worth knowing. More antioxidants is not more protection, since vitamin C, E, and beta carotene at high doses once blunted the benefit of a statin and niacin. But one true partnership is worth acting on. Vitamin D raises the calcium your body absorbs, and vitamin K2 decides where it settles. Take aggressive vitamin D without enough K2 and you may raise the supply while the traffic controller is off duty, which in animal arteries is when calcification climbs. That pairing is the one real synergy here.
I like the idea of the dose makes the medicine and the poison, focused on the amount and form of the vitamins in an inverted U curve where Goldilocks dose is just right. Too little, no benefit and harm. Too much, toxicity and harm. Needs to be just right, just like all parameters of life from temperature, acidity, movement and light.
Food or Pill?
“Nature provides all we require in sufficient measure but we are blind to its magic.”
Dr. Kevin Ham
Step back and one shape emerges, the same in every vitamin. The vitamin in food beats the same vitamin in a capsule, again and again. Vitamin C from fruit slowed plaque while supplements sped it, K2 shows its signal in natto eaters and not in pills, beta carotene protects in a carrot and killed in a capsule, vitamin D works at modest levels and harms at towering ones. The reason is not mysticism, it is pharmacology. Food delivers a nutrient slowly, with everything it naturally comes packaged with, at a dose your body has spent millions of years learning to expect. A high dose pill delivers a single molecule in a sudden flood the body reads as a signal it was never built to interpret, and sometimes answers with harm. Dose, context, and rate are not footnotes to a nutrient. They are the nutrient, and the plate gets all three right in a way the bottle almost never does.
How Many of Us are Actually Deficient?
“A little hole still leaks over a long time to empty life away.”
Dr. Kevin Ham
You asked how many of us are actually deficient. First, one distinction the headlines blur. There is a difference between not eating enough of a vitamin and being measurably low on a blood test. Intake inadequacy is everywhere. True deficiency is rarer, because the body buffers, stores, and for vitamin D, manufactures. The scariest statistics you read are usually intake numbers dressed up as deficiency.
Take vitamin D. By food intake alone more than 9 in 10 Americans fall short, until you remember the skin makes most of it from sunlight. Measured in blood, about 5 percent of Americans are frankly deficient and 18 percent more inadequate, so roughly 1 in 4 are low. Canada is similar, 8 to 10 percent deficient and a third below the bone health cutoff, far worse in winter. This is the one worth a blood test. Vitamin C is second, about 6 to 7 percent of Americans frankly deficient and double that in smokers and the poor, under 3 percent in Canada, with roughly a third more in the suboptimal range.
The rest split in a revealing way. Vitamin E is the paradox, almost nobody is measurably deficient, yet 85 to 90 percent fall below the intake target, a gap that means little for plaque. Vitamin A deficiency is rare here, though 4 in 10 miss the intake target. Vitamin K has no blood standard, only a target most of us miss, with more than half of older adults below it. And niacin is the odd one out, almost nobody is short of it, because we have fortified flour with it for a century, the same reason pellagra vanished.
Now the wider picture, because these vitamins are not where most of us fall down. The nutrients most often flagged as public health concerns include vitamin D, potassium, and fibre, plus iron for young children and menstruating or pregnant women. Almost no one meets the potassium target. More than 9 in 10 miss fibre. About half fall short on magnesium, the mineral your heart's electrical system runs on. B12 deficiency or borderline status runs about 6 percent under 60 and up to 20 percent over 60, a real risk if you are vegan, older, or on metformin or an acid blocker. Iron is a measured deficiency in about 1 in 10 menstruating women, and omega 3 intake is low in most of us.
Put it together and one analysis found about 31 percent of Americans were at risk of at least one true vitamin deficiency or anemia, rising to 40 percent in those taking no supplement, while good eaters sat far lower. So the honest answer is layered. Frank deficiency in the plaque vitamins is mostly vitamin D and vitamin C, and mostly the same people, smokers, the heavy, the poor, the sunless. The widespread shortfalls are elsewhere, in potassium and magnesium and fibre, the very things a whole food plant based plate delivers in abundance. Same lesson, one more time. Fix a true deficiency with a test and a target, and cover the rest with the plate.
How many of us fall short, United States and Canada
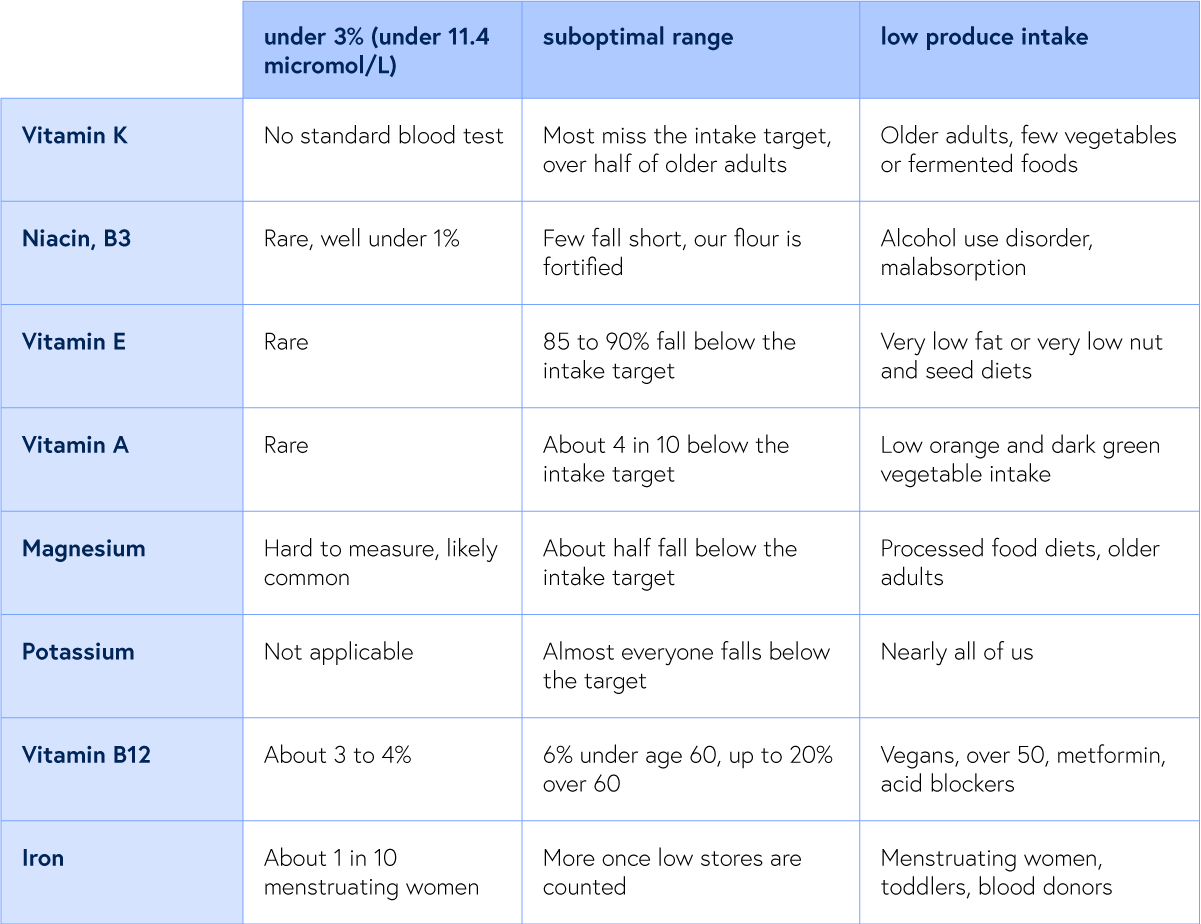
What does a Whole Food Plant-Based Diet Deliver?
“Some of the biggest strongest creatures are herbivores?
Gorillas, elephants, rhinos and hippos. Hmmm.”
Dr. Kevin Ham
Since I eat a low fat whole food plant based diet, and many of you do too, here is what that plate honestly provides. It is generous with most and quietly short on a few. Vitamin C and vitamin A are effortless, several times the target from peppers, citrus, greens, and a single sweet potato. Vitamin K1 overflows from greens, though that is K1, not the K2 your arteries prefer. Niacin is covered by legumes, whole grains, and peanuts. The gaps are predictable. Vitamin D is essentially absent from plants, so it still comes down to sun and a supplement if needed. K2 is scarce without natto or fermented foods, which is why I eat them. And the low fat part matters for vitamin E, because cutting nuts, seeds, and oils cuts the foods that carry it, so a strict plate can land below target, which means little for plaque but is worth knowing. Beyond these, a plant based diet needs vitamin B12 without exception, and benefits from algae omega 3 and iodine. The plate wins easily on potassium, magnesium, and fibre, the shortfalls that trip up everyone else.
What Actually Reversed my Carotid Plaque?
“Intuition, science, lifestyle changes with faith and love.”
Dr. Kevin Ham
I will close where I began, with my own neck, because the most important sentence here is the one the marketing drowns out. I literally put my neck on the line by not getting a stent, going on statins and a baby aspirin. Yes it had its risks. But the evidence showed me what is possible to reverse plaque and eliminate almost all risk of a heart attack.
None of these vitamins reversed my carotid plaque. The foundation did. A whole food, plant based diet very low in added fat, no smoking, prescriptive HIIT exercise, the relentless lowering of ApoB and LDL, blood pressure and blood sugar controlled, real sleep, and in my case a first principle-based fasting protocol. That’s the Reversal engine. The vitamins are stewards and guardians that help.
So the hierarchy I would stake my arteries on when it comes to Vitamins. Get these from food and sunlight, correct genuine deficiencies, treat high dose pills with suspicion, and never confuse a prettier scan with a longer life. Vitamin C from bright plants. Vitamin D from sun and a sensible supplement if your level is low, paired with K2. K2 from fermented foods. E from a handful of nuts and seeds, never the capsule. A as the carotenes in bright vegetables, never the pill. And niacin only in the hands of a physician with a specific reason to reach for it.
I do supplement Vitamin C for prophylaxis of plaque progression and Vitamin D in the winter and boost MK4 short active Vit K2. But I also take the natural forms in foods. I am considering a couple of almonds and hazelnuts for Vitamin E but let’s see what my scans show in June/July.
I am a physician, but not yours, and this is education, not medical advice. Talk to the doctor who knows your numbers before you start, stop, or stack anything, especially niacin, high dose vitamin D, high dose vitamin E and beta carotene, and vitamin K2 if you take a blood thinner. The arteries are more forgiving than I was ever trained to believe, but they are not careless, and neither should we be. My calcium score was 505, a number I was told would only climb. My plaque moved backward in 3 months. Plaque is not a sentence, it is a conversation, and the loudest voice in it is not waiting in a bottle. It is on your fork, in your shoes, in the quiet hours when you let your body repair itself. The engine is you.
A Field Guide to the Six
You also asked for the numbers, and numbers want a table. Here are the six vitamins three ways, their chemistry and daily needs, the top plant based foods with amounts, and the honest supplement guidance, including the heart doses studied, which are not doses to take casually.
Read the last column of Table 3 as the most important text on the page.
Table 1. Chemistry, solubility, and daily needs
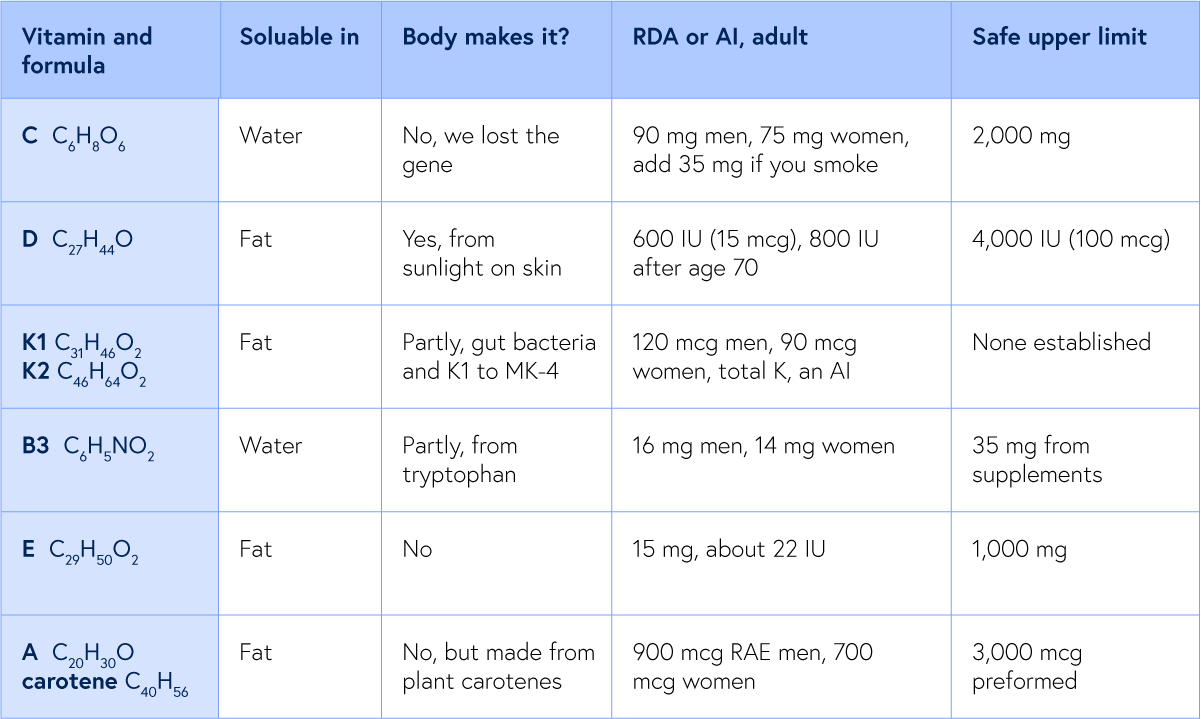
Table 2. Top three plant based food sources, with typical amounts
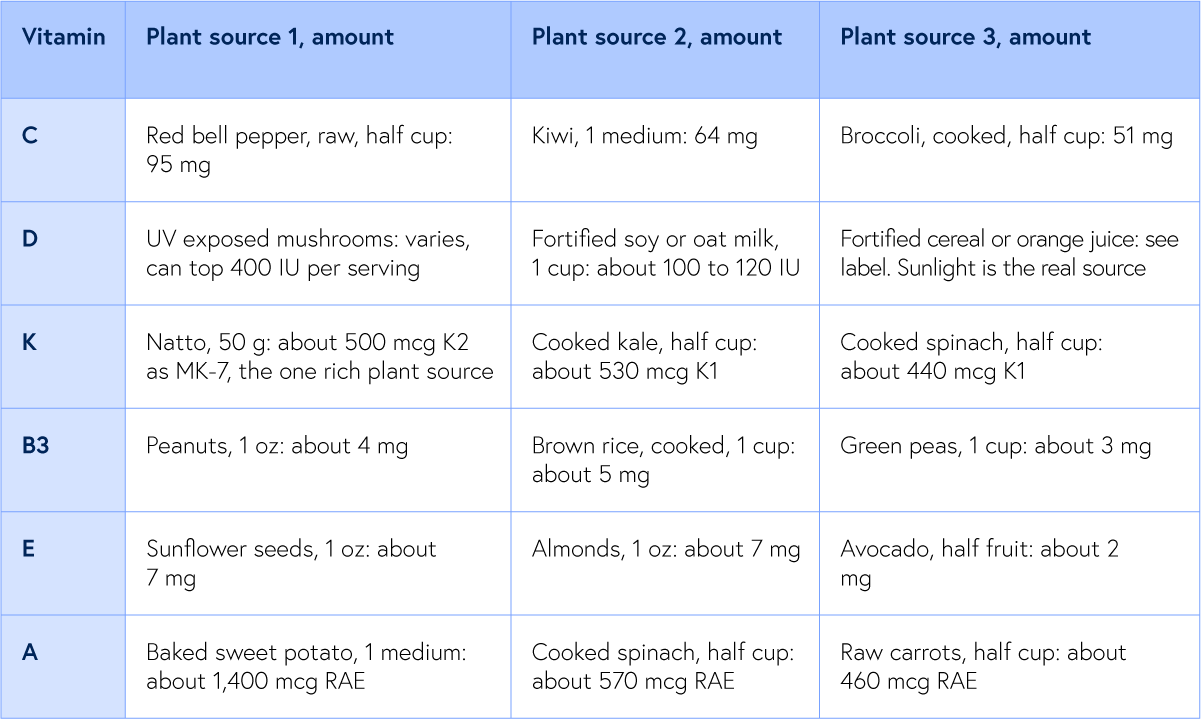
Table 3. Supplements, the heart context, timing, and the cautions that matter most
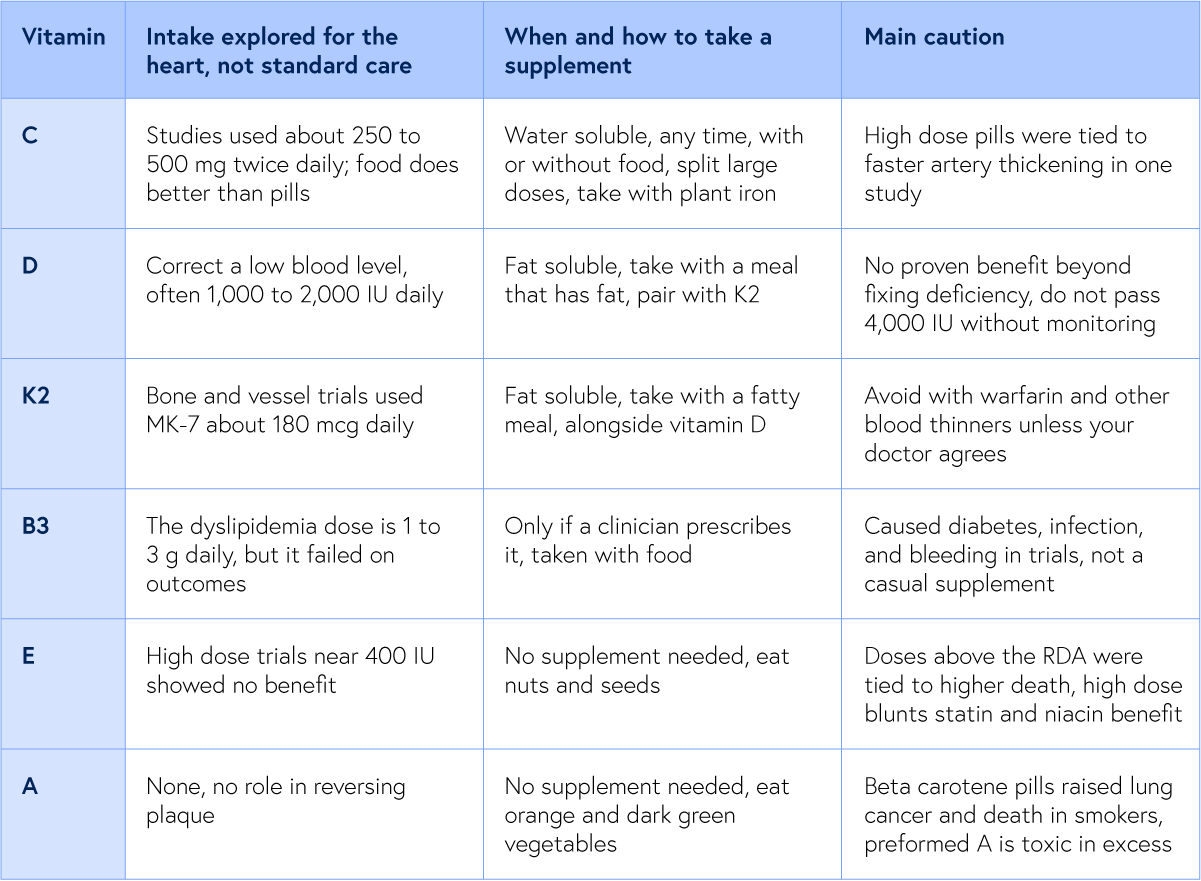
A Question & Action For This Week
Of these vitamins, which one were you taking because you believed it was guarding your heart, and now that you have read this, will you keep taking it?
Reply and tell me. I read every response, and your answers shape what I write next.
And if you do one thing this week, make it one of these three.
Get the one test that matters. Ask your doctor for a vitamin D blood level, and if you smoke or eat little produce, a vitamin C level too. Those are the only two of the six worth measuring.
Feed the gap from your plate. A daily serving of leafy greens for K1, potassium, and magnesium, and a weekly serving of natto or another fermented food for the K2 your arteries actually use.
Audit your supplement shelf tonight. Keep vitamin D paired with K2 only if your level is low, take B12 without fail if you eat plant based, and retire any high dose niacin, vitamin E, or beta carotene unless a doctor puts it there.
A Request
Each Friday, I upload a new YouTube video. Please like, comment and subscribe so I can help many others in your network and beyond. It’s my mission to help people avoid the same fate as Rob, the same fate as I could have had. Heart attack, stroke or sudden death.
https://www.youtube.com/@DrKevinHam
My latest video is going viral :) My #1 meal to unclog arterial plaque. Thank you.
For Someone You Love
There is someone in your life running and falling. You thought of them. Send this to them. Your loved ones just need the information to act and a guide to help them.
Keep going. The race is long, the road is beautiful, and the body was built to heal.
Grace, strength and love to you.
MORE READINGS YOU’LL ENJOY
Health
Reversing My 77% Heart Plaques
Stats Say You Likely Have Heart Plaque
The Healing Power of Food: Nitric Oxide
Meaning
I pray you unlock your heart to reach the height of your full potential by discovering your calling.
Kevin Ham, MD
Appendix
The summary of the referred studies:
Vitamin C from supplements and carotid thickening, Los Angeles Atherosclerosis Study (Agarwal et al., 2012)
Over 3 years, vitamin C from supplements was associated with faster carotid thickening in a dose dependent way, while vitamin C from food was not.
Link: https://pubmed.ncbi.nlm.nih.gov/23002405/
ASAP trial, 6 year follow up (Salonen et al., Circulation 2003)
Slow release vitamin C with vitamin E slowed carotid thickening by about a third in men. Slowed progression, not reversal.
Link: https://www.ahajournals.org/doi/10.1161/01.cir.0000050626.25057.51
Vitamin D and cardiovascular events, large meta analysis (2024), covering VITAL and ViDA
Across more than 134,000 people in 29 trials, vitamin D supplements did not reduce cardiovascular events.
Link: https://pmc.ncbi.nlm.nih.gov/articles/PMC10843321/
Vitamin D deficiency and excess both increase calcification in mice (PLoS One 2014)
Too little and too much vitamin D each raised arterial calcification, the U shaped curve behind the warning against megadosing.
Link: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0088767
Regression of arterial calcification by high vitamin K in rats (Schurgers et al., Blood 2007)
A high vitamin K diet regressed established arterial calcification and restored vessel elasticity, the strongest reversal signal here.
Link:https://pubmed.ncbi.nlm.nih.gov/17138823/
AVADEC randomized trial of MK-7 plus vitamin D (Circulation 2022)
Two years of MK-7 plus vitamin D did not slow valve or coronary calcification despite improving the K dependent biomarker.
Link: https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.121.057008
ARBITER 6 HALTS, niacin and carotid thickness (Taylor et al., NEJM 2009)
Niacin added to a statin regressed carotid thickening, the imaging success at the root of niacin's reputation.
Link: https://pubmed.ncbi.nlm.nih.gov/19915217/
HPS2 THRIVE, niacin outcomes (NEJM 2014), more than 25,000 patients
No cardiovascular benefit on top of statins, plus serious harm: new diabetes, infection, and bleeding.
Link:https://pubmed.ncbi.nlm.nih.gov/31447131/
Vitamin C, NIH Office of Dietary Supplements fact sheet
Authoritative source for the RDA, the food amounts, and the upper limit cited in the field guide.
Link: https://ods.od.nih.gov/factsheets/VitaminC-HealthProfessional/
Vitamin A and carotenoids, NIH Office of Dietary Supplements fact sheet
Documents the ATBC and CARET trials, in which high dose beta carotene increased lung cancer and death in smokers.
Link: https://ods.od.nih.gov/factsheets/VitaminA-HealthProfessional/
Beta carotene, vitamin A, and vitamin E and all cause mortality, meta regression (2013)
Beta carotene above 9.6 mg and vitamin E above the RDA were each tied to a small but significant increase in death.
Link: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3765487/
Vitamin D status in the United States, 2011 to 2014 (NHANES, J Nutr 2019)
By the conservative US thresholds, about 5 percent of Americans were at risk of vitamin D deficiency and 18 percent at risk of inadequacy.
Link: https://pubmed.ncbi.nlm.nih.gov/31076739/
Vitamin D status of Canadians, Canadian Health Measures Survey
About 8 to 10 percent of Canadians fall below 30 nmol per litre, with roughly a third below the 50 nmol bone health cutoff and far more in winter.
Link: https://www150.statcan.gc.ca/n1/daily-quotidien/141216/dq141216d-eng.htm
Serum vitamin C and the prevalence of deficiency in the US (NHANES, AJCN 2009)
About 6 to 7 percent of Americans were frankly vitamin C deficient, with much higher rates in smokers and low income groups.
Link: https://pubmed.ncbi.nlm.nih.gov/19675106/
Vitamin C status of Canadian adults (CHMS 2012 to 2013, CMAJ Open 2016)
Fewer than 3 percent of Canadian adults were vitamin C deficient, with lower levels in smokers and those with obesity.
Link: https://pubmed.ncbi.nlm.nih.gov/27192205/
Micronutrient inadequacies in the US population (Linus Pauling Institute, NHANES)
By intake, roughly 94 percent fall short on vitamin D, 88 percent on vitamin E, 52 percent on magnesium, 43 percent on vitamin A, and 39 percent on vitamin C, with nearly everyone short on potassium.
Link: https://lpi.oregonstate.edu/mic/micronutrient-inadequacies/overview
Risk of multiple concurrent micronutrient deficiencies in the US (Nutrients 2017)
About 31 percent of Americans were at biochemical risk of at least one vitamin deficiency or anemia, rising to 40 percent in those taking no supplement.
Link: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5537775/
Subscribe to my Compounding Wisdom newsletter and start transforming your life. ham.com
Subscribe to my YouTube channel @DrKevinHamfor videos on how I reversed my clogged arteries in 3 months, the top foods that clear your arteries, and the first principles of health that can save your life. Like, share and subscribe — it could save the life of someone you love.
The Diets with No Heart Disease or Cancer
7 Traditional peoples and their diets with no heart disease or cancer
7 Traditional peoples and their diets with no heart disease or cancer, and the cancer record that first set Dr. Esselstyn looking for help for his breast cancer patients and then his most severe cardiac patients.
Dr. Kevin Ham, MD
“Three quarters of the people on this planet had no heart disease. The same peoples carried almost no breast cancer. What were they eating, to the gram, and what does that inform us to eat to be free of our modern day diseases?”
Dr. Kevin Ham
Before Dr. Caldwell Esselstyn became a doctor who prevented and reversed heart disease in the most severe cases at the Cleveland Clinic from 1986 onwards, he was a breast cancer surgeon, and 11 years into that work at the Cleveland Clinic, he grew restless. What unsettled him most was a single fact he could not put down. Roughly three-quarters of the human beings alive had no heart disease at all, and the same people carried strikingly little of the breast cancer he was cutting out of women every week. The common thread was neither a gene nor a drug. It was the food. He himself had a family history of heart attacks, and so he decided to go on this whole plant-based, low-fat diet himself to prevent his own potential demise from a heart attack. His wife went on this diet shortly thereafter when her sister was diagnosed with breast cancer. They are 92 and 90 years old, respectively.
Esselstyn saw that each of these traditional diets had total cholesterol under 150 mg/dL. Below that line, he argued, coronary disease is essentially nonexistent, and he named the people who lived beneath it: central Africa, the highlands of New Guinea, the Tarahumara of northern Mexico, and rural China. Scott Grundy had put the companion figure on the record, that with a blood pressure of 110/70 and a cholesterol under 150, roughly 90% of heart attacks could be avoided. No one has really educated the public well about the plate that would get them there.
I have spent the last year living inside this kind of diet. My own carotid plaque reversed completely in just 3 months on the Esselstyn diet protocol, along with my own first-principles-based layered fasting, and the 5,000 kilometres I ride each year. So this week I went looking for the people Esselstyn pointed at, not for the slogan but for the arithmetic. What did they actually eat, to the gram? Did anyone open their chests and look? And since Esselstyn came to all of this through the breast, what did these same people leave on the cancer record? Seven witnesses answer. Some you will find surprising but definitely informative points of reference to highly consider each time you put something into your mouth.
7 Witnesses For Your Plate
“Eat food. Not too much. Mostly plants.”
Michael Pollan, In Defense of Food
The dietary surveys are old, most of them from the 1950s through the 1990s, the last decades when people still ate the food their grandparents grew before the supermarket reached them. The food we eat today is not the same as what our grandparents grew up with. My father said he ate meat once a year, even though he worked on a farm. Korea went through colonial rule by Japan from 1910 to 1945 and then the Korean War, 1950-1953, where the land and people were ravaged. My father was born in 1936. He is now 90 years old. Now he has a belly with visceral fat due to eating too much and not enough movement, as walking becomes difficult. I have him on two meals a day to reduce his visceral fat; the third meal is really a stored form of high-energy energy in his liver, pancreas, and other organs.
The studies are cross-sectional, and the diagnostic tools were those of their era. No single one of them proves a thing for certain, but it is the convergence, seven peoples on 3 continents arriving at the same place from different foods, that carries the weight.
The First. The Tarahumara of the Sierra Madre.
“The customary diet of the Tarahumaras is hypolipidemic and presumably antiatherogenic.” —William Connor
William Connor and his colleagues spent 4 years in the Sierra Madre measuring a people famous for running footraces over distances that would hospitalize most of us. Their plate was corn, pinto beans, and squash, almost no fat and almost no animal food. Their cholesterol ran far below any line a Western clinic draws, and theirs was among the first human populations in which plasma cholesterol could be shown to rise and fall directly with the food on the plate.
The proof that this was the food and not the bloodline came when the same investigators took 13 Tarahumara and fed them a 4,100 kcal affluent diet, heavy in fat and cholesterol, for 5 weeks. Their lipid levels and body weight increased on schedule. The artery follows the plate, in either direction.
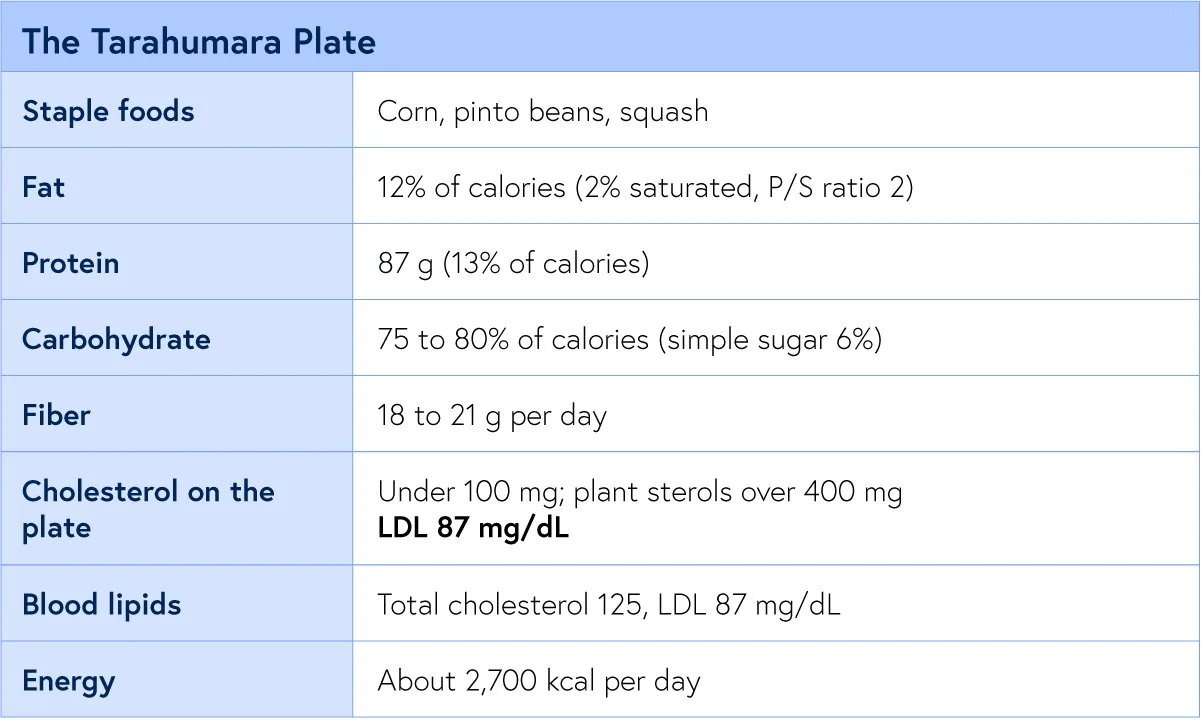
The Second. Rural China.
“A good diet is the most powerful weapon we have against disease and sickness.” —T. Colin Campbell, The China Study
The Cornell-Oxford-China Project remains one of the largest nutritional surveys ever run, collecting blood, food, and mortality data across sixty-five counties. The rural plate carried a fraction of the American fat, several times its fibre, and a tenth of its animal protein. Coronary disease killed American men at many times the rural Chinese rate, and the cholesterol there sat far beneath ours.
This is also the dataset that tied the lipid number to cancer. As cholesterol fell across the counties, so did cancer of the liver, colon, breast, and stomach, and rural breast cancer has climbed since as the villages Westernized. The disease tracks the diet, in real time. The strongest protective signal ran with green vegetables and legumes, the same foods the other six witnesses describe in their own tongues.
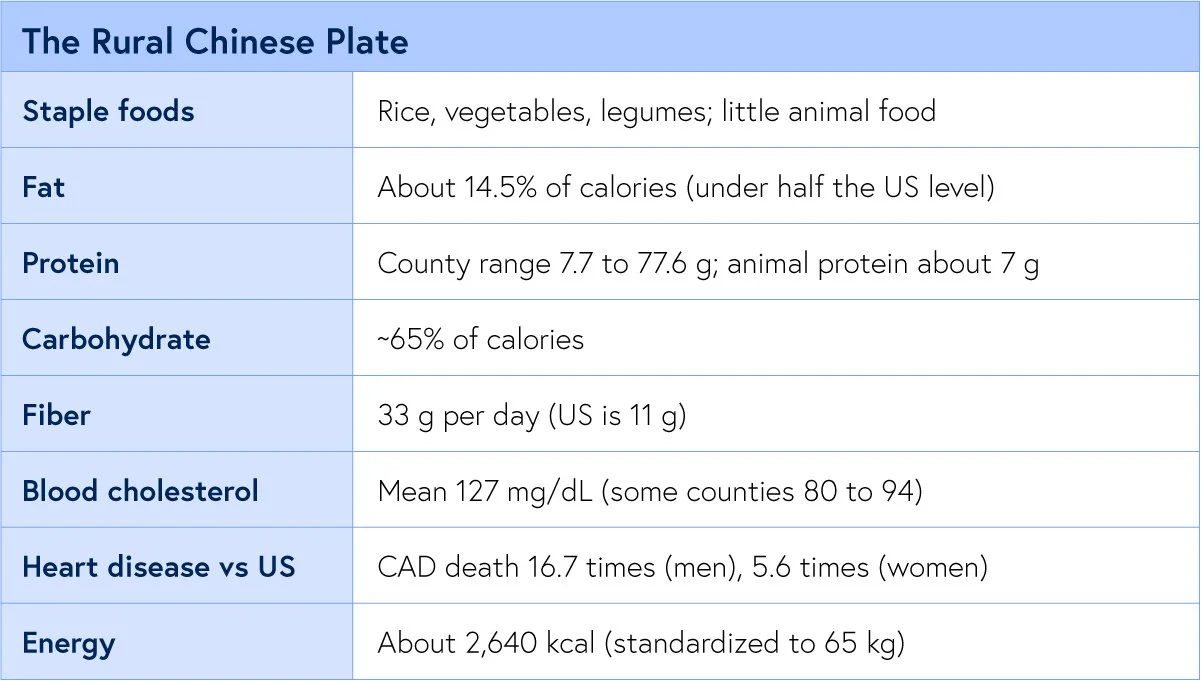
The Third. The New Guinea Highlands.
“Ischemic heart disease was rare if not absent as indicated by resting and post-exercise electrocardiograms.” —Sinnett
It’s based on ECG, which is not definitive for atherosclerosis as we now know it, but back then that was what they mistakenly thought was a clean bill of heart health. Even today, it is the exercise stress test and ECG changes that indicate ischemia, but you could have 80-90% blockages and have no positive ECG changes, like my friend Rob who died suddenly of a heart attack. Even I, with 77%, 51%, etc., blockages, had a normal exercise stress test.
In 1973, Sinnett and Whyte surveyed an entire highland population at Tukisenta and recorded the most extreme diet in the literature, with almost all (90%) of it sweet potato, with fat nearly absent. By every modern reflex it should have wrecked them. Instead, there was no rise with age in blood pressure, cholesterol, blood sugar, or body fat; no diabetes, no gout; and ischemic heart disease was essentially absent. Their glucose tolerance, by the same test used on Americans, was better than ours.
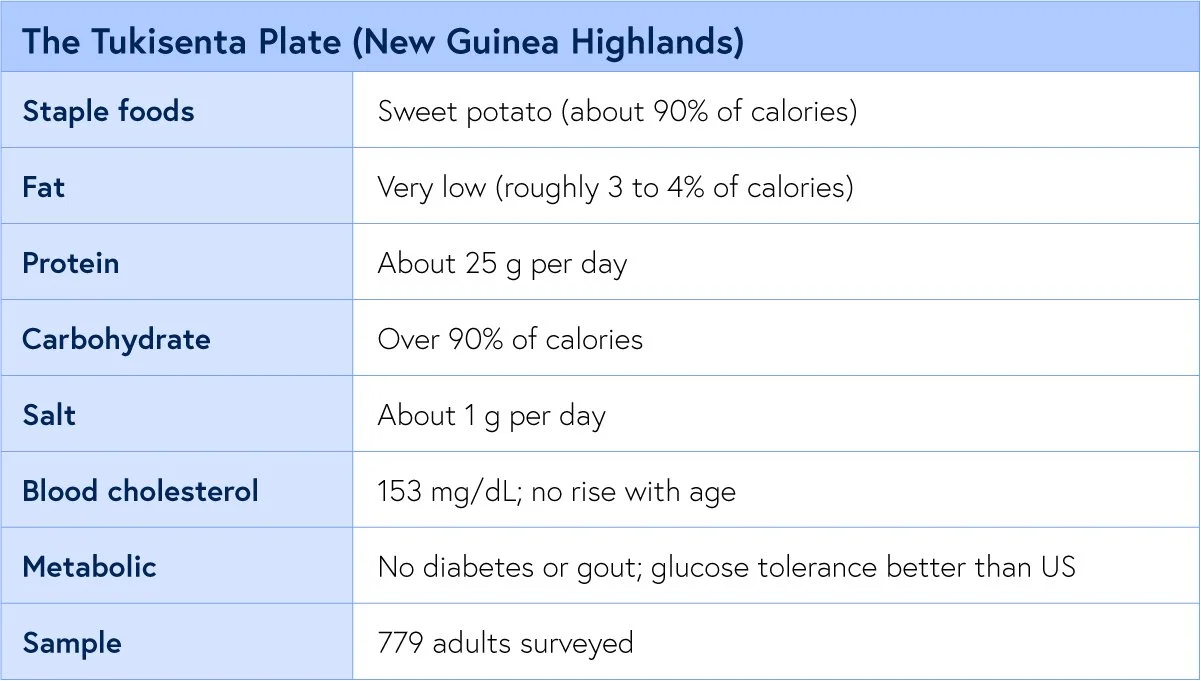
The Fourth. Central Africa.
“In the African population of Uganda coronary heart disease is almost non-existent. This statement is confirmed by adequate necropsy evidence.” —Shaper
Here the evidence is not a questionnaire. It is the autopsy table, which is why this witness matters most. When pathologists in Uganda opened 182 consecutive bodies, they found not one heart attack. The plate was low in fat, unrefined starch and fibre, plantains, sweet potatoes, millet, vegetables, and almost entirely plant protein.
In the South African Bantu, atherosclerosis in the aorta and fatty streaks in the coronary arteries did occur, sometimes severely in the aorta, yet the fatal infarct stayed rare.
Heart disease appeared on cue wherever Africa urbanized to the Western diet.
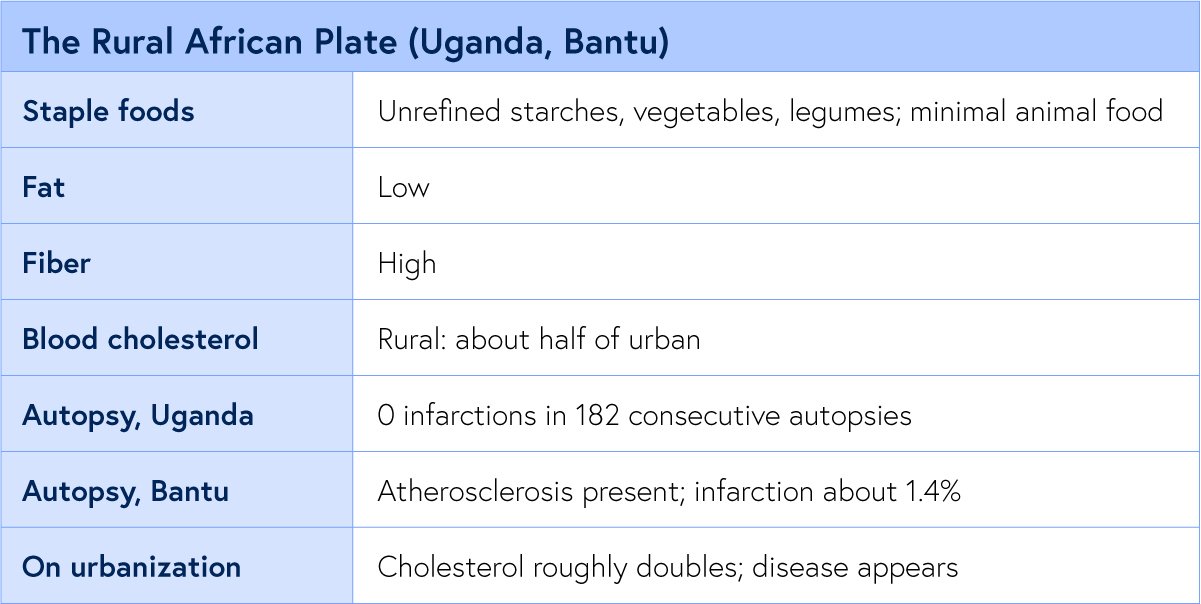
The Fifth. Okinawa, 1949.
“Hara hachi bu: eat until you are 80 percent full.” —Okinawan proverb
The Okinawan record is the best-reconstructed of all because Japan surveyed the islands just after the war. The purple sweet potato supplied most of the plate, soy most of the protein, and fat almost nothing.
And the Okinawans did something none of the other six did on purpose. They ate to about 80 percent fullness and lived in a mild caloric deficit. The result was the highest concentration of centenarians in the world, with heart disease and the hormonal cancers near a fifth of the Western rate.
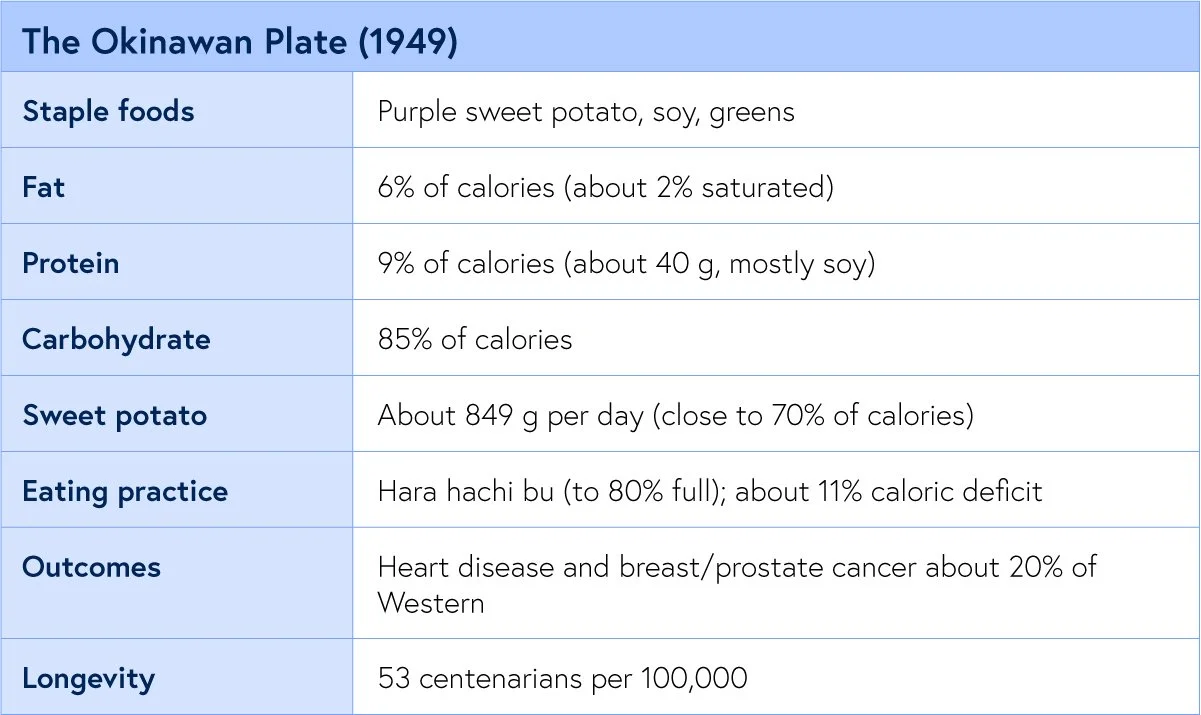
The Sixth. Kitava.
“Apparently free from stroke and ischaemic heart disease.” —Staffan Lindeberg, the Kitava Study
Staffan Lindeberg, the Kitava Study
Staffan Lindeberg spent years on Kitava measuring a people who still ate yam, sweet potato, taro, fruit, fish, and coconut, with refined food at well under one percent of the diet. Among the adults he followed into their nineties, not one case of stroke, sudden death, or angina was found, and this held even though most Kitavans smoked and the coconut pushed some cholesterol readings high. Lindeberg credited leanness and low blood pressure, not a low lipid number, with the protective work.
I have low blood pressure and am lean (BMI was 22)and had severe clogged arteries with LDL at 168mg/dL. Now LDL is 61, and my carotid plaque reversed fully, and CIMT is normal (from 1.8 mm to 0.83 mm in both carotids)
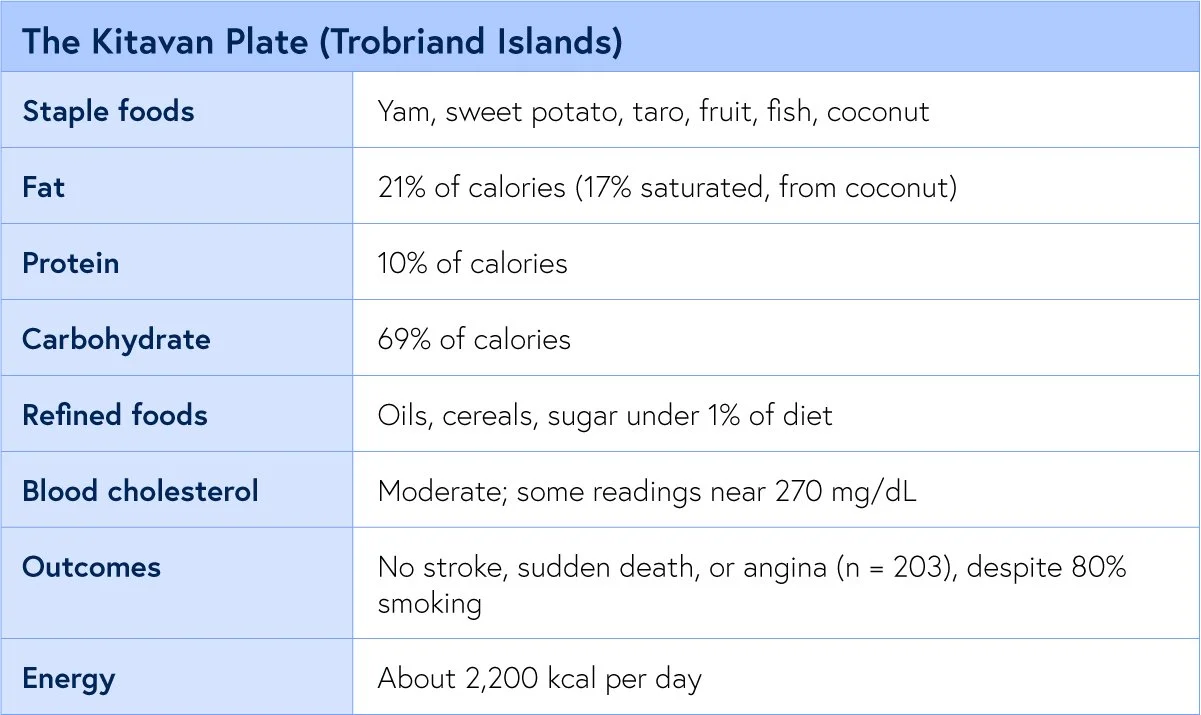
The Seventh. The Polynesian Atolls.
“Vascular disease is uncommon in both populations.” — Ian Prior, 1981
Ian Prior studied two atoll peoples, the Tokelauans and the Pukapukans, in what he called a natural experiment. Coconut supplied most of their energy, so their saturated fat intake was enormous, and their cholesterol sat well above Esselstyn’s line. And yet coronary disease was rare in both. This is the witness that complicates the clean story, and the most instructive of the seven, which is exactly why I keep it in.
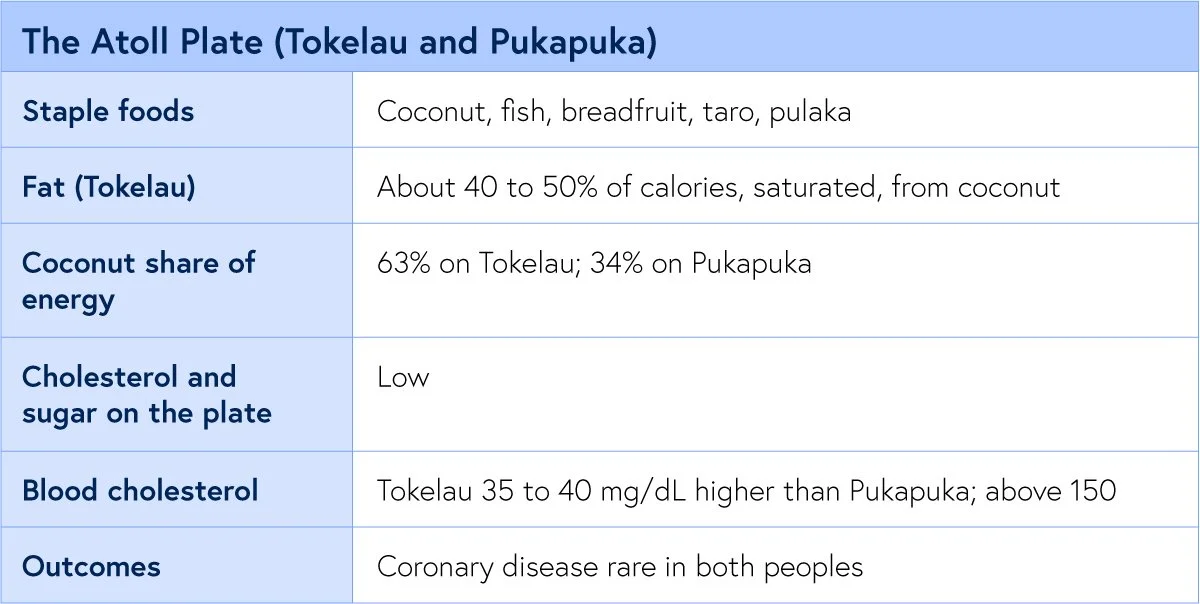
7 Traditional diets that frame the diets that have almost no heart disease or cancers. But what about the autopsy evidence?
What the Autopsies Show
“The easy objection is that these peoples were simply dying before the disease could show. The autopsy table answers it. They opened the chests, and the infarctions were not there.”
Dr. Kevin Ham
Every epidemiologist who has ever reported a healthy population hears the same rebuttal. The disease was there; you just missed it, because the people died young of something else or were never properly examined. It is a fair objection, and the African necropsy literature is the cleanest answer we have to it. You cannot miss a myocardial infarction on a body you have already opened. Among 182 consecutive Ugandan autopsies, there were none.
The Bantu series is even more valuable, because it refuses to flatter the thesis. Atherosclerosis was present in those hearts, sometimes badly in the aorta, in 1.4%. What was rare was the clinical event, the large infarct that kills. The plaque existed. It did not rupture, nor did it occlude the way it does in the West. That distinction between having atheroma and dying of it is the whole game, and it points beyond cholesterol alone toward what makes a plaque stable: leanness, low blood pressure, and an absence of refined foods that inflame a vessel wall.
The Kitavans, with their coconut-driven cholesterol near 270 and their cigarettes, and the Tokelauans with their 40 percent saturated fat, sit in exactly this territory. High numbers, quiet plaques, no events.
The age-of-onset data sharpen it. What the necropsy literature describes is not immunity to atheroma but a vessel wall under so little provocation that the lesion never matures into the thing that kills. Remove the provocation, and even an artery that carries plaque can hold it quiet for a lifetime.
Cancer Dietary Evidence
“Coronary disease is essentially non-existent while hypertension, Western malignancies ... are rarely encountered.”
Dr. Caldwell Esselstyn, MD, Preventive Cardiology, 2001
Because Esselstyn began as a breast surgeon, he never read these populations as a heart story alone. His own argument, laid out in his presidential address to the endocrine surgeons, was blunt. Nations that eat more fat per person carry the highest breast cancer mortality. When people migrate from a low-incidence country to a high one, their breast cancer rate climbs to meet the host country within 2 or 3 generations, which is the single cleanest proof that the cause is the food on the table and not the bloodline. And within one country the gradient holds: rural Japanese women on a low-fat plate had less breast cancer than urban Japanese women on more. The American figure he watched move in his own career, from one woman in 19.1 in 1961 to one in 9 by 1991.
His single most arresting figure is the prostate. In all of Japan in 1958, autopsies recorded just 18 prostate cancer deaths, a rate near 2 per 100,000 men, while American men were dying of it in the thousands. And Japanese men who settled in Hawaii developed far more prostate cancer than those who stayed home. The tumour was not in their genes. It was waiting on a Western plate.
The numbers across the seven hold the same shape. Breast cancer varies more than fivefold between nations and tracks per capita dietary fat closely, running about 7 times higher in the West than in Asia. Sub-Saharan Africa recorded a fraction of the North American breast and colon cancer; Okinawa’s sat near a fifth, and rural China’s fell as its cholesterol fell.
The mechanism that best fits the Asian data is not fat alone but what replaces it. Rural Japanese and Okinawan plates are dense in soy, and the isoflavones in soy, converted by gut bacteria into hormone-like molecules, appear to blunt the estrogen signalling that drives most breast tumours. Women in these populations excrete those compounds at many times the levels observed in Western populations. So the protective plate is doing two things at once: withholding the fat and animal protein that raise circulating hormones, and supplying the plant compounds that quiet them. Subtract the soy and the fibre, add the fat, and the hormonal environment of the Western breast is what remains.
I owe you the honest counterweight, the same one I owe myself on the exercise data. The large Western prospective cohorts, the ones that follow nurses and physicians for a decade, have mostly failed to find a strong link between dietary fat and breast cancer. But read the fine print. Those cohorts sample fat between fifteen and 45 percent of calories. Every protective person in this newsletter lived below 15 percent, with 2 to 3 times the fibre and almost no refined food. The cohorts never measured the place these people lived. You cannot find an effect in a range you never sampled.
Is it the Fat or the Protein?
“If the danger were only fat, the coconut eaters would be dead. The thread through all seven is not low fat alone. It is little animal protein.”
Dr. Kevin Ham
You will hear it argued that I have the wrong villain, that the driver is not fat but protein, and specifically animal protein. The argument has teeth. In a long series of experiments at Cornell, T. Colin Campbell dosed rats with a liver carcinogen and then fed them protein. On 20 percent casein, the protein of milk, the rats grew cancer; on 5 percent, almost none, and he could switch the tumours on and off by raising and lowering that animal protein. Plant proteins, soy and wheat, did not promote the tumours even at 20 percent.
The heart has its own version. When Stanley Hazen and his group at the Cleveland Clinic fed people meat, their gut bacteria turned its carnitine into a compound called TMAO that accelerates atherosclerosis in animals and predicts heart attack and stroke in people. Red and white meat raised it, non-meat protein did not, and the level of saturated fat made no difference at all. Vegetarians, lacking the microbes, barely made it.
I read this as neither a refutation of the fat story nor a footnote to it. Look again at the witnesses. Every one of them ate little fat and little animal protein at the same time, so no population on earth cleanly separates the two.
The protein work is also contested: critics note that Campbell’s low-protein rats may have died of the carcinogen before a tumour could form, and that fish raises TMAO yet protects the heart. My own read is plainer. The Western plate loads fat, animal protein, and refined carbohydrates together, and taking all three down at once empties a plaque. The seven witnesses never ran the controlled experiment. They simply lived the answer.
What the 7 Witnesses Say to Us
“There are always exceptions to the rule. It is the corollary to the rule. Humans are exceptional as is nature in harmony.”
Dr. Kevin Ham
Lay the seven side by side and the pattern is almost monotonous. Six of them sit between 6 and 21% of calories from fat, 9 to 13% protein, fibre at 2 to 3 times the Western intake, refined sugar and oil at or near zero, with lean bodies and a full day of physical work. Those six carry near-absent clinical heart disease, confirmed in Africa on the autopsy table, and roughly a fifth to a seventh of the Western rates of breast and the other hormone-driven cancers.
The two that seem to break the rule, Kitava and the atolls, are the ones I find most clarifying. Both ate enough coconut to carry a cholesterol that would alarm any Western clinic, and both stayed free of heart disease. What they kept is everything else: leanness, low blood pressure, no refined carbohydrate, constant movement. So the line Esselstyn drew at 150 is real and powerful, but it is not the only lever. Leanness is a lever. Blood pressure is a lever. The absence of the refined, oil-soaked, sugar-saturated food that defines our own plate is a lever. The plaque answers to all of them.
And there is the one fact that ties all the witnesses together and shifts the argument from correlation to causation. Each of these peoples lost its protection the moment the Western diet arrived. The Tarahumara fed an affluent plate for 5 weeks. The African who moved to the city. The Okinawan whose mortality advantage vanished as the island Westernized. The disease was never in their blood. It was on a plate they had not yet been handed. That is the whole claim, and it is the reason I ride, and fast, and eat the way I do. The witnesses are unanimous.
3 Things the 7 Teach
“There are always exceptions to the rule. It is the corollary to the rule. Humans are exceptional as is nature in harmony.”
Dr. Kevin Ham
The instruction is plain.
Build the day from whole plants, the grains and beans and tubers and greens that carried all seven of these peoples.
Keep fat low and unrefined.
Drive the cholesterol under the 150 floor that Esselstyn drew, and the LDL well below it, because the lower the lipid drive the faster a plaque empties.
Then add the two levers that Kitava and the atolls prove matter as much as the number. Stay lean. Move every day.
The vessel will follow the plate, and it will follow it in 3 months, not 30 years.
That is the claim I am living, one CT angiogram at a time. The seven witnesses arrived there without trying. We have to choose it.
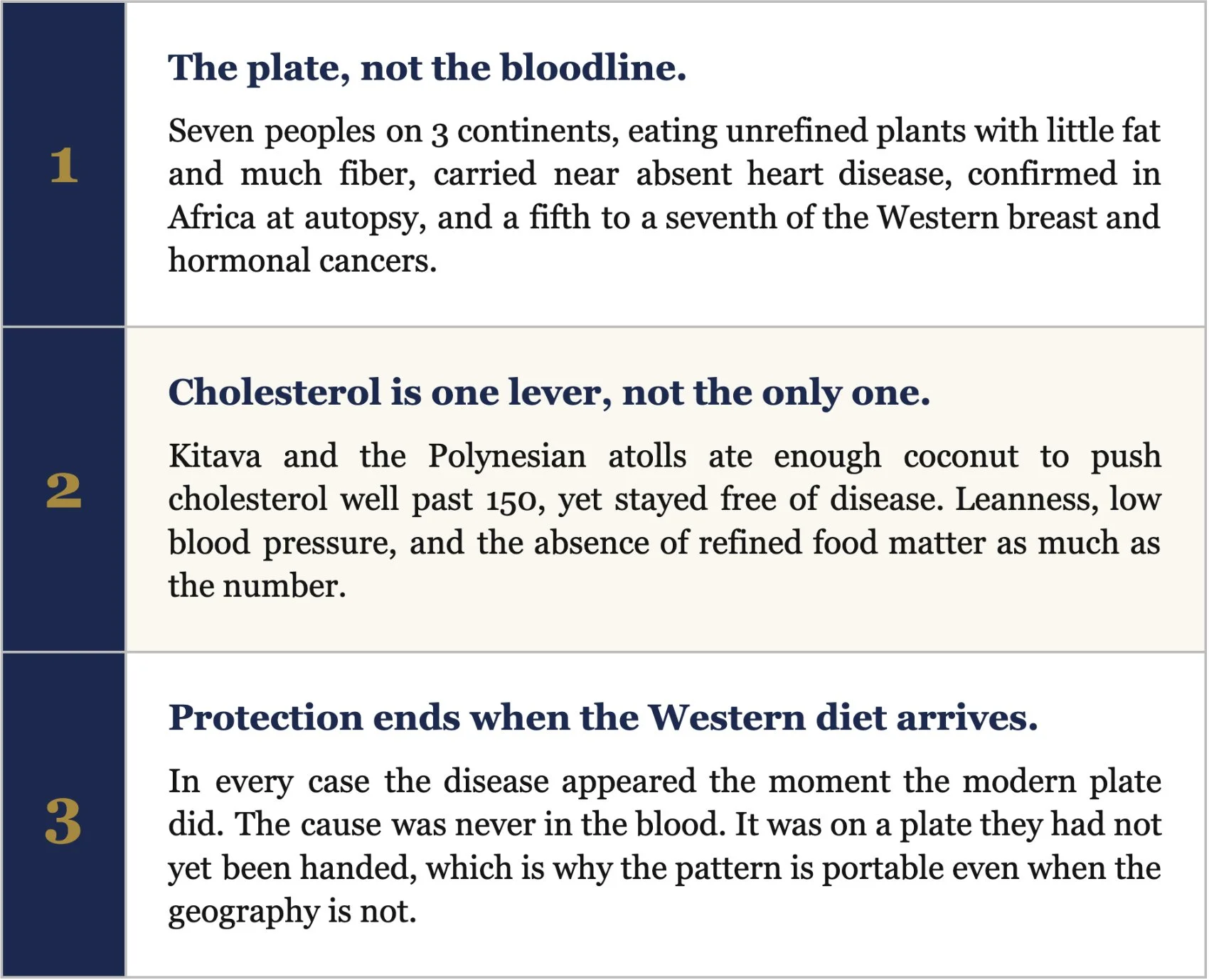
A Question to Meditate On This Week
“If the healthiest hearts that ever lived were built by what people ate on an ordinary day, then what is the one thing on my own plate that these 7 peoples never touched, and what would change in me if I set it down, starting with my very next meal?”
You do not have to move to the Sierra Madre or remake your whole life by Sunday. You only have to choose one plate, and then the next one. So this week, name the single food on your table that belongs to the modern diet and not to the witnesses: the added oil, the refined sugar, the processed meat, and set it down. Then watch how fast your body answers. The artery is listening; it reverses in months and not decades, and it does not care how small that first meal looks. These 7 peoples inherited their pattern without choosing it. You get to choose yours, one plate at a time, beginning with the very next time you sit down to eat. Start there. Start today.
Therefore choose life, that you and your offspring may live.
Deuteronomy 30:19
A Request
Each Friday, I upload a new YouTube video. Please like, comment and subscribe so I can help many others in your network and beyond. It’s my mission to help people avoid the same fate as Rob, the same fate as I could have had. Heart attack, stroke or sudden death.
https://www.youtube.com/@DrKevinHam
My latest video is going viral :) My #1 meal to unclog arterial plaque. Thank you.
For Someone You Love
There is someone in your life running and falling. You thought of them. Send this to them. Your loved ones just need the information to act and a guide to help them.
Keep going. The race is long, the road is beautiful, and the body was built to heal.
Grace, strength and love to you.
MORE READINGS YOU’LL ENJOY
Health
Reversing My 77% Heart Plaques
Stats Say You Likely Have Heart Plaque
The Healing Power of Food: Nitric Oxide
Meaning
I pray you unlock your heart to reach the height of your full potential by discovering your calling.
Kevin Ham, MD
Appendix
The summary of the referred exercise studies:
The dietary surveys, the autopsy series, and the cancer and protein evidence behind this issue, each with a brief synopsis.
1. Connor WE, Cerqueira MT, Connor RW, et al. The plasma lipids, lipoproteins, and diet of the Tarahumara Indians of Mexico. Am J Clin Nutr. 1978;31:1131 to 1142.
Cross sectional survey of 523 Tarahumara aged 5 to 70, sampled across 4 years in the Sierra Madre, with plasma lipids and lipoproteins measured against detailed dietary records. Mean total cholesterol 125 mg/dL, LDL 87, VLDL 21, HDL 25, triglyceride 120; children averaged 116. Total cholesterol tracked directly with the small amount of cholesterol on the plate, among the first such dose response relationships shown in a free living people. Established the corn, bean, and squash diet as hypolipidemic and antiatherogenic, and the Tarahumara as a living low cholesterol reference population.
2. Cerqueira MT, Fry MM, Connor WE. The food and nutrient intakes of the Tarahumara Indians of Mexico. Am J Clin Nutr. 1979;32:905 to 915.
Detailed weighed and recall dietary survey of 372 Tarahumara. To the gram: protein 87 g (13% of energy), fat 12% (saturated 2%, polyunsaturated 5%, P/S ratio 2), carbohydrate 75 to 80% with simple sugar only 6%, crude fiber 18 to 21 g, dietary cholesterol under 100 mg, plant sterols over 400 mg, sodium a moderate 5 to 8 g, on about 2,700 kcal. The most granular macro portrait we have of a traditional very low fat plate, and the companion to the 1978 lipid data.
3. McMurry MP, Cerqueira MT, Connor SL, Connor WE. Changes in lipid and lipoprotein levels and body weight in Tarahumara Indians after consumption of an affluent diet. N Engl J Med. 1991;325:1704 to 1708.
Controlled feeding experiment. Thirteen Tarahumara were moved from their habitual plate of about 2,700 kcal to a calorie dense 4,100 kcal affluent diet rich in saturated fat and cholesterol for 5 weeks. Total cholesterol rose roughly 31% and LDL about 39%, with measurable gains in body weight, triglycerides, and VLDL. The protective profile collapsed in 5 weeks, proving the Tarahumara lipid pattern was diet dependent rather than a fixed genetic trait.
4. Campbell TC, Parpia B, Chen J. Diet, lifestyle, and the etiology of coronary artery disease: the Cornell China Study. Am J Cardiol. 1998;82:18T to 21T.
Ecological study across 65 mostly rural Chinese counties correlating county level diet, blood biomarkers, and cause specific mortality. Mean serum cholesterol 127 mg/dL against 203 in the United States, fat under half the US level, fiber roughly three times higher, animal protein near a tenth; coronary mortality 16.7 times higher in US men and 5.6 times in US women. Cancer mortality at several sites, including breast, fell as county cholesterol declined from about 170 toward 90, with green vegetables and legumes the strongest protective correlates. The largest dataset tying a low cholesterol, plant rich diet to low rates of both heart disease and cancer.
5. Sinnett PF, Whyte HM. Epidemiological studies in a total highland population, Tukisenta, New Guinea. J Chronic Dis. 1973;26:265 to 290.
Total population epidemiologic survey of 779 highlanders over age 15 at Tukisenta, New Guinea. Diet over 90% carbohydrate from sweet potato, protein about 25 g and salt about 1 g daily; no age related rise in blood pressure, serum cholesterol, fasting glucose, or adiposity; no diabetes or gout; glucose tolerance superior to the American Tecumseh cohort tested by the same method. An extreme high carbohydrate, very low fat diet coexisting with metabolic health and essentially absent ischemic heart disease in a lean, active people.
6. Shaper AG, Jones KW. Serum cholesterol, diet, and coronary heart disease in Africans and Asians in Uganda (1959). Reprinted Int J Epidemiol. 2012;41:1221 to 1225.
Clinical and dietary study of African and Asian communities in Uganda, supported by autopsy evidence. Coronary heart disease was almost nonexistent among the rural Africans, contrasted with the rising disease seen in more urban, Westernized groups. A landmark of cardiovascular geography, reprinted in 2012, and one of the four populations Esselstyn names as living below the disease threshold.
7. Higginson J, Pepler WJ. Fat intake, serum cholesterol concentration, and atherosclerosis in the South African Bantu. J Clin Invest. 1954;33:1366 to 1371.
Combined necropsy and biochemical study of the South African Bantu. Coronary atherosclerosis was present and occasionally severe, yet proved myocardial infarction occurred in only about 1.4% of cases, far below contemporaneous European and American figures, with hearts showing small infarcts and patchy fibrosis rather than large transmural infarction; serum cholesterol and fat intake were both low. A cornerstone of the argument that low fat traditional diets blunt the clinical expression of atheroma even when some plaque is present.
8. Florentin RA, Lee KT, Daoud AS, et al. Geographic pathology of atherosclerosis (Uganda autopsy series); with Shaper AG on the Samburu.
Consecutive autopsy series and field cardiology. Among 182 consecutively examined Ugandan autopsies, no myocardial infarctions were found; Shaper separately examined 100 Samburu elders by physical examination and electrocardiography and found no coronary artery disease, despite their pastoralist milk and meat intake. Closes the loophole that the disease was simply undiagnosed, since infarction cannot be missed on an opened heart, and points to leanness and lifelong activity as decisive.
9. Willcox BJ, Willcox DC, Suzuki M. The Okinawa Centenarian Study; with the 1949 Okinawan dietary survey.
The 1949 Okinawan dietary survey paired with the long running Okinawa Centenarian Study. 1949 macros of 85% carbohydrate, 9% protein, and 6% fat, with purple sweet potato near 70% of calories at about 849 g per day and soy the main protein; intake ran about 11% below energy expenditure, reinforced by the practice of hara hachi bu. The cohort later showed about 53 centenarians per 100,000 and heart disease and hormone dependent cancers at roughly a fifth of Western rates. The best documented case of caloric restriction layered on a very low fat plant plate, and of the advantage eroding as the diet Westernized.
10. Lindeberg S, Lundh B. Apparent absence of stroke and ischaemic heart disease in a traditional Melanesian island: Kitava. J Intern Med. 1993;233:269 to 275. With Lindeberg S, et al. Am J Clin Nutr. 1997;66:845 to 852.
Clinical and dietary field study of the Melanesian island of Kitava, largely untouched by Western food. Diet 69% carbohydrate, 21% fat (17% saturated, from coconut), 10% protein, about 2,200 kcal, with oils, cereals, refined fat, sugar, and alcohol together under 1% of energy; among 203 adults aged 20 to 96, interview and examination found no stroke, sudden cardiac death, or exertional angina, despite about 80% being daily smokers, in a strikingly lean population with low diastolic blood pressure. Protection persisting at a coconut driven cholesterol and in the presence of heavy smoking, attributed chiefly to leanness and blood pressure rather than to a low lipid number.
11. Prior IA, Davidson F, Salmond CE, Czochanska Z. Cholesterol, coconuts, and diet on Polynesian atolls: the Pukapuka and Tokelau Island studies. Am J Clin Nutr. 1981;34:1552 to 1561.
Comparative natural experiment between two Polynesian atoll peoples differing in coconut intake. Coconut supplied 63% of energy on Tokelau and 34% on Pukapuka, so saturated fat intake was very high while dietary cholesterol and sucrose stayed low; Tokelauan serum cholesterol ran 35 to 40 mg/dL higher than Pukapukan, attributed to the saturated fat, yet coronary heart disease was uncommon in both. The cleanest demonstration that very high saturated fat from whole coconut did not carry the expected cardiovascular penalty in lean, active peoples free of refined food.
12. Esselstyn CB Jr. American Association of Endocrine Surgeons presidential address: beyond surgery.
A surgeon's synthesis of the international and migration epidemiology of breast cancer, delivered as a presidential address to the American Association of Endocrine Surgeons. Nations with higher per capita fat carry higher breast cancer mortality; migrants from low to high incidence countries reach the host rate within 2 or 3 generations; rural Japanese women on low fat diets have less breast cancer than urban Japanese women; US breast cancer rose from one woman in 19.1 in 1961 to one in 9 by 1991. The origin of Esselstyn's conviction that a 10 to 15% fat plant based diet prevents both the Western cancers and coronary disease.
13. Esselstyn CB Jr. Resolving the coronary artery disease epidemic through plant based nutrition. Prev Cardiol. 2001;4:171 to 177.
Clinical review and argument from Esselstyn's coronary reversal practice. Sets total cholesterol under 150 mg/dL as the level observed in cultures where coronary disease is essentially nonexistent, naming central Africa, the New Guinea Highlands, the Tarahumara, and rural China, and reports halting and reversal of disease in patients held below that line. Frames heart disease and the hormone dependent cancers as twin expressions of the same diet, and supplies the under 150 target this newsletter is built around.
14. International ecological and migration evidence on dietary fat and breast cancer (Carroll; Prentice; Aoki; Boyd).
The body of ecological and migration epidemiology on dietary fat and breast cancer. Incidence varies more than fivefold between nations and correlates with per capita dietary fat at roughly r = 0.8 to 0.9, running about 7 times higher in northern Europe and North America than in much of Asia; Western prospective cohorts sampling fat between 15 and 45% of calories find weaker within population associations. The apparent conflict resolves once you note the protective populations lived below 15% fat, a range the cohorts never sampled.
15. Esselstyn CB Jr (prostate); Annual of Pathological Autopsy Cases in Japan; Akazaki K, Stemmermann GN. Comparative study of latent carcinoma of the prostate among Japanese in Japan and Hawaii.
Esselstyn’s figure traces to Japan’s national pathological autopsy record, which for 1958 logged just 18 autopsy-proven prostate cancer deaths in the entire nation, a rate near 2 per 100,000 men. Akazaki and Stemmermann’s comparative autopsy study found latent prostate carcinoma markedly more common among Japanese men in Hawaii than among those in Japan. Together they argue the prostate tumor is environmental and dietary rather than genetic, since the same gene pool expressed far more disease on a Western plate.
16. Campbell TC and colleagues. Dietary protein level and aflatoxin B1-induced preneoplastic hepatic lesions in the rat. J Nutr. 1987; with Nutrition and Cancer. 1982.
A long series of controlled Cornell experiments in which rats were dosed with the liver carcinogen aflatoxin, then fed differing levels of casein, the protein of milk. Rats on 20 percent casein developed extensive preneoplastic liver lesions while those on 5 percent showed about 75 percent fewer, and tumor promotion could be switched on and off by raising and lowering the animal protein; plant proteins such as soy and wheat did not promote the lesions even at 20 percent. The experimental foundation of the claim that animal protein, not plant protein, drives cancer promotion; the work is contested, since very low protein may let the carcinogen kill cells before tumors can form.
17. Koeth RA, Wang Z, Hazen SL, et al. Intestinal microbiota metabolism of L-carnitine, a nutrient in red meat, promotes atherosclerosis. Nat Med. 2013;19:576 to 585.
Human and mouse study of carnitine, a compound abundant in red meat, and its conversion by gut bacteria into TMAO. Carnitine feeding accelerated atherosclerosis in mice through gut microbes, omnivores produced far more TMAO than vegetarians or vegans, and plasma markers predicted heart attack, stroke, and death across nearly 2,600 patients; later work showed red and white meat raised TMAO while non-meat protein and the level of saturated fat did not. A mechanism by which animal protein, independent of dietary fat, may injure the artery, though the causal weight of TMAO in humans remains debated.
Subscribe to my Compounding Wisdom newsletter and start transforming your life. ham.com
Subscribe to my YouTube channel @DrKevinHamfor videos on how I reversed my clogged arteries in 3 months, the top foods that clear your arteries, and the first principles of health that can save your life. Like, share and subscribe — it could save the life of someone you love.
2x Nobel Prize Winner’s Cure for Heart Disease
Linus Pauling traced the world’s leading killer to a missing vitamin, named the molecule that does the damage, and proposed a cure. Three decades later, cardiology is quietly proving the molecule right.
Linus Pauling traced the world’s leading killer to a missing vitamin, named the molecule that does the damage, and proposed a cure. Three decades later, cardiology is quietly proving the molecule right.
Dr. Kevin Ham, MD
People are asking me “What about Lipoprotein(a)? Have you heard of this? You have a 20% chance for this genetic factor for atherogenic heart disease.
I find this study on Lp(a) very interesting, even though I’ve gotten it tested twice to see if I could move it. I did, somewhat lower, but it was already normal. I thought that I must have a high Lp(a) which factored in my plaque. I went deep on this one and didn’t edit as much or cut it short because I think it’s something to really think about, even if you have normal Lp(a), you will learn a lot.
2x Nobel Prize Winner
“I think we can get almost complete control of cardiovascular disease.”
Dr. Linus Pauling, 1992
Linus Pauling remains the only person ever to win two unshared Nobel Prizes, Chemistry in 1954 and Peace in 1962. He had mapped the chemical bond and read the structure of proteins. So when, late in life, he turned to the disease that kills more human beings than any other, the scientific world had every reason to listen, and almost none of it did.
Heart disease is the number 1 killer on Earth, the leading cause of death for decades. Pauling made a claim so simple it sounded crazy. Coronary disease, he argued, is at its root a chronic, low grade vitamin C deficiency, and it can be prevented and even reversed with three molecules you can buy at any pharmacy for the price of a coffee.
Consider the scale. Elevated Lp(a), the molecule at the center of his theory, is carried by roughly 1 in 5 people on Earth, more than 1.4 billion human beings, the overwhelming majority of whom have never heard of it or been tested for it. It is one of the most common dangerous traits in our species, hiding in plain sight.
To understand why he believed this, and why his colleagues did not, you have to start two decades before Pauling, in a Canadian hospital, with a doctor almost no one remembers.
The Canadian Who Proved Arterial Plaque Reversal
“The Reversibility of Atherosclerosis.”
Dr. G.C. Willis, Canadian Medical Association Journal, 1957
In the early 1950s a Canadian physician named G.C. Willis fixated on a question the cholesterol theory could not answer. If plaque simply precipitated out of the blood, why did it appear in a precise, repeating pattern, always at the bends and forks of arteries where the pulse hammers hardest? To Willis it looked less like a spill than a repair, the body patching where mechanical stress had cracked the lining.
He had a clue. An earlier investigator, Paterson, had found the tissues of heart patients depleted of vitamin C, and it was textbook that vitamin C is required to build collagen, the protein that holds an artery together. Willis chose his animal with care. The guinea pig, like humans and unlike rabbits, rats, or dogs, cannot make its own vitamin C.
The contrast across the animal kingdom was his strongest clue. Almost every other creature makes its own vitamin C in amounts that dwarf what we eat. A 150 pound goat makes around 13 grams a day, and a feedback system can drive that as much as thirteenfold higher under illness, injury, or hard exertion. Those animals, flooded with their own ascorbate, almost never develop the arterial disease that kills humans. To Willis the lesson was plain, that the wall, kept strong by vitamin C, was what mattered, not the cholesterol passing through it. The few species that lost the enzyme, humans, guinea pigs, and a handful of others, are the ones whose walls fail and fill with plaque.
When Willis fed guinea pigs a diet stripped of vitamin C, with no added cholesterol, they grew plaques identical to human atherosclerosis, and when he gave the vitamin back, the lesions cleared. He titled his 1957 report, plainly, The Reversibility of Atherosclerosis. Then he went further. In 1954, photographing the same arteries months apart, he put patients on 500 mg of vitamin C three times a day. Of 6 untreated controls, none improved and 3 worsened. Of 10 treated, 6 had plaques visibly shrink, and in one a leg artery opened enough to raise calculated flow nearly eightfold. Only the young, soft plaques reversed, not the calcified ones. It was, as far as the record shows, the first time anyone had imaged the regression of atherosclerosis in a living person.
Willis also performed autopsies and found human arterial tissue focally depleted of vitamin C exactly at the points of mechanical stress, a local, hidden scurvy in people with no outward sign of disease. You did not need to be a sailor dying of scurvy to be scorbutic where it counted. You only needed to be deficient in the wall of one coronary artery.
His hypothesis tied it together. Where the wall runs short of vitamin C, the ground substance that cements its lining turns leaky, and blood cholesterol drifts in and binds where it never should. In the guinea pigs the deficient diet alone produced the lesions while their blood cholesterol barely moved, and a radiolabeled tracer proved the cholesterol in the plaque came from the bloodstream, not the artery. The plaque was not the artery making fat. It was the blood seeping into a wound vitamin C should have kept closed.
And then medicine moved on. The cholesterol hypothesis was ascendant, the rabbit model was convenient, and Willis and his guinea pigs were filed away and forgotten for a generation.
The Surrogate
“Lipoprotein(a) is a surrogate for ascorbate.”
Rath and Pauling, PNAS, 1990
By the late 1980s two new pieces had appeared. First, arterial disease was understood to begin not as a slow greasing of a clean pipe but as a lesion, a crack in the wall. Second, a sticky, dangerous variant of LDL called lipoprotein(a), written Lp(a), had been characterized, and was found to anchor to tissue through lysine binding sites.
Pauling and Matthias Rath connected the two findings to Willis’s old work, and in 1990 published their hypothesis in the Proceedings of the National Academy of Sciences. Lp(a), they proposed, is a surrogate for ascorbate. The reasoning ran like this. Lp(a) appears in significant amounts almost only in the same short list of species that lost the ability to make their own vitamin C, the primates and the guinea pig. That coincidence, they argued, is not an accident.
When vitamin C is plentiful, the body builds strong collagen, because vitamin C is the cofactor that turns lysine and proline into the hydroxylysine and hydroxyproline that lock collagen fibers together. When it runs short, the wall weakens and the body reaches for an emergency patch. That patch is Lp(a), sticky enough to plaster over a leaking vessel. For an animal facing a brief winter of scarcity, a brilliant stopgap. In a human mildly deficient every day for 50 years, the stopgap never stops. The patch builds on the patch, and that is what we call plaque.
“The body was not failing. It was improvising. Lp(a) was the splint it reached for when the vitamin that builds arteries ran out.”
In a second 1990 PNAS paper, Rath and Pauling supplied the direct evidence. Guinea pigs deprived of vitamin C accumulated Lp(a) inside their arterial lesions, while guinea pigs given an adequate intake of vitamin C developed neither the lesions nor the Lp(a) deposits. The surrogate appeared exactly when the vitamin disappeared, and vanished when the vitamin returned.
The Cure
“Ascorbate prevents the development of atherosclerotic lesions in this animal model.””
Rath and Pauling, hypoascorbemic guinea pig study, 1990
Here is where Pauling, the chemist, made the leap no cardiologist had. If Lp(a) anchors to the wall through lysine binding sites, the move is obvious. Flood the blood with free lysine, and the loose molecules occupy those sites, blocking new Lp(a) and prying loose what has stuck. Rath added proline on the same logic.
So the proposed cure had three parts, each cheap and non toxic. Vitamin C in gram doses to rebuild the collagen so the wall stops needing patches. Lysine, 2 to 6 grams a day, as an Lp(a) binding inhibitor. And proline alongside it. Case reports of angina easing on the combination accumulated from 1991 onward, though they remained anecdotes. Pauling, never modest, believed the regimen could bring cardiovascular disease under nearly complete control.
There was a second half to the theory. Pauling and Rath argued the weakened wall is patched not by Lp(a) alone but by Lp(a) and fibrin together. In their 1991 paper they named the primary lesion the deposition of lipoprotein(a) and fibrinogen in the vascular wall. Lp(a) docks onto that fibrin through the same lysine binding sites, because its apo(a) protein is a near twin of plasminogen, the body’s own clot dissolving enzyme. By occupying plasminogen’s parking spots, Lp(a) keeps the patch from ever being cleared. Clot and cholesterol are stitched together at the lysine site.
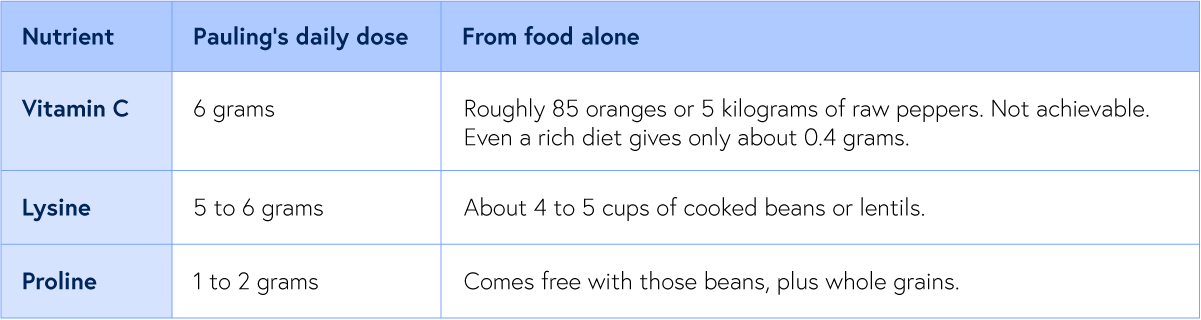
Food versus the bottle: the doses against what a plate can deliver
Pauling therapy doses; food values from USDA and legume data
The table raises an obvious question. Why 6 grams of vitamin C when the blood saturates near 400 mg? Pauling’s answer was that the saturation figure comes from healthy young men, while a stressed, diseased body burns through it far faster, and because the vitamin clears within hours, only repeated grams keep the wall saturated. The honest rebuttal is that the kidney excretes most of an oral megadose, and no trial has shown the high dose beats a modest one for the heart.
This is why lysine is the hinge of the whole cure. Free lysine floods those binding sites, blocks Lp(a) from gluing itself to fibrin and the wall, and can strip loose what has already stuck. Vitamin C does two jobs at once. It rebuilds the collagen so the wall no longer needs a patch, and it converts the lysine residues in the wall into hydroxylysine, lowering their affinity so Lp(a) cannot grip. Lysine and proline release the patch, and vitamin C makes sure the wall stops asking for one. Rath and Pauling were confident enough in the chemistry to patent the approach in the early 1990s.
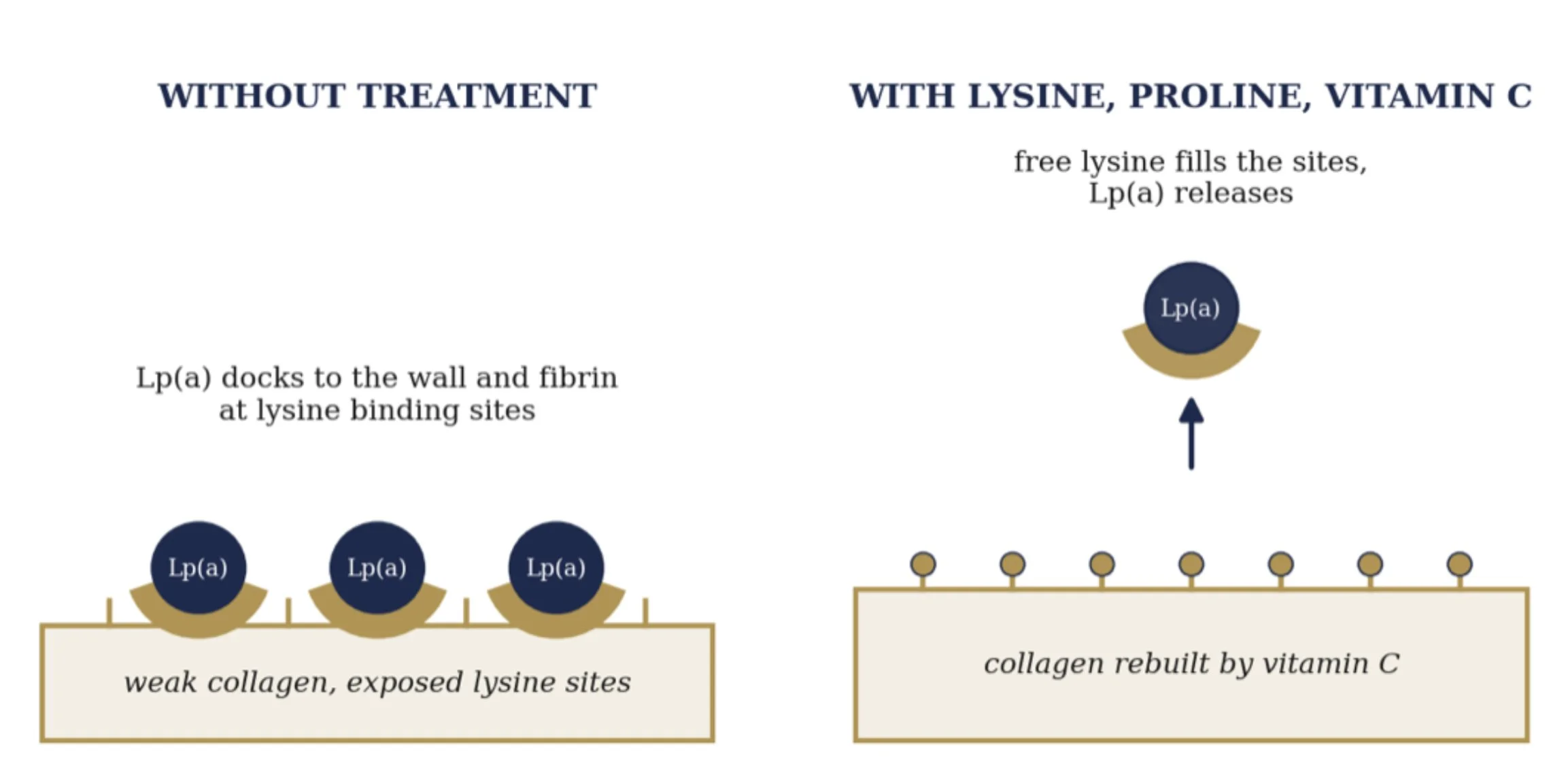
How vitamin C, lysine, and proline release Lp(a) from the wall
Mechanism after Rath and Pauling, 1991 and 1992
It was, on its face, the most consequential medical claim of the century. A two time Nobel laureate had named the killer’s weapon, explained the mechanism, and handed the world a cure made of vitamins and amino acids. And organized medicine declined to pick it up.
How LP(a) Kills
“Lp(a) is about six times more atherogenic than LDL.”
JACC, 2024
To see why this molecule is so lethal, look at how it is built. Lp(a) is an ordinary LDL particle with a second protein, apolipoprotein(a), bolted on. That protein is the whole problem, because it is a near copy of plasminogen, the enzyme the body uses to dissolve clots, sharing as much as 70 percent of its structure. From that one quirk come three ways to cause a heart attack.
The first weapon is plaque. Like LDL, Lp(a) slips into the artery wall and is trapped and oxidized there, only worse. On an equal particle basis it is about six times more atherogenic than ordinary LDL. This is the slow lane, the patient construction of the blockage that Willis and Pauling described.
The second weapon is fire. Lp(a) is the body’s main carrier of oxidized phospholipids, the inflammatory cargo that switches on macrophages and floods the wall with cytokines, leaving a plaque unstable, thin capped, and prone to crack. A particle that merely narrowed arteries would be survivable. One that also inflames them is what makes them rupture.
The third weapon is unique to Lp(a), and it is the one that kills. Because apo(a) impersonates plasminogen, it blocks the conversion of plasminogen to plasmin and raises the body’s clot stabilizing signals. So at the very moment an inflamed plaque cracks, the body cannot dissolve the clot forming over it. The artery seals shut. That sealed artery is the heart attack.
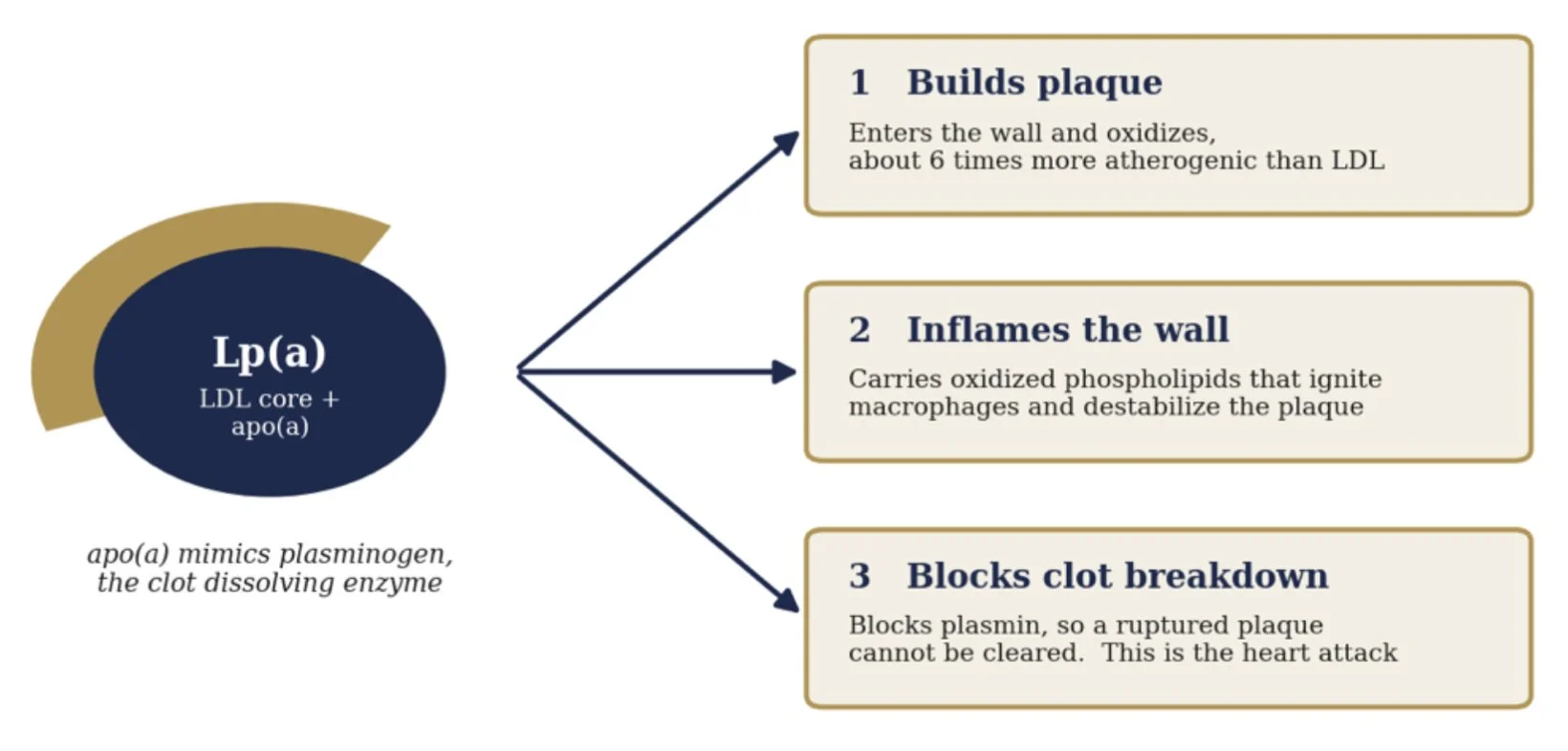
One particle, three ways to cause a heart attack
Mechanism after Boffa and Koschinsky, Nature Reviews Cardiology, 2019
The Genetic Verdict
“A genetically determined, causal, and prevalent risk factor.”
American Heart Association scientific statement, 2022
Here is the fact that turns Lp(a) into a moral one. You do not earn your Lp(a) level through how you live. You inherit it. Between 70 and over 90 percent of a person’s Lp(a) level is fixed by a single gene, the LPA gene, set at conception and holding nearly constant for the rest of life. Diet barely moves it. Exercise barely moves it. Statins do not move it.
That fixity let scientists prove, in a way they almost never can, that Lp(a) does not merely travel with heart disease but causes it, through Mendelian randomization. Because genes are dealt at random at conception and cannot be confounded by how you live, a variant that raises Lp(a) is a lifelong trial run by nature. If those dealt the high Lp(a) genes suffer more heart attacks, the molecule is guilty.
In 2009 the case was closed. The Emerging Risk Factors Collaboration pooled 36 studies and confirmed the association across a smooth gradient. The same year a Copenhagen group showed that genetically elevated Lp(a) raised the risk of myocardial infarction, and a team in the New England Journal found two LPA variants, rs10455872 and rs3798220, that raised coronary risk by roughly 50 to 90 percent per copy. The detail that sealed it: once they adjusted for Lp(a) level, the variants lost all predictive power. The genes act through the molecule and nothing else.
The relationship is a straight dose response. A doubling of Lp(a) raises heart attack risk by roughly 15 percent, and people above 100 mg/dL run more than double the risk of those near zero. The American Heart Association now calls Lp(a) a genetically determined, causal, and prevalent risk factor that stays dangerous even after LDL is driven down. Pauling pointed at this molecule in 1990. The genetics convicted it 20 years later.
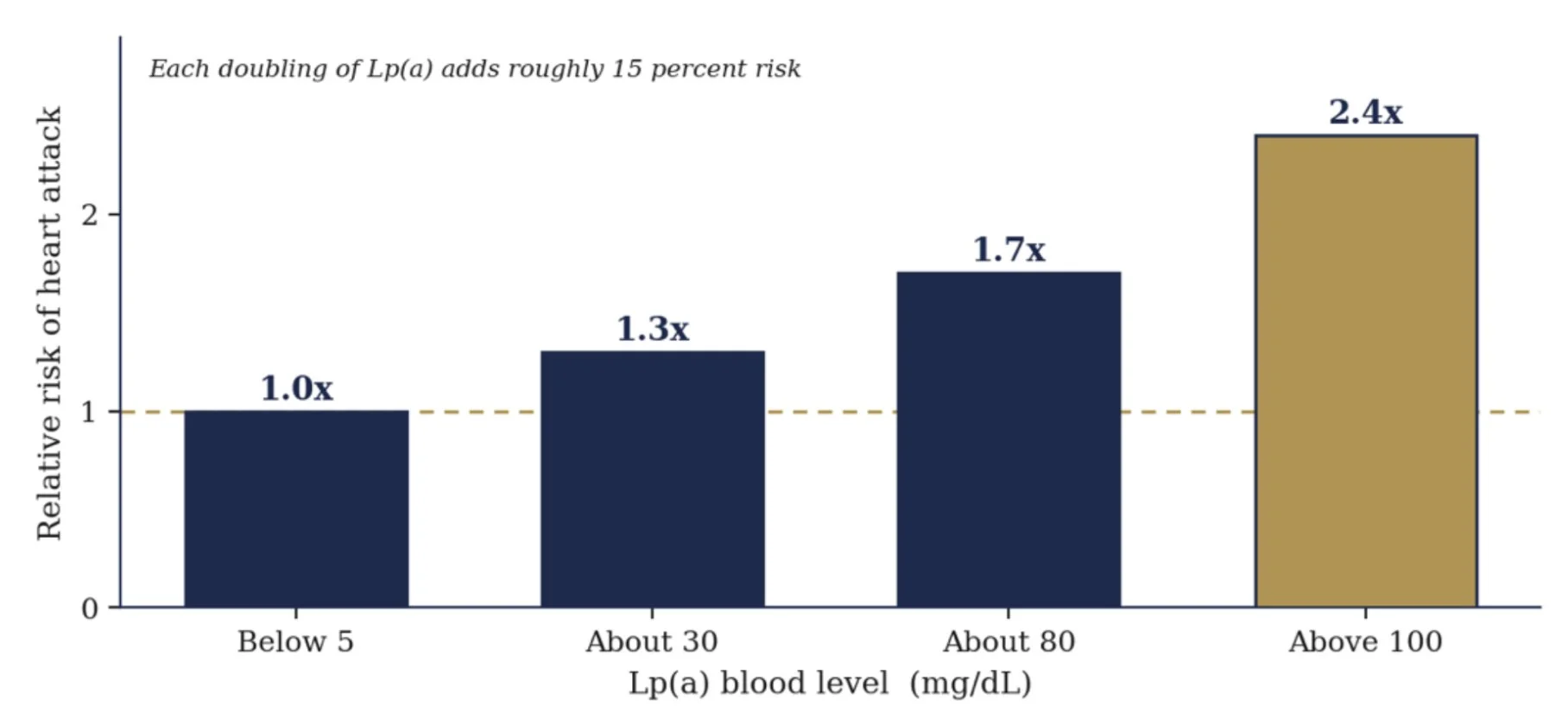
Heart attack risk climbs with Lp(a) level
Approximate, after Copenhagen population studies, Kamstrup 2009
Why Medicine Looked Away
It is worth being honest about why, because the reasons are not all foolish.
First, reputation. Through the 1970s and 1980s Pauling had championed high dose vitamin C for the common cold and then for cancer. Two Mayo Clinic trials, in the New England Journal of Medicine in 1979 and 1985, found it did nothing for advanced cancer. Pauling protested they had used the wrong route, oral instead of iv, but the community had seen enough, and his heart hypothesis inherited the stigma before it was ever tested.
Second, the evidence and the venue. The unified theory papers appeared largely in the Journal of Orthomolecular Medicine, outside mainstream cardiology. The human evidence was pilot data, case reports, and Pauling’s own testimony, never a large randomized trial. By the rules of evidence based medicine, and they are good rules, mechanism plus anecdote is a hypothesis, not a proof.
Third, the reigning paradigm. Medicine had committed its intellect and soon its pharmacy to LDL cholesterol and the statins. A theory insisting that the true driver was a vitamin deficiency and an obscure lipoprotein cut directly against a consensus that would become one of the largest enterprises in the history of medicine.
Fourth, money on the other side too. Rath built a supplement business around the protocol. That commercial entanglement, fair or not, gave academics an easy reason to keep the theory at arm’s length.
Fifth, timing. The tools to measure and to lower Lp(a) at scale, and to run an outcome trial around it, simply did not exist yet. Pauling died in 1994 with the heart hypothesis unproven and very nearly buried.
The Quiet Vindication
“An independent and causal risk factor for cardiovascular disease.”
National Lipid Association, on Lp(a), 2024
Then the molecule Pauling had blamed came back. In the last decade, cardiology has arrived, by its own road and its own data, at three conclusions that Pauling stated first.
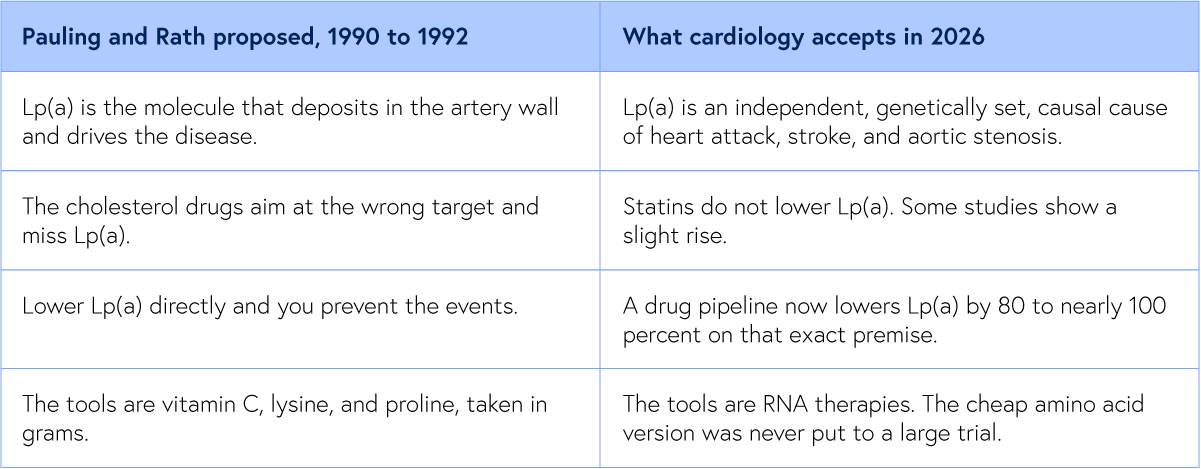
Lp(a) is now recognized as one of the strongest independent, genetically determined, causal risk factors for heart attack, stroke, and aortic valve disease, the culprit Pauling named 30 years before the field agreed. And the statins modern cardiology was built on do not lower it, blind to the very molecule Pauling fingered.
Most striking of all, the entire frontier of cardiovascular drug development is now aimed at doing exactly what Pauling proposed, lowering Lp(a) directly. A wave of new therapies, pelacarsen, olpasiran, lepodisiran, zerlasiran, and the oral muvalaplin, lowers Lp(a) by 80 to nearly 100 percent on precisely Pauling’s premise, that knocking down Lp(a) prevents heart attacks and strokes. The field simply chose engineered RNA over lysine and vitamin C.
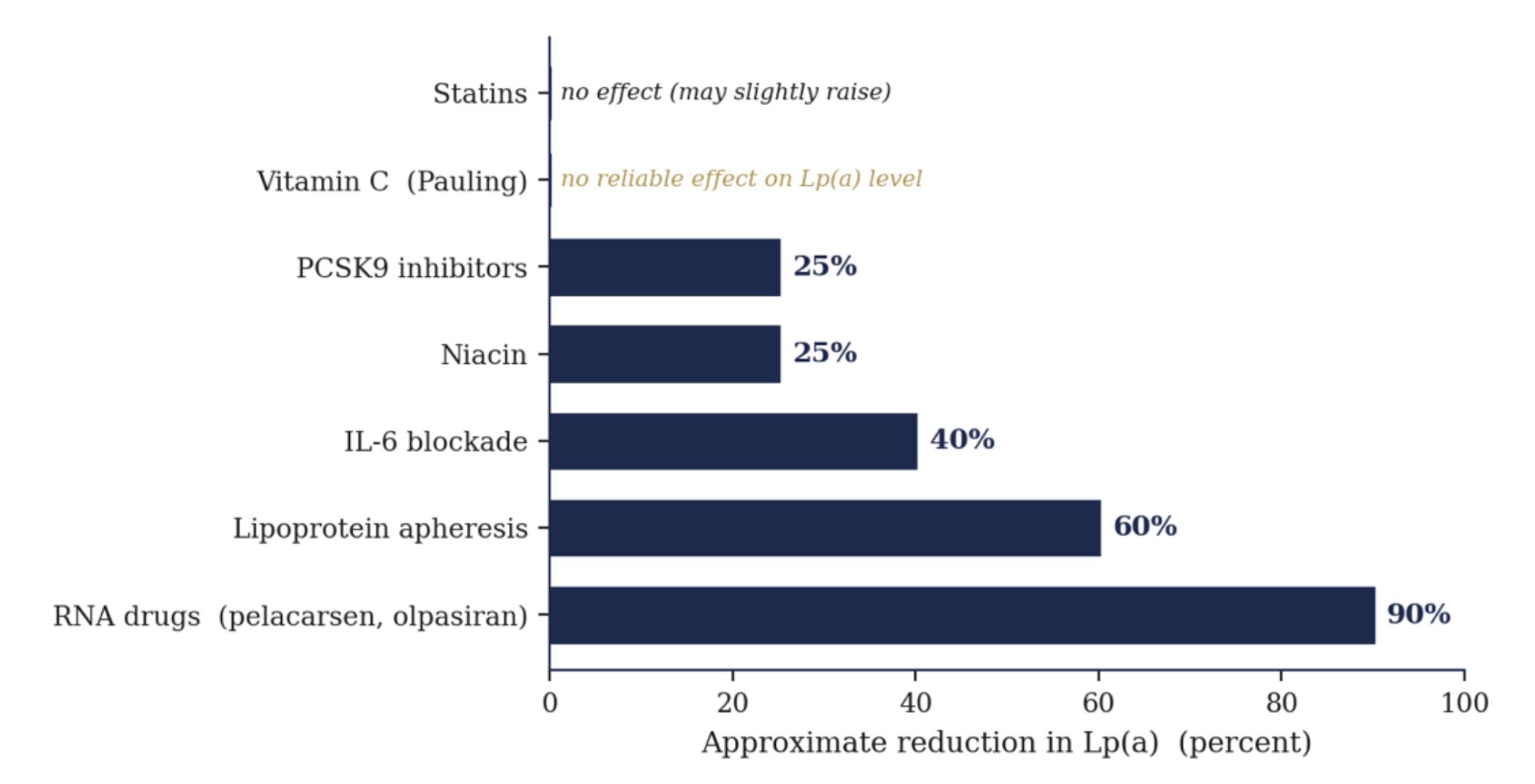
What actually lowers Lp(a), from statins to the new drugs
Approximate reductions. Neither statins nor vitamin C lower the level
Lower the Risk
“Oxidized phospholipids as a unifying theory for lipoprotein(a) and cardiovascular disease.”
Boffa and Koschinsky, Nature Reviews Cardiology, 2019
If the number is written in your genes, is there anything to be done short of the new drugs? Yes, and it comes from separating two things that are easily confused. The level of Lp(a) is mostly fixed. The damage it does is not.
Inflammation is the most actionable lever. The LPA gene is not deaf to the body around it. It carries response elements for interleukin 6, the master inflammatory signal, so chronic inflammation actively drives Lp(a) production. In patients given an interleukin 6 blocking drug, Lp(a) fell by as much as 30 to 50 percent, proof that the level is not wholly beyond reach. And since much of Lp(a)’s harm is delivered through inflammation in the first place, calming the fire blunts both the number and the damage at once.
Oxidation is the next lever, with a caveat. The cargo Lp(a) carries is oxidized phospholipids, so the danger is partly oxidative state, not only quantity. The honest catch is that megadose antioxidant pills have repeatedly failed to lower events in trials, so the credible move is reducing the body’s whole oxidative load through diet and living, not trusting one supplement to neutralize the payload.
Epigenetics is the frontier. The fact that inflammation can switch the LPA gene up and down is proof it is regulated, not frozen. Whether those marks can be deliberately shifted by how we eat and live is still an open question, but it is a real reason the inherited number is not a closed sentence.
This part of the story is mine to act on. I cannot rewrite the LPA gene I was given. Although it’s normal, I can neutralize any of it and possibly even hasten the reversal of the plaque, as it sounds theoretically possible, based on first principle and not much downside from my perspective except focus and time.
I can lower the inflammation that amplifies it, reduce the oxidation that arms it, and clear the fibrin it deposits, with an anti-inflammatory whole food diet, with vitamin C and lysine and proline at the binding sites, and nattokinase at the clot. Cut the cause. Allow the healing. Strengthen the wall. Track the number. The molecule is inherited. The outcome is negotiated.
What It Means
It would be too easy, and untrue, to declare Pauling simply right. The honest verdict is more interesting and more humbling. He was almost certainly right about the target, and he was years ahead of everyone on the mechanism. Lp(a) is real, it is causal, and lowering it is now the great hope of preventive cardiology.
But two questions remain open. The first belongs to all of cardiology. No outcome trial has yet confirmed that lowering Lp(a) reduces events, though the answer is arriving now, with the Lp(a) HORIZON trial of pelacarsen reading out around 2026 and OCEAN(a) by 2027. The second belongs to Pauling alone. No one with the means ever ran a large outcome trial of his cheap amino acid version. Parts of it have not held up in isolation, since vitamin C alone does not appear to lower Lp(a), but the regimen as a whole was never tested. The ingredients are cheap and long off patent, so no sponsor funded the trial.
That gap, between a nearly free intervention and the absence of a trial to confirm or refute it, is the lesson of this story. The artery does not know whether its Lp(a) was lowered by a vitamin or a molecule that took a billion dollars to design. Pauling understood the chemistry. What he could not supply was the will of a system to test a cure no one could sell.
For my own protocol the conclusion is simple. I do not take vitamin C, lysine, and proline as a finished cure. I take them as a wager with good odds and almost no downside, and I give the two time Nobel laureate his due, late, but at last.
A Request
Each Friday, I upload a new Youtube video. Please like, comment and subscribe so I can help many others in your network and beyond, it’s my mission to help people avoid the same fate as Rob, the same fate as I could have had. Heart attack, stroke or sudden death.
https://www.youtube.com/@DrKevinHam
My latest video is going viral :) My #1 meal to unclog arterial plaque. Thank you.
What to Start Now
Get the lipoprotein(a) test. Lp(a). Your doctor likely has not heard of it.
Reduce your risk by lowering your total LDL risk, lowering oxidation, glycation (cut out refined carbs and added sugars) and inflammation (hsCRP<1.0)
Your Question
Question worth exercising with
For yourself. For someone you love. Answer them in the quietness of your day.
When will you get the Lp(a) blood test if you haven’t already?
For Someone You Love
There is someone in your life running and falling. You thought of them. Send this to them. Your loved ones just need the information to act and a guide to help them.
Keep going. The race is long, the road is beautiful, and the body was built to heal.
Grace, strength and love to you.
MORE READINGS YOU’LL ENJOY
Health
Reversing My 77% Heart Plaques
Stats Say You Likely Have Heart Plaque
The Healing Power of Food: Nitric Oxide
Meaning
I pray you unlock your heart to reach the height of your full potential by discovering your calling.
Kevin Ham, MD
Appendix
The summary of the referred exercise studies:
Willis GC. An Experimental Study of the Intimal Ground Substance in Atherosclerosis. Can Med Assoc J. 1953;69:17 to 22.
Willis argued that plaque forms over arterial ground substance weakened by vitamin C depletion and clusters at points of mechanical stress, framing atherosclerosis as a repair response in a locally scorbutic wall rather than a passive spill of fat.
Willis GC, Light AW, Gow WS. Serial Arteriography in Atherosclerosis. Can Med Assoc J. 1954;71:562 to 568.
On vitamin C at 500 mg three times a day, 6 of 10 treated patients showed plaque regression on serial arteriography, while none of the 6 untreated controls improved and 3 worsened. In one case a femoral lumen widened enough to raise calculated flow nearly eightfold. The first serial imaging evidence that human atherosclerosis is reversible.
Willis GC, Fishman S. Ascorbic Acid Content of Human Arterial Tissue. Can Med Assoc J. 1955;72:500 to 503.
Measuring vitamin C in arterial tissue at autopsy, Willis found it locally depleted at the sites of mechanical stress where plaque forms, evidence of a focal scurvy in the artery wall even in people with no systemic signs of scurvy.
Willis GC. The Reversibility of Atherosclerosis. Can Med Assoc J. 1957;77:106 to 108.
In guinea pigs, which like humans cannot make vitamin C, withdrawal produced atherosclerosis and replacement reversed it completely. In 6 of 10 human patients tracked by arteriography, plaques regressed on supplemental vitamin C.
Rath M, Pauling L. Hypothesis: Lipoprotein(a) is a surrogate for ascorbate. Proc Natl Acad Sci USA. 1990;87:6204 to 6207.
Rath and Pauling proposed that Lp(a) acts as a stand in for vitamin C in the species that lost the ability to make ascorbate, depositing on weakened vessel walls as an emergency patch when collagen synthesis falters. Useful in scarcity, it becomes plaque under chronic deficiency.
Rath M, Pauling L. Immunological evidence for the accumulation of lipoprotein(a) in the atherosclerotic lesion of the hypoascorbemic guinea pig. Proc Natl Acad Sci USA. 1990;87:9388 to 9390.
Direct evidence for the hypothesis: vitamin C deprived guinea pigs accumulated Lp(a) inside their arterial lesions, while an adequate intake of vitamin C prevented both the lesions and the Lp(a) deposits. The authors argued for an analogous mechanism in humans.
Rath M, Pauling L. Solution to the Puzzle of Human Cardiovascular Disease: Its Primary Cause Is Ascorbate Deficiency Leading to the Deposition of Lipoprotein(a) and Fibrinogen/Fibrin in the Vascular Wall. J Orthomolecular Med. 1991;6:125 to 134.
The fuller theory, naming fibrinogen and fibrin as the co deposit alongside Lp(a) and proposing that lysine and synthetic lysine analogs, taken with vitamin C, can release Lp(a) from its bonds to the wall. The chemical basis of the lysine binding cure.
Rath M, Pauling L. A Unified Theory of Human Cardiovascular Disease. J Orthomolecular Med. 1992;7:5 to 15.
The capstone synthesis naming chronic ascorbate deficiency as the primary cause of cardiovascular disease, with Lp(a) and fibrin deposition as the downstream damage, and vitamin C, lysine, and proline as the proposed therapeutic counter.
Emerging Risk Factors Collaboration. Lipoprotein(a) concentration and the risk of coronary heart disease, stroke, and nonvascular mortality. JAMA. 2009;302:412 to 423.
A pooled analysis of 36 prospective studies establishing that higher Lp(a) tracks with higher risk of heart attack and coronary death across a continuous gradient. The large scale observational foundation for everything that followed.
Kamstrup PR, Tybjaerg-Hansen A, Steffensen R, Nordestgaard BG. Genetically elevated lipoprotein(a) and increased risk of myocardial infarction. JAMA. 2009;301:2331 to 2339.
A Copenhagen population study showing that LPA gene variants which raise Lp(a) also raise the risk of myocardial infarction. A landmark Mendelian randomization result moving Lp(a) from associated to causal.
Clarke R, et al. (PROCARDIS). Genetic variants associated with Lp(a) lipoprotein level and coronary disease. N Engl J Med. 2009;361:2518 to 2528.
Identified two LPA variants (rs10455872 and rs3798220) that raise Lp(a) and coronary risk, each copy adding roughly 50 to 90 percent. Crucially, the variants lost their association once Lp(a) level was accounted for, proving the molecule itself is the cause.
Burgess S, et al. Association of LPA Variants With Risk of Coronary Disease and the Implications for Lipoprotein(a) Lowering Therapies: A Mendelian Randomization Analysis. JAMA Cardiol. 2018;3:619 to 627.
Used genetics to estimate how much Lp(a) must be lowered to matter clinically, on the order of 100 mg/dL, directly shaping the design and dosing of the new Lp(a) lowering drug trials.
Reyes-Soffer G, et al. Lipoprotein(a): A Genetically Determined, Causal, and Prevalent Risk Factor for Atherosclerotic Cardiovascular Disease. AHA Scientific Statement. Arterioscler Thromb Vasc Biol. 2022;42:e48 to e60.
The American Heart Association consensus statement, declaring Lp(a) genetically determined (70 to over 90 percent), causal, and common, and noting it remains a risk even after LDL is effectively lowered.
Boffa MB, Koschinsky ML. Oxidized phospholipids as a unifying theory for lipoprotein(a) and cardiovascular disease. Nat Rev Cardiol. 2019;16:305 to 318.
Proposes that the oxidized phospholipids carried by Lp(a) tie its three harms together, the atherogenic, inflammatory, and thrombogenic arms, into a single mechanism. The intellectual frame for treating the damage rather than only the level.
Schulte DM, et al. IL-6 blockade by monoclonal antibodies inhibits apolipoprotein(a) expression and lipoprotein(a) synthesis in humans. J Lipid Res. 2015;56:1034 to 1042.
Showed that interleukin 6 drives LPA gene expression and that blocking it lowers Lp(a), while a different anti inflammatory drug did not. Evidence that inflammation actively regulates the Lp(a) level, not only its harm.
Moertel CG, et al. High dose vitamin C versus placebo in the treatment of patients with advanced cancer. N Engl J Med. 1985;312:137 to 141.
A double blind trial that found no benefit of high dose oral vitamin C in advanced cancer. Though about cancer, not the heart, its decisive negative result hardened mainstream skepticism toward Pauling and cast a long shadow over the heart hypothesis that followed.
Nordestgaard BG, Langsted A. Lipoprotein(a) and cardiovascular disease. Lancet. 2024;404:1255 to 1264.
A modern review establishing Lp(a) as an independent, largely genetic, causal risk factor for atherosclerotic disease and aortic stenosis, and noting that conventional lipid lowering drugs, including statins, do not meaningfully lower it.
Lp(a) HORIZON trial of pelacarsen, NCT04023552. OCEAN(a) trial of olpasiran, NCT05581303.
The pivotal phase 3 outcome trials of the new Lp(a) lowering drugs, the first designed to test whether large reductions in Lp(a) actually prevent heart attacks and strokes. Results are expected between 2026 and 2027 and will judge the premise Pauling stated first.
Subscribe to my Compounding Wisdom newsletter and start transforming your life. ham.com
Subscribe to my YouTube channel @DrKevinHamfor videos on how I reversed my clogged arteries in 3 months, the top foods that clear your arteries, and the first principles of health that can save your life. Like, share and subscribe — it could save the life of someone you love.
Which Diet Actually Reverses Plaque?
Mediterranean Diet vs Low-Fat Vegan (Whole Food Plant-based)
Mediterranean Diet vs Low-Fat Vegan (Whole Food Plant-based)
Dr. Kevin Ham, MD
People are asking me “What about olive oil? What about nuts? What about the Mediterranean diet? The portfolio diet? The carnivore, the ketogenic diet? The vegan diet. Can I eat eggs, dairy, fish, meat?
One expert says this, another says that. Sure there are exceptions. But what do the studies show and what do the population studies show?
I used to pour olive oil on everything. I used to eat a lot of nuts. A lot of dairy, meat, seafood.
Now that I have heart disease, I’ve stopped all that. Here’s what I’ve found what each of these diets do and what actually reverses heart disease. Let the evidence speak for themselves.
PREDIMED: The Study that Built the Myth
“The Mediterranean diet is good for everyone. 95% of the population can benefit from it.”
Dr. Ramon Estruch, MD
PREDIMED (Prediction of Diet of Mediterranean) is the most cited diet trial ever run. More than 7,000 people across Spain, all at high cardiovascular risk, were sorted into 3 groups.
One ate a Mediterranean diet enriched with extra virgin olive oil, close to a liter a week.
One ate the same diet enriched instead with a daily handful of nuts.
The third was asked, in the original design, to eat low fat.
The trial ran for years, and the result became scripture. The two Mediterranean groups had about 30 percent fewer heart attacks and strokes than the control. Olive oil, the headlines decided, saves lives. Compared to the control diet.
Read the fine print and a quieter story appears. PREDIMED counted events. Heart attacks, strokes, deaths. It did not, in its main result, measure plaque. And when you lay the actual events side by side, the famous victory is smaller than it sounds.
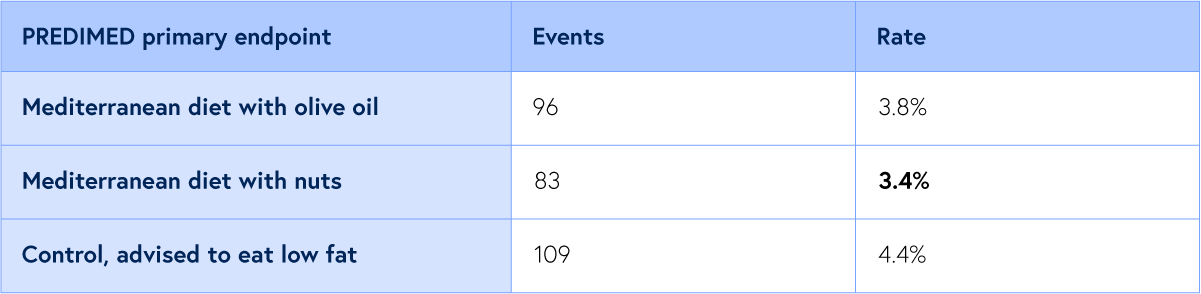
288 primary endpoint events in total. The celebrated result is the gap between 4.4 and 3.4 percent.
This data scares me. This is what people depend on for the proof that the Mediterranean diet prevents death from heart attacks and strokes? Just 1% reduction in severe adverse events?
It means heart disease progressed and is progressing, although at a slower rate than controls. It did not answer the definitive question of whether the Mediterranean diet arrested or reversed heart disease. Just decreased cardiac events and deaths.
That gap, 4.4 percent down to 3.4 percent, is about 1 person in 100 spared an event across roughly 5 years.
It is real, and it is worth having. But it is a difference in events, not in the disease. No one threaded a camera into these arteries or imaged these arteries and watched the plaque retreat. When researchers finally did look, tracking the neck arteries with ultrasound, (not coronary heart arteries) the three diets came apart in a way the event tally had hidden.
In the olive oil group, the artery wall did not shrink. It sat exactly where it had started.
In the nut group, the wall regressed… slightly. The plaque, measurably, grew smaller. Same Mediterranean plate. The only variable was nuts in place of oil, and only the nuts moved the disease slightly backwards.
The Low-Fat Vegan (Whole Food Plant-Based) Diet
“Our bodies often have a remarkable capacity to begin healing.”
Dr. Dean Ornish, MD
To watch an artery heal, you have to leave PREDIMED and return to two stubborn American physicians who used a harder instrument: a camera threaded into the heart itself.
In the 1990s, Dean Ornish took a small group of patients with established coronary disease and put them on a diet most cardiologists called extreme.
About 10 percent of calories from fat.
No added oil at all, not even olive.
Whole food, plant based,
Paired with exercise and
Daily practice of calming the nervous system.
Then he filmed their coronary arteries, and filmed them again 5 years later.
In the treated group the narrowing reversed, the arteries opening by close to 8 percent.
In the control group, following standard heart healthy advice, the narrowing worsened by nearly 28 percent.
The treated patients had less than half the cardiac events.
Caldwell Esselstyn carried the same idea across decades.
In his 2014 series, of 198 patients who held to an oil free, plant based plan,
99.4 percent avoided a major cardiac event over years of follow up.
Not 30 percent fewer events. Almost none at all.
Set the two kinds of study beside each other and the difference in ambition is the whole point.
PREDIMED nudged an event rate by a single percentage point and was crowned.
Esselstyn reversed the plaque on film and almost completely abolished the events.
Same disease. Different finish lines. Different leagues entirely.
The Diet They Actually Ate
“I want patients to eat leafy greens 6 times a day, and no oil.”
Dr. Caldwell Esselstyn, Jr., MD
These three studies get cited in the same breath, as if they tested one idea. They did not. The plates were profoundly different, and so were the lengths of time the patients held to them. Here is exactly what each asked of its people, and for how long.
PREDIMED. Two Mediterranean plates against a low fat control.
PREDIMED ran 3 arms, with no calorie counting and no exercise prescription.
The first group ate a Mediterranean diet built around:
extra virgin olive oil, and was told to use at least 4 tablespoons a day, roughly 50 milliliters. Each household was given 1 liter of free oil a week to make sure they did.
The second group ate the same Mediterranean pattern but traded the oil emphasis for a daily 30 gram packet of mixed nuts,
15 grams of walnuts,
7.5 grams of almonds, and
7.5 grams of hazelnuts, supplied free.
Both Mediterranean groups were coached to
eat vegetables at least twice a day,
fresh fruit 3 or more times a day,
fish or seafood at least 3 times a week,
legumes at least 3 times a week,
white meat in place of red,
a tomato and onion sofrito, and,
for the wine drinkers, a glass with meals.
They were told to steer clear of soda, commercial baked goods, spread fats, and red and processed meat.
The third group, the control, was the quiet flaw in the design. At the start they were simply handed advice to cut all kinds of fat, plus small nonfood gifts, with none of the coaching or free food the other two received. A proper low fat checklist was not even added until about 3 years in. The trial ran for a median of 4.8 years before it was stopped early for benefit.
Ornish. 10% fat, and lifestyle modifications: exercise, stress and support sessions.
The Lifestyle Heart Trial asked far more than a change of groceries. The diet was a
whole food vegetarian plan with about
Fruit, vegetables, whole grains, legumes, and soy filled the plate.
10% of calories from fat,
70 to 75% from complex carbohydrates, and
cholesterol held under 10 milligrams a day.
No added oil.
No meat, poultry, or fish.
The only animal foods allowed were
egg whites and a single cup of nonfat milk or yogurt a day, which is what keeps it from being strictly vegan.
Nuts, seeds, avocados, olives, and caffeine were out, all of them too fatty.
The food was only 1 of 4 pillars. Patients also did about 3 hours of aerobic exercise a week, an hour a day of stress management through yoga, breathing, and meditation, stopped smoking, and met twice a week for 4 hour group support sessions. The program opened with a week long residential retreat. Their coronary arteries were filmed at the start, again at 1 year, and a final time at 5 years.
Esselstyn. No oil, and greens 6 times a day.
Esselstyn was the strictest of the three.
No oil of any kind, not a drop, not even olive.
No meat, fish, poultry, eggs, or dairy, and no refined grains.
He kept nuts, seeds, and avocados off the plate for patients with disease, not because he thinks them unhealthy but because their fat makes a low fat diet hard to hold,
What remained was vegetables, fruit, whole grains, legumes, and leafy greens, which he asked heart patients to eat 6 times a day.
Essential fats instead from a tablespoon or two of ground flaxseed.
Salt, sugar, and caffeine were kept to a minimum.
When diet alone could not pull total cholesterol under 150, he added a cholesterol lowering drug.
His first study, published in 1995, followed 24 severely ill patients, 5 of whom had been told they had less than a year to live. He tracked them past 12 years and reviewed them beyond 20, making it one of the longest studies of its kind.
His 2014 report followed 198 seriously ill patients. Among the 177 who held to the plan, over a mean of 3.7 years, 99.4 percent avoided another major cardiac event, all while staying on their prescribed heart medications.
One contrast is worth marking before the table. The Mediterranean arm that actually shrank plaque leaned on a daily handful of nuts, while both reversal diets, Ornish and Esselstyn, banned nuts outright as too fatty. The same food sits on opposite sides of the line, depending on whether the goal is a lower event rate or the lowest possible fat load. These were never the same experiment wearing 3 hats.
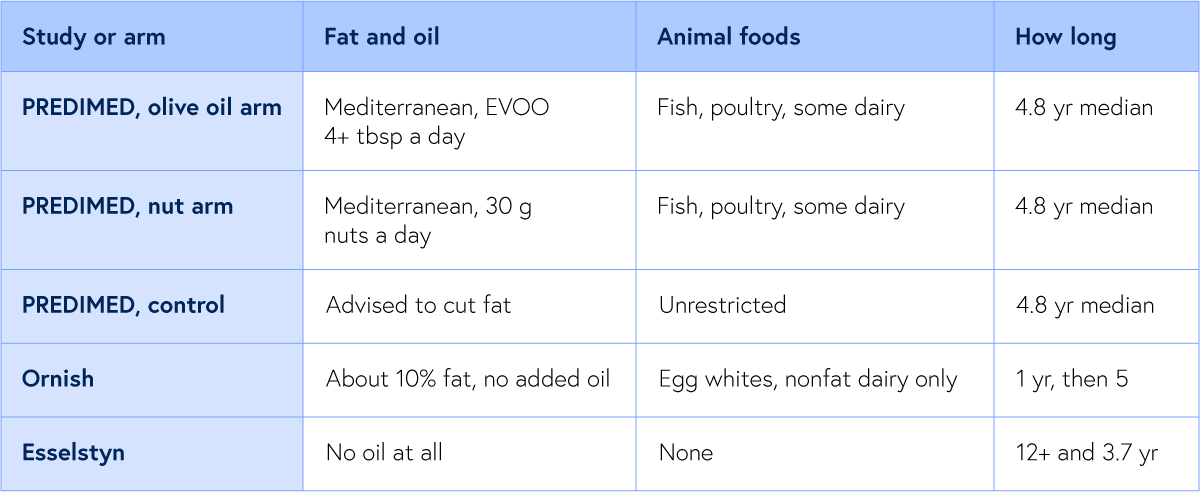
3 studies, 4 plates, very different lengths of time. Only the oil free, near vegan plates were ever filmed reversing disease.
But what did they actually do to the carotid artery in the neck? Below are the exact CIMT measurements, the gold standard ultrasound marker of atherosclerosis, from the same trials.
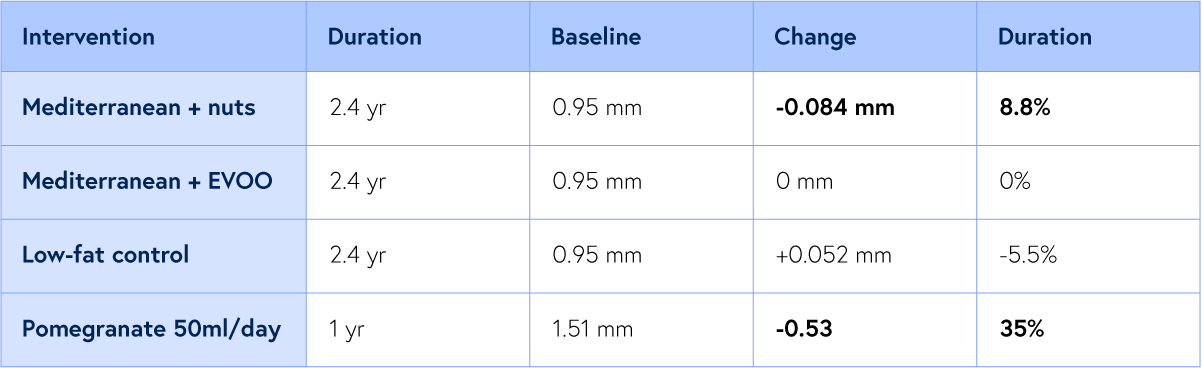
Sala-Vila 2014 (PREDIMED): Internal carotid mean IMT, n=187, 2.4 year median follow up. Aviram 2004: Common carotid IMT, n=10 treated and n=9 control with carotid stenosis, 1 year follow up.
Ornish and Esselstyn measured plaque in the coronary arteries. Predimed did a followup substudy to see the effect of nuts vs olive oil in the Mediterranean diet using the carotid artery wall thickness, which is a more immature plaque. I show what even a single food like pomegranate juice can do reversing CIMT 35% in a year vs Mediterranean diet plus nuts at 8.8% in 2.4 years. Imagine what the Low fat WFPB would reduce.
In fact my own CIMT reduced 53% in just 3 months on Esseltyn’s diet.
Why the Oil Fails to Reverse: The Mechanism
“Oil injures the endothelium, and that injury is the gateway to vascular disease.”
Dr. Caldwell Esselstyn, Jr., MD
Here is the uncomfortable part. It is not only that olive oil fails to shrink plaque. There is evidence, in animals and in the laboratory, that the oil can push in the wrong direction.
At Wake Forest, monkeys fed for 5 years on the monounsaturated fat (oleic acid) that dominates olive oil developed as much coronary atherosclerosis as monkeys fed saturated fat, even though their cholesterol numbers looked better. The fat enriched their LDL particles with a form of cholesterol that settles readily into the artery wall.
In a separate human experiment, a single meal of olive oil dropped the arteries’ ability to relax by about 31 percent within hours.
Fairness demands the caveats, and they are real. Those are monkeys on punishing diets, and a single meal, not years of human imaging. No human imaging trial has shown olive oil growing plaque in people, and over a lifetime olive oil plainly beats butter and beats the refined junk it so often replaces. Olive oil is not poison.
But return to the press. The oil cuts risk because the few polyphenols it retains calm inflammation and slow the oxidation that makes plaque rupture. It makes the plaque quieter. It does not make it smaller, because it is still concentrated liquid fat with the fiber gone and most of the medicine left behind in that bitter water.
A daily pour carries the fat of roughly 100 olives (50g of fat) and only a sliver of their hydroxytyrosol. You are keeping the part that clogs and discarding the part that heals. So eat the olive. The whole fruit holds its polyphenols in the flesh, where some ripe olives carry many times the hydroxytyrosol of the oil. Eat the olive, and leave the bottle for the pan you were going to grease anyway.
Why the Nuts Help Reverse: The Mechanism
“Eating a handful of walnuts every day is a simple way to promote cardiovascular health.”
Dr. Emilio Ros, MD
If the oil is the wrong half of the olive, what is the right prescription?
PREDIMED, read honestly, already named part of it. The nuts.
The trial used an exact recipe, 30 grams a day.
15 grams of walnuts, about 7 walnut halves.
7.5 grams of almonds, about 6 almonds.
7.5 grams of hazelnuts, about 6 hazelnuts.
One small handful, and each carries a different gift.
Walnuts. The highest plant omega 3 of any nut, polyphenols in the papery skin that the gut turns into artery protectors, and the raw material the body uses to make nitric oxide, the molecule that keeps a vessel open. Of more than 1,000 foods once tested for antioxidants, walnuts ranked second. Their deepest work is at the first step of reverse cholesterol transport. In the laboratory, walnut oil raised cholesterol efflux from arterial foam cells by 35 percent, the act of pulling cholesterol back out of the plaque and loading it onto HDL for the trip home. This is the Activate step, where the artery first begins to empty.
Almonds. Vitamin E, magnesium, fiber, and arginine, and a proven drop in LDL and ApoB, the very particles that build the plaque. In a controlled feeding trial, a daily handful raised the mature alpha 1 HDL particles and improved the blood’s capacity to accept cholesterol from cells. This is the Carry step. Almonds give the bloodstream better trucks to haul away the cholesterol the walnuts pried loose, and the vitamin E rides along to keep that cargo from oxidizing on the way to the liver.
Hazelnuts. Plant sterols that sit at the gut wall and compete with cholesterol for the door, blocking its reabsorption so it leaves the body instead of cycling back into the blood. They lower LDL and drop the oxidized cholesterol that tears into the artery. This is the Transfer step, the final out. Hazelnuts show the cholesterol the body delivers to the gut the exit rather than letting it back in, closing the loop the other two nuts opened.
The catch with all three is honest. The benefit fades within a month of stopping. These are not a cure you take once. They are a practice.
One warning belongs here, because more is not better. The dose that shrank plaque was 30 grams, not a bowl. That single handful already carries about 18 grams of fat and close to 190 calories. Double it to 60 grams and you take in roughly 36 grams of fat from nuts alone, which is more than an entire day’s fat allowance on the kind of very low fat diet that actually reverses an active plaque.
This is exactly why Esselstyn keeps nuts off the plate for his heart patients. He is not against the nut. He is against the fat load that rides in with it. Once you are holding total fat under 10 percent of calories to melt a plaque you already have, even one honest handful can quietly push you over the line, and a double handful blows straight past it. So weigh the 30 grams. Treat it as a dose, not a snack.
And then there is the long shot, the food with the largest number on the board. In a small trial, 50 milliliters of pomegranate juice a day, about 2 tablespoons, shrank carotid wall thickness from roughly 1.5 millimeters toward 1 over a single year, a fall near 35 percent, while the untreated arteries thickened. That is several times the effect the nuts produced, in less time. The honesty tax is steep. The study was tiny, only 10 treated patients, and a larger trial came back neutral. The nuts are the sure thing, drawn from thousands. The pomegranate is the long shot.
What do I add to my diet from this?
The 50 ml pomegranate juice. It worked for me.
And after speaking to Dr. Esselstyn a couple of months about the walnuts, I’ve added 2-3 walnuts per day. I put them on my organic sourdough natto arugula sandwich. Delicious!
Moderation Kills: The Case for an Extreme Diet
“Moderation kills.”
Dr. Caldwell Esselstyn, Jr., MD
Dr. Caldwell Esselstyn wrote the most uncompromising book in this entire literature, Prevent and Reverse Heart Disease, and he refused to soften its central sentence.
Moderation kills. Once the disease is in your arteries, he argues, the advice we have all absorbed, a little olive oil, lean meat now and then, everything in moderation, is not a smaller version of the cure. It is a slower version of the disease. Every meal of oil, dairy, or flesh injures the thin layer of cells that lines the artery, the same layer that makes the nitric oxide that keeps the vessel open. Moderation simply relights that injury, a little at a time. In his words, you have to stop pouring gasoline on the fire.
This is not a small claim, because the disease is not a small thing. Cardiovascular disease is the number 1 killer on earth, taking close to 20 million lives a year, near a third of all human death. Our usual answer is mechanical. Around 650,000 stents and bypasses are threaded and stitched into American chests every year, and still the disease holds its place at the top of the list, because a stent reopens a single pipe without touching the illness that clogged it. Moderation, drugs, and surgery, in Esselstyn’s reading, mostly slow a disease that still goes on to claim most of the patients it touches.
His own work points the other way. He took patients with severe, advanced coronary disease, people for whom cardiology had nearly run out of moves, and put them on a plan with no oil, not a drop, no meat, no dairy, no eggs, and leafy greens many times a day.
Their angina faded. Their cholesterol fell. On the follow up angiograms, the blockages visibly reversed.
Hence his favorite line, that heart disease is a toothless paper tiger that need never exist, and if it does exist, need never progress, nothing more than a benign foodborne illness. That is the whole of it. No one need perish from this disease. The control was never in the pill or the operating room. It was on the plate all along.
A Request
Each Friday, I upload a new Youtube video. Please like, comment and subscribe so I can help many others in your network and beyond, it’s my mission to help people avoid the same fate as Rob, the same fate as I could have had. Heart attack, stroke or sudden death.
https://www.youtube.com/@DrKevinHam
My latest video is going viral :) My #1 meal to unclog arterial plaque. Thank you.
What to Start Now
If you are reading this with a calcium score above zero, or a family history that worries you, or a friend who suffered what Rob did
1. CAST. Cut out the harmful foods that harm your endothelium
No oils. No saturated fats. No cholesterol. No avocados. No eggs. No dairy. No meat. No seafood. No nuts except a few walnuts and perhaps almonds and hazelnuts.
No refined sugars (white flour/bread/pastries/white rice etc)
2. Add the foods that heal your endothelium cells of your arteries
Greens 6x/day (a handful)
Two to three Whole food Plant-based meals: veggies, whole grains, fruits, beans.
This is how plaque reverses. This is how compounding pays out on the side of life.
Your Question
Questions worth exercising with
For yourself. For someone you love. Answer them in the quietness of your day.
What changes will you make starting today?
For Someone You Love
There is someone in your life running and falling. You thought of them. Send this to them. Your loved ones just need the information to act and a guide to help them.
Keep going. The race is long, the road is beautiful, and the body was built to heal.
Grace, strength and love to you.
MORE READINGS YOU’LL ENJOY
Health
Reversing My 77% Heart Plaques
Stats Say You Likely Have Heart Plaque
The Healing Power of Food: Nitric Oxide
Meaning
I pray you unlock your heart to reach the height of your full potential by discovering your calling.
Kevin Ham, MD
Appendix
The summary of the referred exercise studies:
1. Estruch R, et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N Engl J Med. 2013, and 2018 reanalysis.
More than 7,000 high risk Spaniards in 3 arms. Both Mediterranean arms cut events about 30 percent. Primary endpoint events: olive oil 96 (3.8 percent), nuts 83 (3.4 percent), control 109 (4.4 percent), 288 in total. The trial measured events, not plaque.
2. Sala-Vila A, et al. Changes in ultrasound assessed carotid intima media thickness and plaque with a Mediterranean diet. Arterioscler Thromb Vasc Biol. 2014;34:439 to 445.
In the long carotid substudy, the nut arm regressed internal carotid IMT and plaque height while the olive oil arm did not change. Same diet, only the nuts moved the wall.
3. Ornish D, et al. Lifestyle Heart Trial. Lancet. 1990;336:129 to 133. Follow up: JAMA. 1998;280:2001 to 2007.
A 10 percent fat whole food plant based program with no added oil. Coronary stenosis regressed about 8 percent in the treated arm while controls worsened nearly 28 percent. Controls had more than twice the cardiac events. The only diet ever filmed reversing a coronary.
4. Esselstyn CB, et al. A way to reverse coronary artery disease. J Fam Pract. 2014;63:356 to 364.
198 patients who adhered to an oil free plant based plan. 99.4 percent avoided a major cardiac event over years of follow up.
5. Esselstyn CB. Prevent and Reverse Heart Disease. Avery, 2007.
Source of the moderation kills and toothless paper tiger framing, and the case that half measures slow a disease that still claims most patients.
6. Rudel LL, et al. Dietary monounsaturated fat and coronary atherosclerosis in African green monkeys. Arterioscler Thromb Vasc Biol. 1995, with the cholesteryl oleate mechanism, J Clin Invest. 1997.
Over 5 years, the monounsaturated fat that dominates olive oil produced coronary atherosclerosis comparable to saturated fat despite better cholesterol, by enriching LDL with cholesteryl oleate. The strongest animal evidence that the oil can promote plaque.
7. Vogel RA, Corretti MC, Plotnick GD. Postprandial effect of components of the Mediterranean diet on endothelial function. J Am Coll Cardiol. 2000;36:1455 to 1460.
A single olive oil meal reduced flow mediated dilation by about 31 percent within hours. An acute mechanistic signal, not a measure of plaque.
8. Aviram M, et al. Pomegranate juice consumption and carotid intima media thickness. Clin Nutr. 2004;23:423 to 433.
50 milliliters a day shrank common carotid IMT by roughly 30 to 35 percent over a year in 10 treated patients, while controls thickened. A dramatic but small signal. A larger trial was neutral.
Subscribe to my Compounding Wisdom newsletter and start transforming your life. ham.com
Subscribe to my YouTube channel @DrKevinHamfor videos on how I reversed my clogged arteries in 3 months, the top foods that clear your arteries, and the first principles of health that can save your life. Like, share and subscribe — it could save the life of someone you love.
Carnivore vs Ketogenic vs Vegan
Which diet reverses plaque best?
Which diet reverses plaque best?
Dr. Kevin Ham, MD
“So whether you eat or drink, or whatever you do, do all to the glory of God.”
1 Corinthians 10:31
Since my YouTube channel has had a video hit a million and a handful of 100,000+ views, I’ve had many people wonder about other diets. I wanted to comb through the medical studies to see what diets actually reverse plaque. I used to eat a lot of meat, seafood, dairy, and fruits, but not a lot of salads or beans. Now most of my meals are salads, veggies, beans, sourdough breads and modest fruits.
I would gladly eat meat, seafood, and dairy, but I sincerely wish to reverse my plaque and not die of a heart attack, stroke, or any metabolic disease, which I put diabetes, autoimmune and cancer in that category as well. As I’ve looked at the evidence, knowing that I have major blockages in my heart arteries and that my Bruch’s membrane (the wall between my retinal vessels and my retina) is brittle, I’ve been pretty disciplined for the past year, reading medical studies and implementing what I believe based on evidence to reverse both my eye and heart disease. So far, so great.
Every drink and food I put into my mouth, I consider whether it is making me healthier or sicker. Closer to life or further from death. Of course, I enjoy a great tasting meal. The irony is that I have made my meals very delicious. I absolutely look forward to many of my meals. Some of them I am still working on making delicious. I never imagined myself being on a ‘vegan’ or what we call a 10% low-fat whole food plant-based (WFPB) diet for a year now. May 9 marked my first anniversary. Wow. I committed at least three years of my life to this WFPB diet protocol, fasting protocol and HIIT protocol. I view myself as being the Roger Bannister of plaque reversal. He was the first to run a mile under 4 minutes.
Although my role model is Dr. Joe Crowe, who reversed 100% of his LAD coronary plaque in 32 months, he was only 44 at the time. His plaque was 11 years younger than mine, so it had more fibrous atheroma (Type 3 plaque), and mine is more Type 4 and 5 (calcified and mixed). It’s like the difference between curing Stage 2 cancer vs Stage 3 vs Stage 4 cancer. I view my diet as 80/20, contributing 80% of the results, with exercise and fasting accounting for the remaining 15%-20%. Of course, sleep, stress, and genetics also play a role.
So in this article, I would like to examine the evidence for and against two of the four most touted and often controversial diets. Carnivore vs Ketogenic vs Low-fat Vegan (plant-based) diets. Each has its evangelists. Right now, I am in the low-fat WFPB camp. Ready?
The Carnivore Diet
“Every moving thing that lives shall be food for you.
And as I gave you the green plants, I give you everything.”
Genesis 9:3
After Noah’s flood, God commanded Noah to eat every moving thing. In other words, fish, birds, creeping things, animals, in addition to every green plant, were the diet for ten generations from Adam to Noah.
The carnivore diet was popularized by orthopedic surgeon Shawn Baker, who stipulated that it be based solely on animal foods. Meat, eggs, dairy, but no plants. The lion is its role model. Ribeye for breakfast. Complete opposite of WFPB.
The carnivore literature, as far as I could find, had no randomized controlled trials for plaque reversal. But let’s look at the lipid endpoints, which are different from plaque reversal endpoints.
The first study we examine is a Harvard social media survey of 2,029 self-selected adults, led by Belinda Lennerz and David Ludwig at Boston Children's Hospital. The respondents had eaten carnivore for a median of 14 months. They reported high satisfaction. LDL cholesterol in the subset who provided lab values averaged 172 mg/dL.
My only risk factor for my heart disease was a high LDL of 168 mg/dl. I was eating a high-saturated-fat diet of meats, seafood, dairy, and complex carbs. My hsCRP has been only 0.3 for the past 6 years.
So far, I don’t think I would reverse my plaque on this carnivore diet.
The second study: a German exploratory study by Rainer Klement and Johanna Matzat, published in Cureus in April 2025. 23 adults submitted paired blood panels before and after at least one month on the diet. Total cholesterol rose from a median of 224 to 305 mg/dL. LDL rose from 157 to 256. Both shifts were statistically significant. The authors wrote:
The significant elevation of total and LDL cholesterol concentration is striking and warrants further investigation into potential adverse effects.
Klement RJ, Matzat JS. Cureus. 2025;17(4):e82521
The third was a scoping review published in Nutrients in January 2026 by Lietz and colleagues. They searched the entire global literature on the carnivore diet. Nine human studies met the inclusion criteria. Zero were randomized. Zero were long-term. Zero captured hard cardiovascular endpoints. Their conclusion was the gentlest possible no:
The Carnivore diet (CD) may offer short-term health benefits but carries substantial risks of nutrient deficiencies, reduced intake of health-promoting phytochemicals, and the development of cardiovascular disease. At this time, long-term adherence to a CD cannot be recommended.
Lietz A, Dapprich J, Fischer T. Nutrients. 2026;18(2):348
We should also consider George Mann’s studies on the Masai, an African tribe that is said to eat meat, dairy, and blood and to have no cardiovascular disease. Mann found in 1964 that they were lean, fit, and their ECG and blood pressure were normal. They consumed 3000 calories but were so active and fit from hunting and roaming that they were metabolically fit. Guess who this reminds me of? Yes, my friend Rob Thompson, who climbed the Matterhorn mountain three times. He died of a sudden heart attack at age 58.
They also had periods of fasting between meals. It also reminds me of me. HR 42 bpm. BP 105/65. Able to ride 100 km on my bike at fast speeds, up mountains every week with relative ease. Coronary arteries clogged 77%, 55%, 45% in every vessel!
In early 1972, Mann did an autopsy study on 50 Masai. Most of the population did not reach past 60, so they were still relatively young. What was found was astounding! Major atherosclerosis in their arteries. But their arteries were larger. Let’s see what Mann reported.
A field survey of 400 Masai men and additional women and children in Tanganyika indicates little or no clinical or chemical evidence for atherosclerosis. Despite a long continued diet of exclusively meat and milk the men have low levels of serum cholesterol and no evidence for arteriosclerotic heart disease.
he average total cholesterol is about 130 mg/dL in men aged 25 to 55. Lean. Active. No clinical signs of CVD on physical exam or EKG. This is the paper the carnivore community cites. Mann himself became a public critic of Ancel Keys on the strength of it.
Mann's 1972 paper, American Journal of Epidemiology, 95(1):26-37
This was the autopsy study. Fifty Maasai men. Hearts and aortae were examined under the microscope. Verified verbatim abstract:
The hearts and aortae of 50 Masai men were collected at autopsy. These pastoral people are exceptionally active and fit and they consume diets of milk and meat. The intake of animal fat exceeds that of American men. Measurements of the aorta showed extensive atherosclerosis with lipid infiltration and fibrous changes but very few complicated lesions. The coronary arteries showed intimal thickening by atherosclerosis which equaled that of old U.S. men. The Masai vessels enlarge with age to more than compensate for this disease. It is speculated that the Masai are protected from their atherosclerosis by physical fitness which causes their coronary vessels to be capacious.
Read those two sentences together.
Coronary intimal thickening that equalled that of old U.S. men. Extensive atherosclerosis in the aorta. The Maasai had the disease. They just weren't dying from it.
The protection was not the diet. The protection was three things the diet did not provide.
One. Compensatory arterial enlargement. Their coronary vessels dilated as plaque grew, preserving the lumen. We now call this positive remodelling, the Glagov phenomenon, first formally described by Seymour Glagov in 1987 in the New England Journal of Medicine. The Maasai were the original case series.
This arterial enlargement, and I believe also the collateral vessels, which are natural bypasses the body makes, allow more blood flow past the severe obstructions.
Two. Extreme physical activity. The Maasai warriors walked 15 to 20 kilometres per day, herding cattle, in semi-fasting states between feedings. The Mbalilaki 2010 study in the British Journal of Sports Medicine found that Maasai daily energy expenditure was roughly twice that of urban Bantu Tanzanians.
Three. Extreme leanness. Mean BMI around 20. Frequent caloric restriction between feedings. Genetic adaptations to a milk-heavy diet (the Maasai are among the most lactase-persistent populations on earth).
If you have seen any studies that show plaque reversal with the carnivore diet, I would love to read them.
I can see how a carnivore diet could eliminate some of the processed, sugar-laden food that many people eat and have a great metabolic effect, as well as cover some of the nutritional deficiencies from the “Western diet”.
But long term, I believe a carnivore diet will increase the risk of disease and death from heart attacks, strokes and cancer. After all, red meat is classified as a Class 2 carcinogen. I await studies showing plaque reversal with a carnivore diet.
The Ketogenic Diet
“And after fasting forty days and forty nights, he was hungry.”
Matthew 4:2
The ketogenic diet was born to treat epileptic seizures. When fasted, childhood seizures would drastically reduce or disappear on day 4 or 5. But the kids needed to eat, and they discovered that removing carbs (glucose) from their diet mimicked a fast. This was popularized by Robert Atkins (the Atkins diet). Eat fat and protein and remove carbs. The body then converts fats and carbs in the liver to ketones. The body can run on ketones. Glucose falls. Insulin falls. Hunger dissolves. Weight loss ensures. It is great for diabetes and weight loss.
I’ve developed a protocol for diabetics, high blood pressure, and weight loss that has quite remarkable results based on this and other dietary protocols. Reversing diabetes is much easier than reversing plaque. Of course, diabetes is also a very high risk factor for heart attacks and strokes, so although I have excellent glucose control and insulin sensitivity.
The ketogenic data is more interesting than the carnivore data because it is recent and contradictory.
In August 2024, Matthew Budoff and Nicholas Norwitz published the KETO Trial in JACC Advances. Eighty lean ketogenic dieters, averaging 4.7 years on the diet, with LDL cholesterol above 190, were matched one-to-one with Miami Heart cohort controls whose LDL was 149 milligrams per deciliter lower. Cross-sectional coronary CT angiography asked a simple question: Does the lean mass hyper-responder phenotype carry more plaque?
The answer, in the authors' own words:
Coronary plaque in metabolically healthy individuals with carbohydrate restriction induced LDL-C ≥190 mg/dL on KETO for a mean of 4.7 years is not greater than a matched cohort with 149 mg/dL lower average LDL-C. There is no association between LDL-C and plaque burden in either cohort.
Budoff M, Manubolu VS, Kinninger A, Norwitz NG, et al. JACC Advances. 2024;3(8):101109
The comparison here is against a matched cohort where there is no cited plaque reversal. The endpoint I would like to model is any protocol or diet that reverses plaque, and what kind of plaque and the degree of plaque reversal.
The keto community received the paper as justification. The cardiology community received it with caution. A cross-section is a single photograph. It tells you where you are. It does not tell you where you are going.
In April 2025, the same research group published the longitudinal answer. Adrian Soto-Mota and Nicholas Norwitz followed 100 ketogenic dieters in the lean mass hyper responder phenotype for one year with serial coronary CT angiography. The endpoint was a change in noncalcified plaque volume. The paper, titled "Plaque Predicts Plaque, ApoB Does Not," reported a median plaque progression of 18.9 cubic millimetres in one year. A 42.8 percent relative increase. The authors wrote:
In lean metabolically healthy people on KD, neither total exposure nor changes in baseline levels of ApoB and LDL-C were associated with changes in plaque. Conversely, baseline plaque was associated with plaque progression.
— Soto-Mota A, Norwitz NG, Manubolu VS, et al. JACC Advances. 2025;4(7):101686
The story, so far, is that elevated LDL in this phenotype does not translate cross-sectionally to greater plaque than matched controls, but the same phenotype shows measurable plaque progression over one year of longitudinal imaging. Progression. Not reversal.
The ketogenic diet has one other claim, and it is real. In 2019, Shaminie Athinarayanan and the Virta Health group, including Sarah Hallberg, Jeff Volek, and Stephen Phinney, published a two-year open-label trial of 262 type 2 diabetic adults on a well-formulated ketogenic protocol with continuous remote care. HbA1c fell from 7.6 to 6.3 percent. Patients lost about 12 percent of body weight. Many came off insulin. The five-year extension published in 2024 reported 20 percent sustained diabetes remission and 32.5 percent reversal to HbA1c below 6.5 percent on no medication or only metformin. Type 2 diabetes is real. Ketosis reverses it. That is the legitimate ketogenic claim.
It is, however, not a coronary endpoint. No ketogenic trial has ever documented coronary plaque regression on imaging.
The Plant Based Diet
“Test your servants for ten days; let us be given vegetables to eat and water to drink. Then let our appearance and the appearance of the youths who eat the king's food be observed by you, and deal with your servants according to what you see. At the end of ten days it was seen that they were better in appearance and fatter in flesh than all the youths who ate the king's food.”
Daniel 1:1,12-15
The low-fat, plant-based diet, advanced by Dean Ornish and Caldwell Esselstyn since the 1980s, asks the opposite. No oil. No animal products. Whole foods with less than 10 percent fat. The Tarahumara as model. A bowl of beans and greens for breakfast.
Next week, we will look at plaque reversal studies for a whole-food, plant-based diet, and then also examine the Mediterranean diet for plaque reversal. This is a much more interesting comparison, in my opinion.
Plaque reversal on imaging has been documented only by Ornish and Esselstyn. No carnivore study has ever imaged the arteries. No ketogenic study has ever reported plaque regression. The ketogenic phenotype showed measurable plaque progression at one year in KETO-CTA.
LDL and ApoB: Plant based drives both sharply down. My LDL decreased from 168 to 61 mg/dL. My ApoB 45. Carnivore drives both consistently up, sometimes doubling within months. Keto raises both modestly on average and dramatically in the lean responder phenotype.
If you have established coronary plaque on a CT angiogram or calcium score, the imaging trials are the endpoints of which dietary protocols shrink it.
A Request
Each Friday, I upload a new YouTube video. Please like, comment and subscribe so I can help many others in your network and beyond. It’s my mission to help people avoid the same fate as Rob, the same fate as I could have had. Heart attack, stroke or sudden death.
https://www.youtube.com/@DrKevinHam
My latest video is going viral :) My #1 meal to unclog arterial plaque. Thank you.
What to Start Now
If you are reading this with a calcium score above zero, or a family history that worries you, or a friend who suffered what Rob did
Get the numbers. ApoB, Lp(a), CIMT, CT calcium. You cannot manage what you do not measure. If your doctor will not order them, find one who will.
Eat real food. Whole, plant-based, low in added fat. The Esselstyn protocol is the most effective in all the studies I have seen for plaque reversal and arrest.
Walk, cycle, run, or move. Every day before meals and especially after meals. Move your body the way your great grandparents moved theirs for 30 minutes to an hour each day. Take the stairs.
Sleep. Eight hours. Without an alarm if you can manage it.
Then repeat.
This is how plaque reverses. This is how compounding pays out on the side of life.
Your Question
Questions worth exercising with
For yourself. For someone you love. Answer them in the quietness of your day.
What diet shrinks plaque and why aren’t you on it?
For Someone You Love
There is someone in your life running and falling. You thought of them. Send this to them. Your loved ones just need the information to act and a guide to help them.
Keep going. The race is long, the road is beautiful, and the body was built to heal.
Grace, strength and love to you.
MORE READINGS YOU’LL ENJOY
Health
Reversing My 77% Heart Plaques
Stats Say You Likely Have Heart Plaque
The Healing Power of Food: Nitric Oxide
Meaning
I pray you unlock your heart to reach the height of your full potential by discovering your calling.
Kevin Ham, MD
Appendix
The summary of the referred exercise studies:
1. Lennerz BS, Mey JT, Henn OH, Ludwig DS. Behavioral Characteristics and Self-Reported Health Status among 2029 Adults Consuming a "Carnivore Diet." Curr Dev Nutr. 2021;5(12):nzab133.
Online survey of 2,029 self-selected carnivore dieters at median 14 months. High subjective satisfaction. Average LDL 172 mg/dL in subset with labs. No imaging. No cardiovascular endpoints. (28 words)
2. Klement RJ, Matzat JS. Subjective Experiences and Blood Parameter Changes in Individuals From Germany Following a Self-Conceived "Carnivore Diet." Cureus. 2025;17(4):e82521.
Twenty four German adults with paired pre and post panels. Total cholesterol rose 224 to 305 mg/dL. LDL rose 157 to 256 mg/dL. Both statistically significant. (26 words)
3. Lietz A, Dapprich J, Fischer T. Carnivore Diet: A Scoping Review of the Current Evidence, Potential Benefits and Risks. Nutrients. 2026;18(2):348.
Scoping review of nine human studies, 2021 to 2025. Zero randomized. Zero captured cardiovascular endpoints. Long term adherence to a carnivore diet cannot be recommended. (25 words)
4. Budoff M, Manubolu VS, Kinninger A, Norwitz NG, et al. Carbohydrate Restriction-Induced Elevations in LDL-Cholesterol and Atherosclerosis: The KETO Trial. JACC Adv. 2024;3(8):101109.
Eighty lean keto dieters, mean 4.7 years on diet, LDL above 190, matched against Miami Heart controls with 149 mg/dL lower LDL. Cross sectional plaque burden equal. (28 words)
5. Soto-Mota A, Norwitz NG, Manubolu VS, et al. Plaque Predicts Plaque, ApoB Does Not: Longitudinal Data From the KETO-CTA Study. JACC Adv. 2025;4(7):101686.
One hundred lean keto dieters, serial CT angiography at one year. Median plaque progression 18.9 cubic millimeters, a 42.8 percent increase. ApoB not associated with progression. (27 words)
6. Athinarayanan SJ, Adams RN, Hallberg SJ, et al. Long-Term Effects of a Novel Continuous Remote Care Intervention Including Nutritional Ketosis for the Management of Type 2 Diabetes. Front Endocrinol. 2019;10:348.
Two year open label trial in 262 type 2 diabetic adults on Virta ketogenic protocol. HbA1c fell 7.6 to 6.3. Twelve percent body weight loss. Insulin reduced. (27 words)
7. Ornish D, Brown SE, Scherwitz LW, et al. Can lifestyle changes reverse coronary heart disease? The Lifestyle Heart Trial. Lancet. 1990;336(8708):129.
Forty eight patients randomized to whole food vegetarian intervention or usual care. Eighty two percent of intervention patients regressed coronary stenosis at one year on quantitative angiography. (27 words)
8. Ornish D, Scherwitz LW, Billings JH, et al. Intensive lifestyle changes for reversal of coronary heart disease. JAMA. 1998;280(23):2001.
Five year follow up of Lifestyle Heart Trial. Intervention group regressed 7.9 percent. Control group progressed 27.7 percent. Control group experienced 2.47 times more cardiac events. (26 words)
9. Esselstyn CB Jr, Ellis SG, Medendorp SV, Crowe TD. A strategy to arrest and reverse coronary artery disease. J Fam Pract. 1995;41(6):560.
Twenty two severe coronary patients on plant based protocol with cholesterol below 150 mg/dL. Eleven completers imaged at 5.5 years. All eleven showed disease arrest. Eleven lesions regressed. (28 words)
10. Esselstyn CB Jr, Gendy G, Doyle J, Golubic M, Roizen MF. A way to reverse CAD? J Fam Pract. 2014;63(7):356.
One hundred ninety eight cardiovascular patients counseled in plant based nutrition. Mean follow up 3.7 years. Of 177 adherent patients, 99.4 percent free of recurrent cardiac events. (27 words)
Subscribe to my Compounding Wisdom newsletter and start transforming your life. ham.com
Subscribe to my YouTube channel @DrKevinHamfor videos on how I reversed my clogged arteries in 3 months, the top foods that clear your arteries, and the first principles of health that can save your life. Like, share and subscribe — it could save the life of someone you love.
When Your Life Flashes Before You
What will you do at that moment?
What will you do at that moment?
Dr. Kevin Ham, MD
“And some of the wise shall stumble, so that they may be refined, purified, and made white, until the time of the end, for it still awaits the appointed time.”
Daniel 11:35
I rode the Levi Gran Fondo in Napa Valley. My longest ride of the year. 113 miles (183 km) with 3000m elevation. 8 hours in the saddle. Going at zone 2 speed. Steady but not hard. They were hard hills with 10-16% grade elevations. Average heart rate was only 135 bpm. I felt great and recovered well.
I had dinner with Rob’s wife, and we spoke about Rob, who passed away too early from a sudden heart attack. I told her about my dreams of writing a book with him in it and about the YouTube channel I had started, so that others might not suffer the same fate as Rob. She is also a physician, so I told her how I reversed my carotid plaque and am working on my coronary plaque. How carotid plaque forms later in the 30s, while coronary plaque starts in childhood. So coronary plaque is older and harder to reverse. I expect it to take me 3 years plus to reverse my plaque. I think of it as “Stage 4 heart disease,” except it doesn’t metastasize like cancer in the same way.
She told me how they spread Rob’s ashes in the mountain where he ran. I was staying in SF, Sausalito, so on the day I was heading back home, I went to visit Rob and pay tribute. I parked at the foot of the mountain in Tennessee Valley and hiked up 45 minutes. It was quite foggy at the top, and I couldn’t see the rock where his beloved family had spread his ashes, overlooking the Golden Gate and Pacific Ocean. I shot a video tribute to Rob at the top and then started running down the mountain. But I missed a turn and got lost. I had to run back up the mountain. I was late for my lunch meeting with one of Rob’s best friends, so I started running down the mountain. I was about a mile away, and I saw some people in the distance. I was catching up and felt great. Then WHAM….
The Height and Speed of the Fall
“For the righteous falls seven times and rises again, but the wicked stumble in times of calamity.”
Proverbs 24:16
My face hit the dirt stony path hard. My left knee, shoulder and right hand had searing pain, but most of all, the pain in my face. I quickly made an inventory to go down the checklist of the Glasgow Coma Scale: Could I open my eyes and see? Could I comprehend and think? Could I move my appendages and breathe? Did I lose consciousness? Just a lot of pain. I immediately knew I would need stitches, that I might have fractured my face, but my eyes were ok. I lay on the ground, thinking that the person I saw heading up the hill would soon arrive near me. Wow, what a searing pain in my face. It’s not going to look pretty.
I got up, and there was a tremendous amount of gravel in my mouth. I spat about a half dozen times as I started running down the mountain again, this time at a much slower pace.
The young man looked at me and immediately asked if I needed help. I asked if he had some water for my face. He had one of those backpacks that water came out of and sprayed my face, then my right hand. It stung a lot. He said I had a bad gash and asked if he should call 911. I said I think I am okay. He suggested I use my jacket to stop the bleeding from my facial laceration.
I had been holding my brand-new jacket, but I immediately put it against the left side of my face. It felt better. This was an expensive jacket, gray/beige and would get stained with my blood. It was necessary. I thanked him and continued running. The next person I saw asked if I needed help. “I have some bandages.” Oh, you are so kind. Thank you. She gave me her whole stash of small and large bandages. I put them in my pocket and ran for the next mile, and each person who saw me asked if I needed help. I felt so grateful for the kindness of strangers.
I finally got to my rental SUV. I took a look at myself in the mirror, and my initial assessment seemed correct. I texted Gordon, Rob’s friend, that I had fallen while running down the mountain. It was already noon, the time I was supposed to be at his home. I told him I would try to make it as fast as possible, but I still needed to check out of my hotel. He said to take my time.
When I arrived at the hotel, the hotel manager had a look of horror on her face when she saw my face, which was covered with my own blood. She remarked that the left lens of my glasses was badly scratched. I could still see slightly beyond this lens, but my vision itself was not affected. Thank you, Lord.
I got in the shower and let out a quiet yelp as the water hit my wounds. But I knew I had to get the dirt and rocks out. They were deeply embedded. Road rash is what we call it when we crash on our bikes. I didn’t know the same thing could happen while running, but I was running downhill quickly.
I lost track of time as I let the running water cleanse my wounds.
Then I applied squalene, a shark liver oil I always carry with me. It’s so great for burns and cuts. It instantly soothed the pain. I knew it was my saving grace, helping me heal faster.
Then I put the bandages on. The small one on my face was too small. I put the much larger one on my face. You could barely see the facial wounds. I was beginning to get a black eye.
I bandaged my shoulder and knee. Tried my hand, but it was hard to get. The hotel manager applied a large dressing and secured it with tape. I was so appreciative and grateful.
One Word: Providential
“The heart of man plans his ways but the Lord establishes his steps.”
Proverbs 16:9
Then I texted Gordon. I am on my way.
He greeted me at his door with open arms. We hugged. Instantly, I felt we were friends. We were bonded by Rob. He had run the very mountain range I was on just two days with Rob before Rob died. He showed me a photo they had taken on that run. Precious. I had never taken a single photo with Rob because we were so engaged in our conversations. Rob was supposed to visit me in Vancouver on the day he passed. We were connected by Rob. I wanted to meet Gordon to hear his “Rob stories.” I wanted to know what it was like to climb these big Swiss mountains. Rob had been training on the elliptical the morning he passed, so he could climb his next big mountain. Mt Eiger, . Gordon is planning to do it on his own behalf. What a tribute! I wanted to hear all about it. As he described how precipitous it could be, I realized that I was speaking with hearts of courage and grit.

I had not eaten all day. I was hiking and running up and down the mountain for 2.5 hours, covering over 600m of elevation. I was running, not on my bike. I wished I had my bike :) That would have been much easier. I’m not a runner.
I gladly ate the salad Gordon had ready for me. We spoke so much, full of heart, questions, and stories. I felt full of love, purpose and meaning.
I had to leave after an hour and a half to catch my flight home. When I had fallen, I already planned to go to the ER when I arrived in Vancouver. Gordon had called Anita, Rob’s wife, who was expecting me, so she could stitch me up, but I preferred speaking with Gordon and thought that if I got a scar, it would be in memory and honour of Rob.
I got six stitches under my left eye at Urgent Care. The Nurse Practitioner who stitched me up asked if I preferred a Plastic surgeon. I said I trusted him. Let’s do it. But X-rays were not available at the urgent care.
The next morning, I felt some nasal discharge. I blew my nose gently, worried about a facial fracture. I saw blood in my discharge. I went to the ER and then did CT facial scans, which revealed a minor displaced fracture of my anterior maxilla. Conservative management and follow-up in three months.
I sent photos of my face and shoulder to Anita and Gordon. “Oh my goodness! …” were the words in common.
Rapid Healing
I thought about how I could heal faster. I decided to ground myself, barefoot on the lawn, and get some sun. So the next two days, I worked outside in my backyard for hours, feet on the grass. I had also planned a three-day fast from Sunday to Wednesday. I was skeptical about doing it because of my accident, but after thinking deeply about it, it made sense that autophagy from fasting could heal me faster. I decided to do a two-day fast and ride my bike for an hour each day. Why? To accelerate blood flow and mimic a longer fast by stacking exercise with fasting. My wife was upset I was already biking, but I told her to look at my eye. Half of my black eye had dissipated. My urine was bright yellow, even though I had drunk a lot of green tea. My hemoglobin was breaking down, just like jaundiced babies with sunlight.
I had so many messages of love and care that my heart overflowed with gratitude. My body was bruised and battered, but my heart was serene and boundless.
The principles I have learned to heal my wet macular degeneration, a severe cause of blindness, and to heal my heart have helped me heal my wounds speedily and remarkably.
Today is day 6, and I took out my six stitches using tweezers and a small pair of scissors. I improvised as I didn’t have the proper equipment. Will I scar? Perhaps a little. It will be a brand of honour in memory of Rob, bonded by heart with Gordon and Anita, my dear friends. Here’s to you Rob, buddy!

The morning after my fall.

5 days later.
I thank Anita and Gordon, the kindness of all the strangers who offered their help, their water, their bandages and their care and concern. Even the customs officer at the border wished me well. My family, my friends who reached out as they heard I had broken my face, my first fracture.
You never know what will befall you. I don’t take a moment or a day for granted. As I lay on the ground, in pain, a Bible verse came to mind. “He will not let your foot stumble.” “He will establish your path.” I had stumbled hard. But I knew I would be great. I knew I would get back up. I knew I would become wiser, stronger and humbler. I just knew. Running downhill can be dangerous. Gordon imparted wisdom to me. “Small steps, feet slightly facing outwards, and hiking poles.” Thank you.
I rode to church yesterday. 42 km. The distance of a marathon. The outer man decays, but the inner man is renewed day by day.
I was going to write about how stacking the various proven strategies of diet, focused proven dietary strategies, HIIT exercise and fasting leads to remarkable results, but I got carried away with my own personal story. It felt like a keystone moment in my life. The beginning of a new chapter.
My prayer is that if you are suffering from an illness or a wound, the body has remarkable healing abilities. Nature has remarkable healing abilities. Food, exercise, rest, and sleep have remarkable healing abilities. Faith and God have remarkable healing abilities. Love has remarkable healing abilities.
I am full of love, heart, and gratitude. To you, to the kindness and love in our hearts and the grace, mercy and love of God.
A Request
Each Friday, I upload a new Youtube video. If you could like, comment and subscribe so I can help many others in your network and beyond, it’s my mission to help people avoid the same fate as Rob, the same fate as me.
https://www.youtube.com/@DrKevinHam
My latest video is going viral :) My #1 meal to unclog arterial plaque. Thank you.
Your Question
“The educated soul can be healthy through its lifestyle, set by its heart and its mind and translated into the body. Heartset first, then Mindset, it then appears in Bodyset.”
Questions worth exercising with
For yourself. For someone you love. Answer them in the quietness of your day.
What are your healing principles that you employ each day? For your body, for your soul, for your spirit?
For Someone You Love
There is someone in your life running and falling. You thought of them. Send this to them. Your loved ones just need the information to act and a guide to help them.
Keep going. The race is long, the road is beautiful, and the body was built to heal.
Grace, strength and love to you.
MORE READINGS YOU’LL ENJOY
Health
Reversing My 77% Heart Plaques
Stats Say You Likely Have Heart Plaque
The Healing Power of Food: Nitric Oxide
Meaning
I pray you unlock your heart to reach the height of your full potential by discovering your calling.
Kevin Ham, MD
Subscribe to my Compounding Wisdom newsletter and start transforming your life. ham.com
Subscribe to my YouTube channel @DrKevinHamfor videos on how I reversed my clogged arteries in 3 months, the top foods that clear your arteries, and the first principles of health that can save your life. Like, share and subscribe — it could save the life of someone you love.
Statins Arrest Heart Disease. Exercise Can Reverse it.
It’s not just theory anymore.
It’s not just theory anymore.
Dr. Kevin Ham, MD
“He has made everything beautiful in its time. He has also set eternity in the human heart; yet no one can fathom what God has done from beginning to end.”
Ecclesiastes 3:11
I completed the Levi Gran Fondo. 113 miles, 3000m of climbing and 8 hours in the bike saddle. But the most important stat: my average heart rate was just 135 beats per minute (bpm) despite the huge effort. I did take it ‘easier’ just going at zone 2 effort, applying the arterial pressure wash throughout, supercharging my HDL to reverse plaque. I felt great.
One fellow rider asked me, “How do you know you won’t get a hard attack on these hard climbs?” The simple answer. I don’t truly know. But I have 0% low attenuated plaque, my heart flow is improving, so I am doubling down, treating my plaque as Stage 4 heart disease.
Let me tell you, some hills were very challenging. 400m with 10%-16% grade elevation. But I trained on 25% grade in the big, hard ring for years, so mentally, seeing these didn’t faze me at all, and I just befriended them as my therapeutic medicine to reverse my plaque.
In my last newsletter, Does Exercise Reverse Plaque, many readers asked me about those who could not do High Intensity Interval Training (HIIT).
First, HIIT is just relative to your maximum heart rate, which is a rule of thumb: 220 minus your age. So, walk briskly for x period of seconds or minutes where it is hard to talk. That’s HIIT. As your body chemistry changes with your CAST Reversal Diet, increase your HIIT duration and intensity as tolerated. Note that exercise is more of a mental exercise than physical exercise.
And for the most severe cardiac patients, which Dr. Esselstyn treated, who had bypasses, stents, meds and had no more hope, he arrested and reversed their heart disease for at least the next 14 years and beyond. These were effectively “Stage 4” Heart disease patients. It’s quite remarkable. He did not advise or prescribe any exercise. In fact, his patients could barely even walk across the room without angina or claudication. Even shaving was an effort for some.
But the ones who exercised improved a lot, like Dr. Joe Crowe, younger at 44, who reversed his severe LAD blockages in just 32 months. I asked Dr. Esselstyn last month if Dr. Crowe exercised. He said, “Yes, he did.”
While I am 55 and my plaque is 11 years older than Dr. Crowe’s, I do have 33% soft, fibrous plaque, which is reversible. So I put my faith in both Dr. Esselstyn’s 10% low-fat whole-food plant-based (WFPB) diet with no oils, nuts, coconuts, or avocados. But I am doubling down on HIIT based on the evidence and have added a few walnuts per day, with Dr. Esselstyn's cautionary advice not to eat too many nuts, as they can impede endothelial cells in the arterial walls.
As you may know, I had bilateral plaque in the carotid arteries, now all gone. It seems almost miraculous, so I am studying the studies to understand the mechanism of how and what happened for such a remarkable result. I have reviewed the major carotid artery studies on exercise.
Do the Carotid Studies Show Reversal?
“Read not to contradict and confute, nor to believe and take for granted, but to weigh and consider."
Francis Bacon
The carotid is the artery that runs up the side of your neck and supplies your brain with blood. It is also where stroke begins. When carotid plaque ruptures, a clot forms, breaks loose, and travels into the cerebral circulation. Carotid plaque starts forming in your 30s, so much younger than your coronary plaque, which starts in childhood.
The carotid is not just a proxy for the rest of the arterial tree. It is the artery that decides whether you can walk or lift your right arm.
It is also the easiest artery in the body to image. 20 minutes of ultrasound—no contrast, no radiation, repeatable as often as you want, and relatively inexpensive. I get mine for $140 USD.
Let’s look at a couple of the carotid trials that matter most.
1. Okada, 2022. The largest meta-analysis we have.
Published in the Journal of Physical Activity and Health in 2022. The most comprehensive review of exercise effects on carotid wall thickness ever assembled.
Patients. 1,370 adults across 26 randomized controlled trials. 32 study groups in total. 24 of the 32 groups enrolled patients with documented disease. Mean ages ranged from the early 20s to mid-70s across studies.
Exercise. Multiple modalities across the 32 groups: aerobic, resistance, combined aerobic plus resistance, high-intensity interval, moderate-intensity continuous, and endurance training. The paper analyzed each separately.
Duration. From 2 to 12 months. Most trials ran 6 months or less.
Control. Usual care. Controls maintained their habitual activity. Sedentary controls were specifically excluded.
Results
Pooled effect of exercise on CIMT: Weighted mean difference −0.02 mm against controls (95% CI −0.03 to −0.01)
Aerobic alone: −0.02 mm (95% CI −0.04 to −0.01). The largest single-modality effect
Resistance alone: −0.01 mm (95% CI −0.02 to −0.00). Smaller, but statistically significant
Duration > 6 months: Reduction of 0.02 mm with no heterogeneity (I² = 0). The effect was clean and consistent
Baseline CIMT < 0.7 mm: No effect (95% CI −0.03 to 0.00). Healthy walls did not change
Baseline CIMT ≥ 0.7 mm: −0.03 mm. The effect was concentrated in patients with measurable disease
Bottom line: Exercise reduces carotid wall thickness in adults, even though minimally. Aerobic exercise produces the largest effect. The effect is concentrated in people who already have disease, and trials longer than 6 months produce the cleanest signal.
20 micrometres across 26 trials is a real effect, but a modest one. It is the average of every kind of exercise at every dose at every duration. My own carotid moved 700 micrometers in 90 days. 35 times the pooled effect. That gap is the question this whole series exists to answer.
2. Ghardashi-Afousi, 2020. The fastest published carotid regression on exercise alone.
Published online in November 2019 in the Journal of Diabetes and its Complications, with 2020 final citation. The reason this study matters is its speed: 12 weeks. The closest analog on timeline to my own three-month result.
Patients. 74 sedentary patients with type 2 diabetes were recruited from the Diabetes Clinic at Shariati Hospital in Tehran—mean age 55. Inclusion required fasting blood glucose above 7 mmol/L and HbA1c above 7%. Randomized 1:1 to HIIT or control.
Exercise. High-intensity interval training on a stationary bike. 6 intervals, 4 minutes each, at 85% to 90% of maximum heart rate. 3 minutes of active recovery between intervals at 45% to 50% of maximum heart rate. 3 supervised sessions per week.
Duration: 12 weeks of training, with carotid ultrasound at baseline and follow-up.
Control. Continued usual diabetic care, no exercise prescription, no significant change in CIMT or other vascular measures at 12 weeks.
Results
CIMT in the HIIT group: Decreased from 0.83 mm to 0.71 mm. A 14% absolute reduction in 12 weeks (p < 0.001)
CIMT in controls: Unchanged. 0.84 mm at baseline, 0.85 mm at follow-up
Wnt pathway markers: Serum Dkk-1 and sclerostin both fell significantly in the HIIT arm. These are the molecular inhibitors of Wnt signalling that drive vascular calcification. They went down because the calcification signal went down
VO2 peak: Improved significantly in the HIIT arm. No change in controls
Bottom line: 12 weeks of supervised HIIT produced a 14% absolute reduction in carotid wall thickness in diabetic patients. The mechanism mapped to the Wnt pathway, quieting and calcification suppression
This is 24 minutes of High Intensity and 18 minutes of Interval, so the total time is 42 minutes. At 3 times per week, that is 2 hours 6 minutes. I do 4x this amount. And I had 53% CIMT reduction in 12 weeks.
A short word on the Wnt pathway
This is the first time I have heard of this pathway. Like meeting a new friend! The Wnt pathway is one of the most ancient signalling systems in animal biology. It is named for the Wingless gene first identified in fruit flies and the int-1 gene in mice. Wnt is what tells a cell where it is, what tissue it should become, and when to grow. It builds your skeleton in the womb. It maintains your stem cells. And inside the wall of an adult artery, it is one of the master switches that decides whether vascular smooth muscle cells stay quiet or transform into bone-like cells that lay down calcium.
Wnt signalling works by ligand and receptor, like a hand in glove catching a ball. A Wnt protein binds a Frizzled receptor on the cell surface, partnered with an LRP5 or LRP6 co-receptor. That binding stabilizes a protein called beta-catenin inside the cell. Beta-catenin moves to the nucleus and switches on the genes that drive osteogenic transformation. In the artery wall, those genes turn ordinary smooth muscle cells into calcium-depositing cells. That is the molecular beginning of the calcification you see on a CT scan as a CAC score.
The body has built-in brakes on this pathway. They are called Wnt inhibitors. The two most studied in vascular disease are Dkk-1 (Dickkopf-1) and sclerostin. They are circulating proteins that bind to LRP5 and LRP6 and physically block the Wnt signal from getting through. They keep tissues from over-calcifying.
Here is the counterintuitive part. In healthy biology, more Dkk-1 and sclerostin should mean less calcification. In atherosclerotic disease, the relationship inverts. Diseased arteries chronically express more Dkk-1 and sclerostin precisely because the calcification process is already running and the body is trying, ineffectively, to hold it back. Elevated levels of these inhibitors in the blood are a marker that the disease is active. The brakes are on, but the wheels are still turning.
Ghardashi-Afousi found that 12 weeks of HIIT lowered both Dkk-1 and sclerostin in the blood. That sounds like the brakes coming off. It is actually the opposite. When the calcification signal upstream of Dkk-1 quiets down, the body no longer needs to crank up the brakes. Inhibitor levels fall because the disease they were inhibiting is fading. The same drop in Dkk-1 and sclerostin that would be alarming in a healthy person is, in a diabetic with subclinical atherosclerosis, a signal that the artery is beginning to heal.
HIIT drives this through two mechanisms.
First, the mechanical signal. High-velocity blood flow during interval work shears against the endothelium and tells it to upregulate endothelial nitric oxide synthase. Nitric oxide is one of the master suppressors of vascular smooth muscle cell osteogenic transformation. More nitric oxide means less Wnt activation upstream.
Second, the metabolic signal. HIIT lowers insulin resistance and circulating glucose, which lowers AGEs (advanced glycation end products), which are themselves potent activators of Wnt signaling in vascular tissue. Quieter glucose, quieter Wnt, quieter calcification.
This trial tells me 3-month carotid regression is biologically plausible at the right dose. 14% in 12 weeks. My result was 53% in 12 weeks. Roughly 4 times larger. The mechanism Ghardashi-Afousi identified, Wnt pathway suppression through HIIT-driven shear stress and nitric oxide upregulation, is one of the levers I was running. It was not the only one. I am running 5 levers at once.
How Does Exercise Compare to Statins?
“Statins halt progression of carotid wall thickness. Exercise at the right dose reverses it and combined with the powerful effects of the CAST diet, reverses it synergistically.”
Kevin Ham, MD
If you are reading this with a CAC score and a prescription for a statin, the question you actually want answered is whether exercise comes anywhere near what a drug can do.
The honest answer is that it depends on which drug, in which patient, at which dose. Here is the cleanest comparison the literature offers.
1. Rosuvastatin alone (METEOR, 2007)
Trial: 984 low-risk subjects with mild carotid wall thickening. Randomized to rosuvastatin 40 mg or placebo for 2 years
LDL change on rosuvastatin: Mean baseline 155 mg/dL fell to 78 mg/dL. A 49% reduction
CIMT in rosuvastatin arm: −0.0014 mm/year. Essentially zero. The statin halted progression
CIMT in placebo arm: +0.0131 mm/year. The disease moved forward
Translation: A high-dose statin held the line. It did not regress the wall
2. Statin plus PCSK9 inhibitor (SLICE-CEA, evolocumab on top of statin)
Trial: 52 Asymptomatic high-risk patients, evolocumab 420 mg monthly added to maximally tolerated statin, 12 months
LDL change: 93 mg/dl to 31 mg/dL on combined therapy
Vessel wall volume: No significant difference vs usual care. Lipid-rich necrotic core of plaque significantly reduced
Cost: Approximately $6,000 per year in addition to the statin
Translation: Drugs can produce stabilization of the dangerous character of plaque but not reverse plaque.
3. High-intensity exercise alone (Ghardashi-Afousi, 2020)
Trial: 74 sedentary diabetics, 12 weeks of HIIT, no medication change
LDL change on exercise: Modest. The Pattyn meta-analysis pegs exercise alone at −7.2 mg/dL on average
CIMT change: 0.83 mm to 0.71 mm. A 14% absolute reduction in 12 weeks
Cost: Free
Translation: Exercise at HIIT intensity produced absolute regression that a 2-year course of high-dose rosuvastatin did not produce
This is the headline that should make every cardiologist who reads it jump for joy and become an evangelist for HIIT. High-intensity exercise produces carotid regression at a magnitude that high-dose rosuvastatin alone could not match in 2 years. With a fraction of the LDL movement. Through a different mechanism. PCSK9 inhibitors stacked on a statin can produce arrest of plaque but not meaningful regression, at significant cost. The biology of regression is real and is accessible by multiple paths. Exercise at the right dose is one of them.
What Does Exercise Do to the Blood?
“Exercise is a prescription that enhances the right diet but if your diet is toxic, then exercise accelerates its toxic effects.”
Kevin Ham, MD
If exercise reverses carotid plaque, exercise must be doing something to the blood that affects the plaque. Something measurable. Something a cardiologist could, in principle, find on a lab draw. So I went to the lipid literature, looking for the part of the lipid panel that exercise moves the most. What I found was not what I expected.
A 2024 meta-analysis in Sports Medicine by Pattyn and colleagues pooled 148 randomized controlled trials of exercise interventions on blood lipids. The averages, expressed as the difference exercise alone produces against a non-exercising control on the same baseline diet:
• LDL: −7.2 mg/dL
• Triglycerides: −8.0 mg/dL
• HDL: +2.1 mg/dL
That is the honest magnitude of exercise on the lipid panel. Disappointing. It is not biologically meaningless, especially compounded across decades. But it is small compared with what a statin does. Smaller still compared with what the Esselstyn diet does. Exercise will not move an LDL of 168 to 61. No trial has ever shown that it can. My LDL came down on the diet, not on the bike.
Which leaves a problem. If exercise barely moves the lipid panel, and if the lipid panel is supposedly the upstream driver of plaque, how does exercise reverse plaque at all?
Exercise does not move plaque through the lipid panel. It moves plaque through something the lipid panel does not see.
The Measurement That Actually Matters to Plaque Reversal
“HDL number tells you how much cholesterol is in the blood. Efflux capacity tells you how well it is working. The number on your lipid panel is a passenger count. Efflux is the exhaust engine.”
Kevin Ham, MD
There is a process inside your arteries that you have probably never heard of. It is called reverse cholesterol transport. It is your system for taking cholesterol out of the wall of an artery and sending it to the liver to be excreted in bile. The scientific term for this is Efflux Capacity. It is the disease running in reverse. It is regression, expressed as biology.
Picture a single foam cell, deep in the wall of your carotid artery. A macrophage that swallowed too much oxidized LDL 20 years ago and has been sitting there ever since, swollen, slow, dying by inches. On the surface of that cell are pumps. Two of them, named ABCA1 and ABCG1. Their job is to push cholesterol out of the cell, across the cell membrane, onto a passing HDL particle in the bloodstream. The HDL particle, now loaded, drifts away with its cargo and delivers it to the liver.
Exercise upregulates ABCA1 and ABCG1. More pumps. More efflux. More plaque leaving the wall. The lipid panel does not measure pumps. The lipid panel counts particles. 3 studies in the last 20 years have measured what exercise actually does to the efflux engine itself, and they tell a single, escalating story.
1. Olchawa, 2004. Athletes have more fuel pumps.
Published in Arteriosclerosis, Thrombosis, and Vascular Biology in 2004.
Design. Cross-sectional comparison of 18 endurance athletes (cyclists and runners) versus 18 age and sex-matched sedentary controls. Mean age 32. All non-smokers, all on no medications, all with normal lipid panels.
What was measured. HDL particle subspecies (pre-beta-1, alpha-1, alpha-2 by 2D gel electrophoresis), LCAT activity, CETP activity, and macrophage cholesterol efflux capacity using J774 cell assay.
Results
Pre-beta-1 HDL: +46% in athletes (p < 0.001). This is the HDL subspecies that actually picks up cholesterol from ABCA1
LCAT activity: +23% in athletes. The enzyme that locks cholesterol onto HDL so it cannot fall back off
Cholesterol efflux capacity: Significantly higher in athletes from macrophages loaded in vitro
Total HDL: Higher, but only by about 15%. Far less than the functional measurements
The athletes did not just have more HDL. They had HDL that worked. The same number on a lab report can mean two completely different things in the body, depending on whether the engine is running.
2. Sarzynski, 2022. The engine builds in 12 weeks.
Published in the Journal of the American Heart Association in 2022.
Patients. 61 healthy young men, mean age 24, randomized to 12 weeks of moderate intensity exercise or sedentary control.
Exercise. Treadmill running, 4 to 5 sessions per week, 30 to 45 minutes per session, at 65% to 80% of VO2 max. Heart rate is monitored at every session.
Control. Maintained a sedentary lifestyle. No change in efflux capacity or HDL composition at 12 weeks.
Results
Total cholesterol efflux capacity: +10.6% (p < 0.05)
ABCA1-mediated efflux capacity: +13.5% (p < 0.01). The engine specifically
Total HDL concentration: Barely changed. The number on the lipid panel did not move
HDL particle profile: Shifted toward smaller, denser particles, the more functionally active subspecies
The implication is one most cardiologists have not internalized. You can be working hard on exercise, watching your lipid panel and seeing nothing move, and meanwhile the efflux engine inside the panel is becoming dramatically more powerful. The lab report cannot see what you are building.
3. Rohatgi, 2014. The efflux engine predicts whether you live or die.
Published in the New England Journal of Medicine in 2014. The most cited paper in the cholesterol efflux capacity literature.
Patients. 2,924 adults from the Dallas Heart Study, a population-based cohort of Dallas County residents. Mean age 42, 51% women, multi-ethnic. None had known cardiovascular disease at baseline.
What was measured. Cholesterol efflux capacity at baseline using a validated cell-based assay, alongside the standard lipid panel.
Follow up. Median 9.4 years. The primary endpoint was incident cardiovascular events: myocardial infarction, stroke, coronary revascularization, and cardiovascular death.
Results
Highest quartile vs lowest quartile of efflux capacity: 67% reduction in cardiovascular events (HR 0.33, 95% CI 0.19 to 0.55)
Independent of HDL concentration: Yes. The relationship persisted after adjustment for HDL-C
Independent of LDL: Yes
Independent of all traditional risk factors: Yes. After adjustment for age, sex, race, smoking, diabetes, hypertension, LDL, HDL, and family history
Two-thirds fewer heart attacks and strokes, predicted by a measurement your cardiologist almost certainly has not run, cholesterol efflux that exercise raises by more than 10% in 12 weeks, which the standard lipid panel cannot see.
I believe this is where an important component of my 3-month carotid result came from. The lipid panel moved through diet but the HIIT efflux engine moved cholesterol efflux enormously. I cannot prove it, because nobody is running serial efflux capacity assays on me, but the biology fits the result, and the trial data fits the biology.
A Question You Should Ask Yourself
For yourself. For someone you love. Answer them in the quietness of your day.
If the most aggressive drugs for lowering cholesterol cannot reverse your plaque, what will?
Taking a pill will slow down the progression, but not reverse it. Even though my friend Rob was on a statin since age 34 (LDL ~80-90), he still died of a sudden heart attack at 58 years. He had no other risk factors or symptoms.
For Someone You Love
There is someone in your life building plaque. Most are. You thought of them. Send this to them. Your loved ones just need the information to act and a guide to help them.
Keep going. The race is long, the road is beautiful, and the body was built to heal.
Grace, strength and love to you.
MORE READINGS YOU’LL ENJOY
Health
Watch: The 2 Foods That Reverse Heart Plaque (Half a Million Views)
Reversing My 77% Heart Plaques
Stats Say You Likely Have Heart Plaque
The Healing Power of Food: Nitric Oxide
Meaning
I pray you unlock your heart to reach the height of your full potential by discovering your calling.
Kevin Ham, MD
Appendix
The summary of the referred exercise studies:
1. Okada Y, et al. Effect of exercise on carotid artery intima media thickness in adults: a systematic review and meta analysis. J Phys Act Health. 2022;19:855 to 867.
26 randomized trials, 1,370 participants. Pooled weighted mean difference of −0.02 mm. Aerobic produced the largest effect. Subgroup analysis showed effect doubled in trials lasting more than 6 months in patients with disease at baseline.
2. Ghardashi-Afousi A, et al. Improved carotid intima media thickness induced by high intensity interval training associated with decreased serum Dkk 1 and sclerostin in type 2 diabetes. J Diabetes Complications. 2020;34(1):107469.
74 sedentary diabetics, 12 weeks of HIIT (6 intervals of 4 minutes at 85% to 90% maximum heart rate, 3 sessions per week). CIMT fell 14% absolute. Wnt pathway markers Dkk-1 and sclerostin both fell. The fastest published carotid regression on exercise alone.
3. Crouse JR, et al. Effect of rosuvastatin on progression of carotid intima media thickness in low risk individuals with subclinical atherosclerosis: the METEOR trial. JAMA. 2007;297:1344 to 1353.
984 low-risk subjects, 2 years of rosuvastatin 40 mg vs placebo. LDL fell 49% (155 to 78 mg/dL). CIMT essentially flat at −0.0014 mm/year on statin vs +0.0131 mm/year on placebo. Statin halted progression but did not produce regression.
4. Pattyn N, et al. The effect of exercise training on blood lipids: a systematic review and meta analysis. Sports Med. 2024;54:1 to 28.
148 RCTs. Exercise alone effects on lipids: LDL −7.2 mg/dL, TG −8.0 mg/dL, HDL +2.1 mg/dL. The honest baseline magnitude of exercise on the standard lipid panel.
5. Olchawa B, et al. Physical fitness and reverse cholesterol transport. Arterioscler Thromb Vasc Biol. 2004;24:1087 to 1091.
18 endurance athletes vs 18 sedentary controls. Athletes had +46% pre-beta-1 HDL, +23% LCAT activity, and significantly higher macrophage cholesterol efflux capacity. The functional HDL measurements were 2 to 3 times more elevated than the simple HDL concentration.
6. Sarzynski MA, et al. Moderate and high intensity exercise improves lipoprotein profile and cholesterol efflux capacity in healthy young men. J Am Heart Assoc. 2022;11:e023386.
61 young men, 12 weeks of moderate intensity treadmill running 4 to 5 days per week. ABCA1-mediated efflux capacity rose 13.5%. Total HDL barely changed. Function moved before concentration did.
7. Rohatgi A, et al. HDL cholesterol efflux capacity and incident cardiovascular events. N Engl J Med. 2014;371:2383 to 2393.
Dallas Heart Study, 2,924 adults, median 9.4 year follow up. Highest quartile of efflux capacity had 67% fewer cardiovascular events than lowest quartile. Independent of HDL concentration, LDL, and every traditional risk factor.
Subscribe to my Compounding Wisdom newsletter and start transforming your life. ham.com
Subscribe to my YouTube channel @DrKevinHamfor videos on how I reversed my clogged arteries in 3 months, the top foods that clear your arteries, and the first principles of health that can save your life. Like, share and subscribe — it could save the life of someone you love.
Does Exercise Reverse Plaque?
Is there a threshold?
Is there a threshold?
Dr. Kevin Ham, MD
“And let us run with perseverance the race marked out for us, fixing our eyes on Jesus, the author and perfecter of faith.”
Hebrews 12:1-2
I just launched a video of why you should start drinking 50 ml of pomegranate juice each day. I know we hear a lot of things, but I repeat so more people are reminded and my hope is they move to action. If I could stop one heart from aching…
Let me know in the comments of this video if you are drinking pomegranate or not and make sure you subscribe so that you are notified of each video in my channel. https://www.youtube.com/@DrKevinHam
Also watch my Thursday video. It will show you why half the people who are seemingly healthy can have a sudden heart attack. If you are over 50, there is a 91% chance you have plaque in your heart arteries. Also let me know in the comments here whether you knew this or not and if you will get a Calcium CT Heart scan. I’m curious. I’ve had medical doctors ask me for personal consults, which is humbling and my heart goes out to everyone who wants to reverse their diseases.
I am flying to San Francisco today to ride in the Levi Gran Fondo. I’m going to ride a true century mile ride (160 km) with 14,000 ft of elevation (3000 m). I’m excited to meet up with my good friend Michael Woods, who just retired from pro cycling and who can also run a 4 minute mile. He wishes to be the world’s fittest man and is running Ironmans, skiing, biking, running and swimming.
After thinking how I reversed my carotid plaque from May 9, 2025 (Started WFPB Esselstyn diet) to August 19, 2025, when my carotid ultrasound showed that all my plaque was gone and CIMT reduced 53%, I have been trying to understand the mechanism and biochemical pathways this occurred. I have been so focused on diet, that I wondered how much my 3000 km of cycling played a role. I did three Gran Fondo (120+ km) rides last year. Then after my September fondo, I basically stopped riding. My coronary plaque did not really reverse after that, although blood flow improved remarkably. So that has made me curious.
My thought is that high intensity riding accelerated my plaque reversal. So this year I am doubling down and riding four Gran Fondos and running a half marathon. I don’t like running at all but since I am turning 56 years old, I want my bones to be strong and need some impact exercises besides cycling. I also plan to start strength training after my Sept fondo this year and build more muscle so I can retain it as I age. Then I will focus on fasting and less intense exercises for fall and winter months. This is a natural seasonal pattern imho.
So I did a deep dive on exercise studies and plaque. It was so much research that I have to divide it into four parts. Here is the first part looking at the various trials to answer my first question: Is there a threshold intensity and amount of exercise that reverses plaque independently? After this I plan to do a deep dive on fasting and then on multi-modal strategies to reduce plaque, like I am doing:
Dietary x HIIT exercise x Fasting. I call it my Trinity Reversal Flywheel Synergy.
Why High Intensity Interval Exercise?
“Can exercise reverse atherosclerosis?”
Kevin Ham, MD
I have been cycling since 2008 and more seriously since 2014. I can ride with the best and have ridden with my pro team during their rest days on the Tour de France. Riding between Michael Woods and Chris Froome, also a good friend and winner of the Tour de France four times, I felt like I was in the best shape of my life.
Yet I found out that I have severe atherosclerosis. If intense exercise reversed plaque, then shouldn’t my arteries have been healing while I cycled? Why were they so clogged? 77%, 55%, 45% etc.
I even thought initially that because of my intense cycling, maybe it caused my plaque. But I’ve determined that the cause is mostly dietary. When I changed my diet, my plaque reversed. This is what Dr. Esselstyn revealed through his patients, who were ‘end-stage’ heart disease, barely able to walk without getting chest pain or short of breath. But before my dietary changes, I was riding up the Alp mountains in France, Italy and Switzerland. 100,000 m of riding my bike up mountains a year for years! That’s pretty high intensity.
But when my biochemistry became optimal by a complete focused diet that eliminated all added oils and dietary cholesterol, I believe exercise accelerated Reverse Cholesterol Transport (read this article I wrote) in my plaques.
I continually think from first principles and then study how the biochemical pathways work in the body. My degree in Biochemistry and Medicine is delighted to learn with great curiosity and interest and translate this complex biochemical language into something you can relate to so you can be empowered to restore your own health and those around you.
Does studying medicine for four years allow you to heal disease?
Four years of medical school made me a doctor, but if you studied your disease and educated yourself, I believe within a month, you would have enough wisdom and knowledge to start healing yourself. I am spending my spare moments for this very reason. To empower you with health wisdom to reverse disease. We were not taught this in medicine. We were taught to diagnose and manage and sometimes treat disease. Many diseases we do not know or ponder the true cause. Let’s look at some exercise studies to see what’s better: exercise or diet?
What is HIIT?
“I think of my high intensity exercise as a prescriptive pressure wash of my arteries to activate eNOS and nitric oxide, medicine for my blood vessels and to mobilize my HDL to be more functional and activate Reverse Cholesterol Transport, which is one of the greatest health secrets.”
Kevin Ham, MD
Just a note here to describe what HIIT is. It is high intensity, when you exercise at a high intensity such that you cannot speak, huffing and puffing, when your heart rate is more than 80% of your maximum heart rate. A simple measure of your max hr would be 220- your age. So if you are 50 years old, your max hr = 220-50 = 170. I’m 56, but my max hr which should be 220-56=164, is actually 195 beats per min (bpm). So I try to 195*80%=156 bpm. I used to average this hr for 4 hours on my Gran Fondos. Average! After I found out I have blocked arteries, I try to limit my heart rate to 160 bpm and hover between 130-150 bpm, which is what we call zone 2 or tempo training.
So that is the HI in high intensity. Then you must consider the second ‘I” which is Interval. So you have to pace or decide for how long you do this high intensity. There are studies that do 4x4 which is 4 minutes of high intensity repeated four times. In between the repetitions (reps) of high intensity, there is an interval of rest. You need to recover before the next round of HI effort. You’ll know when you are ready when you can breathe comfortably and speak easily. At 150 bpm, I can go 4-6 hours with HIIT. At 130 bpm, I could go even longer. Pretty extreme. So all the HIIT studies are very easy for me as I like to ride 2-4 hours to clear my mind, exercise my eyes. It’s my meditation and hobby.
Top Exercise Studies
“How can we thank all these scientists who pursue their curiosity and passion to discover life’s secrets. I feel so blessed for each scientist. Thank you from the depths of my heart!”
Kevin Ham, MD
1. Vesterbekkmo, 2023.
The first randomized trial of coronary plaque regression from exercise alone.
Published in the European Journal of Preventive Cardiology in 2023, the CENIT trial randomized sixty patients who had recently undergone PCI to either six months of high intensity interval training or usual care. Serial intravascular ultrasound at baseline and six months to measure plaque. The HIIT (high intensity interval training) group showed a between group difference in normalized total atheroma volume of twelve cubic millimeters against controls. Slight regression like cholesterol lowering drugs.
This study was the first randomized trial to show that exercise alone, without additional dietary or pharmacological change, can regress coronary atheroma in humans.
The effect was small in absolute terms. It was also statistically robust, mechanistically coherent, and the first crack in the dogma that only drugs regress plaque.
2. Hambrecht, 1993.
The 2,200 kilocalorie threshold.
Published in the Journal of the American College of Cardiology in 1993 by Rainer Hambrecht and the Heidelberg group, this is the dose response study that quietly defined the exercise prescription for reversal for the next thirty years. Sixty two patients with coronary artery disease were tracked for a year with repeat angiography. The patients were stratified by weekly leisure time physical activity expressed in kilocalories expended.
Below 1500 kilocalories (kcal) a week, lesions progressed.
Above 2200 kcal a week, lesions regressed.
There was a clean dose response, and a clean threshold. 2200 kcal a week translates to about five to six hours of moderate aerobic exercise.Three times what the current American Heart Association baseline recommends. Twice what the average American cardiac rehab program prescribes.
My cycling volume runs at ~8000 kcal a week during the season. More than three times Hambrecht's regression threshold. No wonder I cannot find anyone who has matched the degree and speed of my carotid reversal. I’m an extreme outlier.
But this shows the world what is possible, just like a World Record does. Just like once the 4 minute mile was run by Roger Bannister, runners believed it was possible. I long for many people to break my reversal record for carotid plaques and CIMT of 53% reduction in just three months. I will show by first principles why such reversal is possible, much like a fractured bone healing in just 3 months. This is the basis of my CAST protocol. This is the miraculous healing power within us and in nature and in foods and blood.
3. Ornish, 1990 and 1998.
The Lifestyle Heart Trial.
Published in The Lancet in 1990 with five year follow up in JAMA in 1998, Dean Ornish’s Lifestyle Heart Trial is the most cited reversal experiment in the literature. Forty eight patients with angiographically proven coronary disease, randomized to either a comprehensive lifestyle program or usual care. The lifestyle arm got a ten percent fat vegetarian diet, moderate aerobic exercise, stress management, and group support. Quantitative angiography at baseline, one year, and five years.
At one year, the experimental group showed an average stenosis regression, with eighty two percent of patients improving. The control group on usual care showed progression. By five years, the experimental arm had deepened its regression, and the control arm had accumulated two and a half times the cardiac events.
Two things to notice. First, the exercise component was only three hours per week, and the diet did most of the work. Second, the angiographic changes were small in absolute terms. Mean stenosis fell from roughly forty percent to thirty seven percent at one year.
Meaningful, but modest.
4. Schuler and Niebauer, 1992 and 1997.
The Heidelberg secondary prevention trial.
Published in Circulation in 1992, with six year follow up in 1997, this trial randomized 113 men with stable angina to either a one year intensive low fat diet and exercise program or usual care. Serial angiography at baseline and one and six years.
At one year, 32% of the intervention group showed regression compared with 17% of controls. Progression was 45% versus 48%.
Six years later, the numbers held. Three times the maintenance dose, lower regression rates, but the disease stayed arrested.
The early work suggested that the induction dose of exercise is higher than the maintenance dose, a finding that matches what every endurance athlete in their sixties has figured out empirically.
5. Madssen, 2014.
Twelve weeks to the necrotic core.
Published in the American Journal of Cardiology in 2014, this twelve week trial in 36 post PCI patients used grayscale and radiofrequency intravascular ultrasound to measure plaque composition before and after a short course of aerobic exercise training.
The finding that matters: plaque burden fell by 10.7 percent in treated lesions, and necrotic core volume fell by roughly three percent.
Twelve weeks. That is the shortest regression signal anywhere in the coronary literature. It is the answer to the question every patient asks when they begin. How long until something changes? Three months of real work.
Five coronary trials. Different populations. Different protocols. Different imaging modalities. All pointing at the same finding. Exercise regresses coronary plaque when the dose crosses a threshold that looks something like 2000 kcal a week, sustained over three to twelve months.
What the Trials Say
Exercise reverses plaque. The regression threshold is roughly 2200 kcal per week, which translates to five to six hours of moderate aerobic activity. The modality that matters most is aerobic. The effect is concentrated in people who already have disease. The effect shows up in as little as twelve weeks on imaging.
If that is all you take from this week, it is enough. If you are a man between forty and sixty five with a new CAC score, and a cardiologist who told you to take a statin and walk more, here is what the literature now shows beyond reasonable dispute. The walking is not wrong. The dose is insufficient to reverse plaque. Three hours a week of leisure exercise sits below the regression threshold. Six hours of real aerobic work crosses it.
But that is the trial literature.
I have some ideas for those of you who may find this intensity of exercise difficult.
Focus on reducing your inflammation, oxidation, glycation and LDL lower and exercise will work on helping phase 1 of Reverse Cholesterol Transport via HDL efflux capacity, which means to transport cholesterol out of the plaque.
Even the best statins and PCSK9 cholesterol lowering drugs only reverse plaque by 1%, which is essentially arrest rather than reversal. Even with PCSK9 + statins reducing LDL to 34 mg/dL, reversal does not seem to increase. This means you just need to lower LDL below a certain threshold, which I will cover in Part 3 of this Exercise series.
My own reversal result sits in a place the trial literature does not describe.
“The educated soul can be healthy through its lifestyle, set by its heart and its mind. Heartset and Mindset.”
Kevin Ham, MD
Next week, Part 2: How Much Can Exercise Reduce Plaque?
On Exercise Reversing Plaque.
Arterial plaque reversal can be easier to see, what we call a lead indicator in the carotid neck arteries. That’s what was revealed in my 3 month carotid arterial plaque reversal.
The five published exercise case studies that come closest to mine but none of them come close to my reversal. Why?
My Trinity Reversal Flywheel is running every lever I can find at the same time and explains why three months is not miraculous.
Your Questions
“The educated soul can be healthy through its lifestyle, set by its heart and its mind. Heartset and Mindset.”
Kevin Ham, MD
Questions worth sitting with
1. How many hours a week do you move hard enough that talking hurts?
If the honest answer is under five, you are below the floor where your exercise reverses your plaque meaningfully. Work up towards this as you change your biochemistry.
2. Can you move, hard, for 5 minutes today and repeat each day?
The first 5 minutes are the only 5 minutes that feel impossible. The biology responds to what you do, not what you know.
For Someone You Love
There is someone in your life running their nine steps poorly right now. You thought of them. Send this to them. Your loved ones just need the information to act and a guide to help them.
Keep going. The race is long, the road is beautiful, and the body was built to heal.
Grace, strength and love to you.
MORE READINGS YOU’LL ENJOY
Health
Watch: The 2 Foods That Reverse Heart Plaque (Half a Million Views)
Reversing My 77% Heart Plaques
Stats Say You Likely Have Heart Plaque
The Healing Power of Food: Nitric Oxide
Meaning
I pray you unlock your heart to reach the height of your full potential by discovering your calling.
Kevin Ham, MD
Subscribe to my Compounding Wisdom newsletter and start transforming your life. ham.com
Subscribe to my YouTube channel @DrKevinHam for videos on how I reversed my clogged arteries in 3 months, the top foods that clear your arteries, and the first principles of health that can save your life. Like, share and subscribe — it could save the life of someone you love.
Reverse Cholesterol Transport
Through Diet, Movement and Fasting
Through Diet, Movement and Fasting
Dr. Kevin Ham, MD
Endothelium is the Life of Blood
“The highway of life is from the heart into the blood into the liver.”
Kevin Ham, MD
I’m attending the last TED conference in Vancouver this week, and it is so inspirational. I wanted to meet Reed Hastings, the Founder of Netflix. Made my day when I saw him. I was standing to his right as a lady spoke to him on his left. He turned to me and smiled, stuck out his hand, and kindly embraced my right hand. He said, “Hi Kevin,” with a sweet smile and tender voice. He is such a kind gentleman, and I will never forget his attention, his smile and humility. He felt like a kindred spirit. No wonder Netflix has flourished under his guidance.
Then I was blown away by Mark Rober, a YouTube superstar with 75 million subscribers. He had a dream of making a $60 million educational program to provide to teachers for free. As he showed how he taught science to kids through experiments, making things fun, and hiding lessons in play, I wondered how I could do this for health education?
And Ann Patchett, who inspires everyone to be a reader of books. Wow, her TED talk melted my heart. In that moment, all the plaques of my coronaries were laid low like valleys in humble adoration to her heart for all people to read.
And of Amy Cuddy. I had a class with her while at Harvard Business School 18 years ago. I knew of her rise as one of the most-viewed TED Talks, thanks to her power pose. But I did not know how much professional bullying she had experienced due to it. I was in tears for most of her talk. I was so glad to give her a warm, empathetic embrace. I pray and wish to help her. I know she will rise again, like a caterpillar emerging from a cocoon.
I can go on about the endless emotions and wonder as I listened to Susan Burton provide homes for women who leave the prisons with no place to call home. Or Gabriella Dieguez, who has resurrected the lost voice of buried women composers. Or Gabriela Moynihan, who donated her left kidney at age 21. Or Azusa Murakami, who spends a year producing bubbles to show the beauty of life through the ethereal and temporal nature of our being and moments of life. I dream of organizing a conference like this, just for health, by wisdom that heals the body, soul, and spirit. It is a quiet seed planted in the vessels of my heart in the mountains of plaque, that faith shall remove and place them into the sea of blood that is impeded by the voluminous heights that oppose life, my own doing of decades of not living right, not eating right, as body, soul and spirit urge. I have heeded the warning signs and will live each moment in gratefulness and humble myself under the hand of God and people to do that which is planted in my heart.
May you be blessed by the hearts of others who yearn to make you and themselves whole and united, in peace and harmony, though the outer being be afflicted and the inner being assaulted.
I wish I could just start and be of heart and inspire and teach as they have at TED in my YouTube videos (youtube.com/@drkevinham) and in this newsletter, but I currently lack the full wisdom and creativity, not to mention the time. I have had so many people send their thanks and encouragement to keep providing valuable information as I learn and live it. To strive for excellence, yet have compassion and empathy as we journey together on our heart journey to heal together as best we can.
I will continue to pour my heart into figuring things out for myself and accomplish the proverb, “Physician, heal thyself!” so I can do so for you and everyone who suffers from these chronic, deadly diseases.
As you know, I reversed my carotid arterial plaque in just three months. I thought surely someone else in the world has done this, but I have yet to find any RCT or case study, for that matter. I’m continually searching for a better, faster way to heal arteries (coronaries, carotids (done), aortic, cerebral, femoral (easy), mesenteric (easy), retinal (I think it’s done, but will have to see when I get my next eye shot, last one three years ago, but supposed to be monthly)).
But my coronary arteries have not reversed… Yet. The obstruction volume was essentially the same, but I could see the plaque remodelling in shape, and my FFR (think of it like blood flow) past my most severe obstruction has improved from 75% to 80%, which is significant.
But why had my carotid plaque reversed and not my coronary heart arteries?
That question sent me down a deep scientific rabbit hole in my spare moments over the last 7 months. I prayed and asked for wisdom. Then, I found the ancient pathway that was actually discovered over 50 years ago, a 9-step biological pathway that I had never heard of before, yet once I found it, I started to understand it was already well known, yet only by special interest groups. Why wasn’t this mainstream when heart disease is the #1 global killer?
Reverse Cholesterol Transport, RCT. The same acronym we use for randomized controlled trials.
As I was listening to Peter Steinberger at TED, the creator of Open Claw, and how he had created it by thinking “a big Holy S**t” idea. As Peter described his Open Claw moment, one also came to me just minutes later. He said he hadn’t coded a single line, but had just prompted the AI to create the first versions of Open Claw when it became a team of autonomous, self-coding AI agents. He made it open source and clawed its way into everything to solve problems.
I thought, what could be a bigger problem than our world’s biggest disease killers, causing death and suffering to so many tens of millions each year? Mimi and Dave, whom we had just met at TED, have to leave tomorrow to be with her ailing 96-year-old father. God bless you, Mimi, and your dad.
I had a vision of how to help cure our top diseases. I saw a vision of the TED stage, and in its place was a different set of talks, talks by both healers and patients of wisdom that truly heal. The body, the mind and the spirit.
RCT
“Life is taught to be driven forward, but if you wish to live fully and openly, your direction should be in reverse.”
Kevin Ham, MD
The man who first described the process of Reverse Cholesterol Transport (RCT) was John Glomset, a Norwegian-American biochemist at the University of Washington. In 1968, Glomset published the hypothesis that HDL particles were not passive markers of cardiovascular health but active cholesterol collectors, gathering cholesterol from peripheral tissues, including arterial walls and returning it to the liver for permanent disposal.
He named it Reverse Cholesterol Transport (RCT) because it runs in the direction opposite to the process that causes arterial disease. Cholesterol enters arterial walls through LDL. Glomset said it also has to come out through a specific pathway, or plaque accumulates regardless of how well you manage the inflow. He already surmised the cure for heart disease with this insight.
His colleagues largely ignored him. Glomset’s hypothesis sat dormant for nearly two decades before Alan Tall at Columbia and Daniel Rader at Penn built the modern molecular framework on his foundation. Glomset was right in 1968.
Medicine took fifty years to act on it.
Almost everyone is focused on the first step: slowing or halting arterial disease by lowering LDL cholesterol. Hardly anyone focuses on reversing cholesterol transport (RCT) out of arterial plaque. Why not? It seems so ‘bloody’ obvious to me. Hidden in plain sight. It’s like I was finally let in on one of the world’s greatest medical secrets.
Then I saw an even bigger vision.
I only had one body to experiment on, but what if patients like me were motivated to test different foods and lifestyle measures to see who could reverse plaque better and faster?
What if we did an open source model like Open Claw or Wikipedia, by the people and for the people?
Why don’t we RCT (randomize controlled trials) RCT (reverse cholesterol transport)?
ACT
“Reverse Cholesterol Transport is a 9-step pathway but its players seem like strangers from a strange land we must befriend. How can we understand this new language? It must be translated into a language and visuals we can easily understand and act upon. Then I had it, acronyms that remind us of what they do. ACT.”
Kevin Ham, MD
The nine steps are grouped into three master phases, which spell ACT. Each phase has three sub-steps. Understanding the architecture makes the nine steps memorable and actionable.
Activate (Phase I): Driven by diet, reverses cholesterol transport from the arterial wall into the bloodstream.
Carry (Phase II): Driven by exercise, it moves the cholesterol from the blood to the liver.
Take out (Phase III): Driven by fasting and fibre to take out the cholesterol through the intestines.
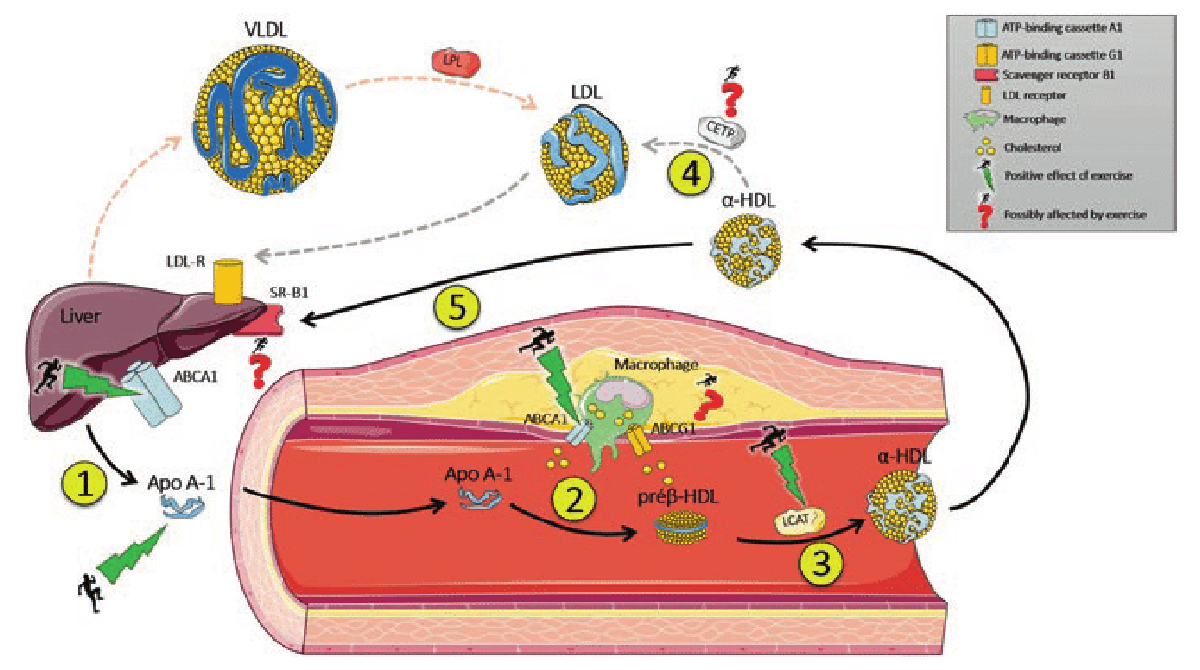
Each step has an exact science and precise levers you can pull.
This week, we will focus on Phase I: Activate, and its first three steps, which spell: AMP.
Awaken Cholesterol Efflux (Step 1)
Mobilize ApoA-I (Step 2)
Prime LCAT (Step 3)
Step 1: Awaken Cholesterol Efflux
The Emergency Exit That Nobody Knows Is Armed
“The gate is ancient. Your only job is to stop blocking it. Every plant-based meal is the key to unlocking it while every gram of saturated fat keeps it locked.”
Kevin Ham, MD
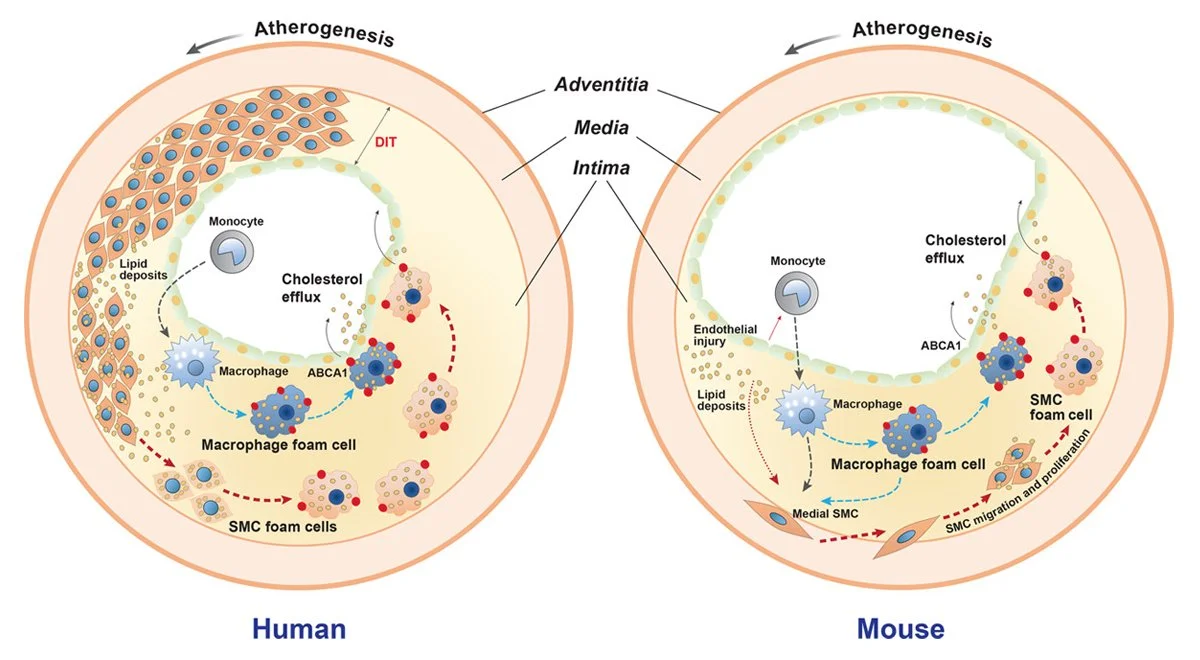
Inside every foam cell embedded in your arterial plaque is a protein called ABCA1 (a Binding Cassette A1) on its outer membrane. ABCA1 is a molecular emergency exit. When it opens, it pumps cholesterol out of the cell and onto passing HDL particles in the bloodstream. The foam cell has been reaching for a rope for years. The question is whether you are giving it one.
The lock on this exit is a nuclear receptor called LXR (liver X receptor).
Every vegetable and legume you eat contains phytosterols that bind LXR and activate it directly, a mechanism confirmed across multiple published trials.
Exercise shear stress above 80 percent of maximum heart rate triggers nitric oxide synthesis through eNOS that opens the gate from outside.
Saturated fat suppresses LXR and keeps ABCA1 shut.
This is the most critical step of the 9-step Reverse Cholesterol Transport pathway. Without it, the engine doesn’t start.
WHAT BLOCKS IT:
Saturated fat: directly suppresses LXR and prevents ABCA1 expression in macrophages
Oxidized LDL: drives continued cholesterol uptake faster than efflux can remove it
Hyperglycemia: glycates apoA-I and impairs the ABCA1 cholesterol loading interaction
WHAT ACCELERATES IT:
Plant phytosterols: LXR activation confirmed in published trials; every plant-based meal signals ABCA1 to open
High-intensity exercise above 80% max HR: shear stress activates eNOS and endothelial nitric oxide, activating ABCA1
Fasting and AMPK activation: Fasting activates AMPK, which stabilizes ABCA1 at the macrophage cell surface
Step 2: Mobilize ApoAI
“You cannot collect what you never sent to collect. Every reverse cholesterol transport system begins with the decision to dispatch the vehicle. Your liver makes that decision. Those shuttles are ApoA1. Your diet and exercise power it.”
Kevin Ham, MD
Brouillette et al., Biochim Biophys Acta 2001, Fig. 1
Your liver manufactures apolipoprotein A-I continuously and dispatches it into the bloodstream as a nearly lipid-free particle. ApoA-I is the empty truck. It carries no cargo. It circulates, seeking a foam cell with an open ABCA1 gate so it can accept a first load of cholesterol and initiate the reverse cholesterol transport cascade.
An open exit door means nothing if no truck is waiting outside. Think of apoA-I as a delivery fleet. Dispatching more trucks means more pickups completed per hour. Fewer trucks means packages pile up on the doorstep even when the door is wide open. Your liver is the fulfillment center. Your daily choices are the dispatcher.
WHAT BLOCKS IT:
Processed diet and liver dysfunction: reduces hepatic apoA-I synthesis; fewer trucks dispatched
Smoking: directly oxidizes and degrades the apoA-I protein structure in circulation
Chronic systemic inflammation: serum amyloid A displaces apoA-I on HDL particles and degrades their function
WHAT ACCELERATES IT:
Whole food plant-based diet: increases hepatic apoA-I synthesis at the source
Fasting: upregulates apoA-I production and reduces apoA-I catabolism
Regular aerobic exercise: increases the rate apoA-I cycles through arterial tissue each day
Step 3: Prime LCAT
The Garbage Compactor That Makes the Truck Useful
“Capacity is not determined by how many vehicles you have. It is determined by how much each vehicle can carry. Protect the compactor and every truck becomes a freight train.”
Kevin Ham, MD
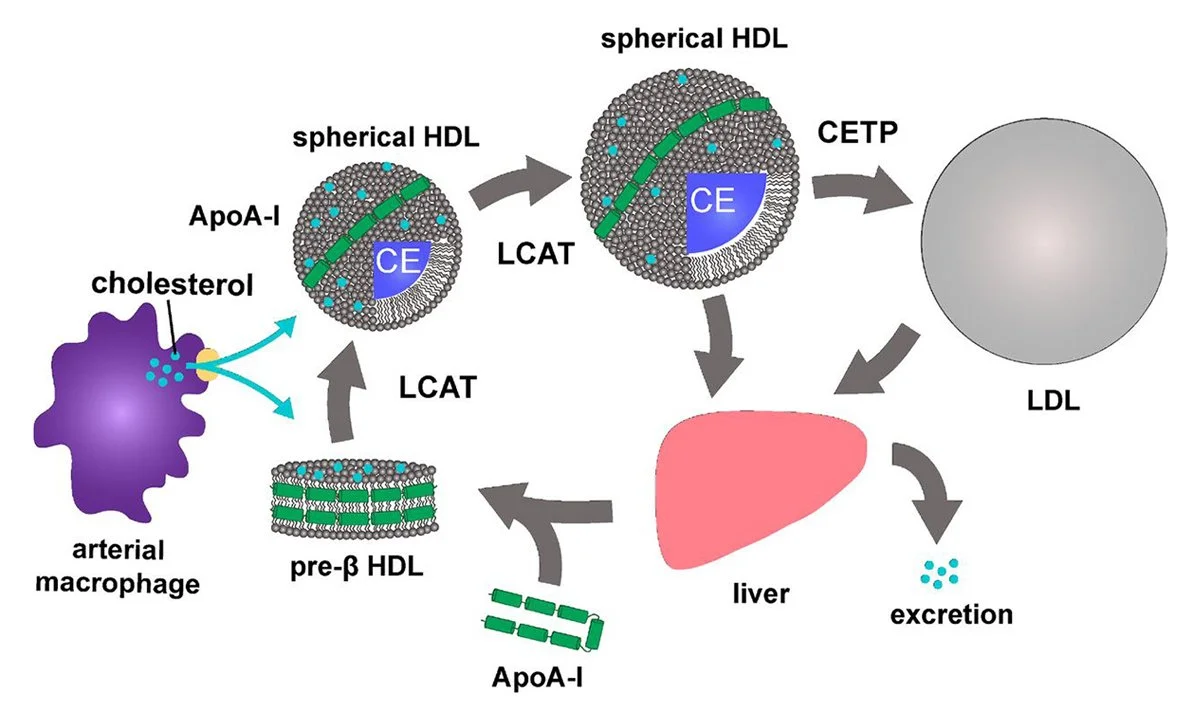
Glomset, J Lipid Res 1968, Fig. 1
The LCAT esterification reaction: free cholesterol on HDL surface is converted to cholesterol ester and moves to the hydrophobic core, expanding particle from a flat disc (nascent HDL) to HDL3 sphere to HDL2 sphere.
A nascent HDL particle is tiny and flat, like a small coin, and fills up quickly at the surface. This is where LCAT enters. Lecithin-cholesterol acyltransferase (LCAT) is an enzyme traveling on the HDL surface. It converts loose surface cholesterol into cholesterol ester and packs it into the particle core, freeing the surface for another full load. LCAT is activated by apoA-I and is the enzyme responsible for HDL maturation; this mechanism is well established in the published biochemistry literature.
Without LCAT running, the truck fills up after a few houses. With it running, the same truck covers fifty houses per run. But apoA-I must be structurally intact to activate LCAT. Oxidative stress from processed foods and chronic inflammation damage apoA-I and silence the compactor entirely, which is why HDL particles can be numerous in the blood yet functionally impaired.
WHAT BLOCKS IT:
Oxidative damage to apoA-I: from processed food, smoking, and chronic inflammation; prevents LCAT activation
Serum amyloid A: displaces apoA-I from the HDL particle surface during acute phase responses
Low HDL phospholipid content: insufficient phospholipid substrate for the LCAT transesterification reaction
WHAT ACCELERATES IT:
Pomegranate juice 50ml once or twice daily: (after meals, then walk) activates PON1 antioxidant enzyme on HDL, protecting apoA-I from oxidation; confirmed in Aviram et al. studies
Algae-derived EPA and DHA: incorporate into HDL membrane phospholipids, improving fluidity and LCAT activation efficiency
Aged garlic extract 2,000mg: reduces systemic inflammation and oxidative stress that damages apoA-I structure
Some steps are running well. Some are blocked. The question is which ones, and which levers to pull first.
Like waves of water on rock, daily compounding with many small correct decisions is what running all nine steps feels like. The direction is clear. The biology is responding. Give the cleanup crew the conditions they need to do their job of healing.
Seems complicated yet its so beautiful and simple. A well orchestrated system that heals when we give it the right lifestyle conditions to operate smoothly, like it was meant to be.
Your Questions
“The educated soul can be healthy through its lifestyle, set by its heart and its mind. Heartset and Mindset.”
Kevin Ham, MD
Questions worth sitting with
For yourself. For someone you love. Answer them in the quietness of your day.
1. Awaken: What did you eat today and did it open the ABCA1 gate or close it?
Every gram of saturated fat you consume suppresses LXR and closes the exit hatch on your foam cells. Every legume and vegetable activated it. Look at your last three meals and name one specific change to tomorrow’s first meal that arms the gate.
2. Mobilize: When will you help ApoA1?
Whole food, plant-based diet. Eat greens, move them through exercise and rest (fast) to boost their production.
3. Prime: How will you reduce oxidation today?
Compact your garbage cholesterol trucks (HDL) by activating PON1 and LCAT. Pomegranate juice. Get some at your organic health food store. Just 50 ml a day or twice a day, at the end of your meals and then walk for 15 minutes.
For Someone You Love
There is someone in your life running their nine steps poorly right now. You thought of them. Send this to them. The system is universal in human biology. The endothelium that repaired my carotid arteries responds to the same signals as the endothelium in our coronary arteries. Your loved ones just need the information to act and a guide to help them.
MORE READINGS YOU’LL ENJOY
Health
Watch: The 2 Foods That Reverse Heart Plaque (Half a Million Views)
Reversing My 77% Heart Plaques
Stats Say You Likely Have Heart Plaque
The Healing Power of Food: Nitric Oxide
Meaning
The Courage to Your Magnum Opus
APPENDIX
The published research underlying the nine-step reverse cholesterol transport framework
Reverse Cholesterol Transport: Foundational Science
Glomset JA. The plasma lecithins:cholesterol acyltransferase reaction. Journal of Lipid Research. 1968;9(2):155-167. [Foundational paper naming reverse cholesterol transport and describing the LCAT-driven HDL maturation mechanism.]
Tall AR. Plasma high density lipoproteins: metabolism and relationship to atherogenesis. Journal of Clinical Investigation. 1990;86(2):379-384.
Oram JF, Heinecke JW. ATP-binding cassette transporter A1: a cell cholesterol exporter that protects against cardiovascular disease. Physiological Reviews. 2005;85(4):1343-1372. [Comprehensive review of ABCA1 biology.]
LXR Signaling, ABCA1 and Plant Phytosterols
Tontonoz P, Mangelsdorf DJ. Liver X receptor signaling pathways in cardiovascular disease. Molecular Endocrinology. 2003;17(6):985-993. [LXR as master regulator of ABCA1 and cholesterol efflux.]
Repa JJ, Mangelsdorf DJ. The liver X receptor gene team: potential new players in atherosclerosis. Nature Medicine. 2002;8(11):1243-1248.
Cholesterol Efflux Capacity and Cardiovascular Outcomes
Khera AV, Cuchel M, de la Llera-Moya M, et al. Cholesterol efflux capacity, high-density lipoprotein function, and atherosclerosis. New England Journal of Medicine. 2011;364(2):127-135. [Key Rader group study showing CEC predicts CV events independently of HDL-C level.]
Rohatgi A, Khera A, Berry JD, et al. HDL cholesterol efflux capacity and incident cardiovascular events. New England Journal of Medicine. 2014;371(25):2383-2393. [Prospective confirmation: highest CEC quartile had 67% fewer events.]
CETP Inhibitor Trial Failures
Barter PJ, Caulfield M, Eriksson M, et al. Effects of torcetrapib in patients at high risk for coronary events. New England Journal of Medicine. 2007;357(21):2109-2122. [Torcetrapib increased mortality despite raising HDL-C.]
Schwartz GG, Olsson AG, Abt M, et al. Effects of dalcetrapib in patients with a recent acute coronary syndrome. New England Journal of Medicine. 2012;367(22):2089-2099. [Dalcetrapib: no benefit.]
Lincoff AM, Nicholls SJ, Riesmeyer JS, et al. Evacetrapib and cardiovascular outcomes in high-risk vascular disease. New England Journal of Medicine. 2017;376(20):1933-1942. [Evacetrapib: no benefit despite substantial HDL-C increase.]
Esselstyn Protocol and Plaque Regression
Esselstyn CB Jr, Gendy G, Doyle J, Golubic M, Roizen MF. A way to reverse CAD? Journal of Family Practice. 2014;63(7):356-364. [198 patients; 177 compliant had 1 event vs 62 in non-compliant group.]
Esselstyn CB Jr. Resolving the Coronary Artery Disease Epidemic Through Plant-Based Nutrition. Preventive Cardiology. 2001;4(4):171-177.
FXR, FGF19, and the Bile Acid-CYP7A1 Axis
Inagaki T, Choi M, Moschetta A, et al. Fibroblast growth factor 15 functions as an enterohepatic signal to regulate bile acid homeostasis. Cell Metabolism. 2005;2(4):217-225. [Established the FXR-FGF15/19-CYP7A1 feedback axis.]
Lefebvre P, Cariou B, Lien F, Kuipers F, Staels B. Role of bile acids and bile acid receptors in metabolic regulation. Physiological Reviews. 2009;89(1):147-191
Soluble Fiber and Bile Acid Elimination
Anderson JW, Baird P, Davis RH Jr, et al. Health benefits of dietary fiber. Nutrition Reviews. 2009;67(4):188-205. [Comprehensive review of soluble fiber mechanisms including bile acid binding.]
Ripsin CM, Keenan JM, Jacobs DR Jr, et al. Oat products and lipid lowering: a meta-analysis. JAMA. 1992;267(24):3317-3325. [Confirmed oat beta-glucan bile acid binding and LDL reduction in randomized trials.]
Gibb RD, McRorie JW Jr, Russell DA, Hasselblad V, D’Alessio DA. Psyllium fiber improves glycemic control proportional to loss of glycemic control: a meta-analysis of data in euglycemic subjects, patients at risk of type 2 diabetes mellitus, and patients being treated for type 2 diabetes mellitus. American Journal of Clinical Nutrition. 2015;102(6):1604-1614.
Pomegranate and PON1 Protection of HDL
Aviram M, Rosenblat M, Gaitini D, et al. Pomegranate juice consumption for 3 years by patients with carotid artery stenosis reduces common carotid intima-media thickness, blood pressure and LDL oxidation. Clinical Nutrition. 2004;23(3):423-433.
Aviram M, Dornfeld L, Rosenblat M, et al. Pomegranate juice consumption reduces oxidative stress, atherogenic modifications to LDL, and platelet aggregation: studies in humans and in atherosclerotic apolipoprotein E-deficient mice. American Journal of Clinical Nutrition. 2000;71(5):1062-1076.
Exercise, eNOS, and Endothelial Nitric Oxide
Hambrecht R, Wolf A, Gielen S, et al. Effect of exercise on coronary endothelial function in patients with coronary artery disease. New England Journal of Medicine. 2000;342(7):454-460. [Exercise increases endothelial NO production and improves coronary flow.]
Niebauer J, Cooke JP. Cardiovascular effects of exercise: role of endothelial shear stress. Journal of the American College of Cardiology. 1996;28(7):1652-1660.
SR-B1 and Hepatic Cholesterol Delivery
Acton S, Rigotti A, Landschulz KT, et al. Identification of scavenger receptor SR-BI as a high density lipoprotein receptor. Science. 1996;271(5248):518-520. [Original identification of SR-B1 as the hepatic HDL receptor.]
Krieger M. Charting the fate of the "good cholesterol": identification and characterization of the high-density lipoprotein receptor SR-BI. Annual Review of Biochemistry. 1999;68:523-558.
Appendix compiled for educational purposes. Full citations available at ham.com.
I pray you unlock your heart to reach the height of your full potential by discovering your calling.
Kevin Ham, MD
Subscribe to my Compounding Wisdom newsletter and start transforming your life. ham.com
Subscribe to my YouTube channel @DrKevinHam for videos on how I reversed my clogged arteries in 3 months, the top foods that clear your arteries, and the first principles of health that can save your life. Like, share and subscribe — it could save the life of someone you love.
Most Everyone Has Plaque
It may be the biggest secret in the world
It may be the biggest secret in the world
Dr. Kevin Ham, MD
The Way of Life
“For the life of the flesh is in the blood, and I have given it to you upon the altar to make atonement for your souls; for it is the blood that makes atonement for the soul.”
Leviticus 17:11
Would you subject yourself to chemotherapy if you found out you had one cancer cell? How about 100 cancer cells? 1000? A million cancer cells? How about a billion cancer cells? Cancer becomes detectable typically at a billion cells. Stage 1.
Would you take insulin if you found out you were insulin resistant? How about if you were pre-diabetic? How about if you were a Type II diabetic? The average time from full insulin resistance to a diagnosis of diabetes is 13 years. It takes decades to develop insulin resistance. Once pre-diabetic, the average is ~ five years to diabetes.
How about if I told you that if you are over the age of twenty, there is a 77% likelihood that you have plaque growing in your arteries. If you are over fifty, then you have 91% likelihood. This will grow and grow year by year until it occludes your arteries. That is what the data declares again and again over the past seven decades. The average age of a heart attack in men is 61 and in women, 71. And it is the global #1 killer. 20 million people a year. I’m on this hit list but I am learning how to get myself off this list.
Food for thought. This one is a long one but so important that I’m not editing it to half the usual length I write on the first draft.
The Scan
“The CT Artery Calcium scan declared 505. My first instinct was to blame the extreme cycling up mountains. My second instinct, the physician’s instinct, was to go back further. Much further.”
Kevin Ham, MD
I got the calcium scan because Rob, a close friend, died suddenly of a heart attack at 58. Super fit. Seemingly healthy. No warning anyone had communicated to him. And then gone, with the abruptness that only the cardiovascular system can manage, before any of the conversations that were supposed to happen. I am a physician. I left clinical medicine in 2000 thinking I’d build an Internet company for three to six months. I wanted to do health as philanthropy and make $ on the Internet. It’s been 25 years, but the physician’s mind does not leave, and what it does with grief is turn it into a question. Why Rob? Now it’s why me? And who else? What happened?
A calcium score of 505 means significant atherosclerotic burden. Your coronary arteries have been accumulating calcified plaque for long enough that a CT machine can measure the mineral deposits and assign them a number. A score above 400 places you in the highest risk category. A likely heart attack in the next two to five years. Ominous. The standard response in conventional cardiology is statins, aspirin, and watchful management of a disease that will continue to progress.
My first thought, shocking and surprising, thought it must be my extreme cycling. I had been riding the North Shore mountains aggressively for a decade, up to 7,000 kilometers per year at a significant 100,000m of elevation each year with intensity. I knew the literature on extreme endurance athletes and coronary calcification. I wondered whether I had done this to myself. Rob was also an athlete, climbing the Matterhorn three times. Extreme.
I sat on the ledge of my bathtub at two in the morning as I prayed and pondered my result and my future. I had so many questions that I could not answer. How could this be? Then a revelation.
In my few spare moments, I read scientific and medical research studies. The autopsy studies. Mice studies. Human studies. The food studies. The biochemical pathways. Before I had a hard time remembering the differences between LDL and HDL. Now I feel like they are my close friends. The PDAY data. The Bogalusa Heart Study. I now have a good high level overview of what happens to us over the decades.
Why wasn’t this being taught in medical schools? In books? In the news? Why didn’t I ever hear this?
If I hadn’t been exercising, I would likely not be here right now.
It started when I was a teenager.
The Carefree Teenager
“The risk factors that predict coronary heart disease in adults are the same risk factors that correlate with the extent of atherosclerosis in teenagers. The need for risk factor control during adolescence and young adulthood cannot be overstated.”
Henry C. McGill Jr., MD, PDAY Research Group
I grew up eating fried food. A lot. In my thirties, I became health-aware. I was eating organic. But I loved Korean and American fried chicken, tempura, the crisp oil-saturated foods that felt like pleasure and were, at the cellular level, a sustained assault on the endothelial lining of every vessel in my body.
The autopsy literature is unambiguous about when plaques begin. The Bogalusa Heart Study found fatty streaks in the coronary arteries of half the children between ages two and fifteen. The Korean War autopsies of 1953 found gross coronary atherosclerosis in 77% of soldiers with an average age of 22.1 years. My calcium score of 505 was not the product of five years of cycling up mountains. It was the product of four decades of compounding plaque.
Here is what cycling had actually done: it built collateral vessels. Naturally coronary bypasses. When a coronary artery narrows progressively, the body grows alternative routes. Small vessels enlarge and reroute the blood supply. This is why I could ride at the intensity I rode, why I was in the best aerobic shape of my life at 55, and why my CT showed multi-vessel coronary artery disease simultaneously. The cycling had not caused the disease. It had made me functionally elite despite it.
I had the arteries of a man heading for a cardiac event in the next two to five years. I also had the cardiovascular capacity of a competitive athlete. I rode with the fastest in the city. Both were true at the same time.
The Logic of Choice
“I could stent one vessel and watch the others progress. Or I could address the biological process driving every vessel simultaneously. The stent fixes the pipe. The protocol fixes the entire plumbing system.”
Kevin Ham, MD
A June 17 CT angiogram confirmed multi-vessel disease: 77% obstruction in the D1 coronary artery, 55% in the Ramus Intermedius vessel, significant disease in all vessels. Traditional cardiology had a clear pathway: a stent for the 77% lesion, statins, aspirin, regular monitoring. Standard of care. Evidence-based. And, as I thought about it that night, obviously insufficient.
If I stented the 77% vessel, I would fix one obstruction in a system where multiple vessels were diseased and the underlying biological process was still running. The 55% obstruction would continue toward 70%, the conventional threshold for the next intervention. I was 55 years old. On the conventional trajectory: two stents, then three, then a bypass conversation in my sixties.
I thought about Esselstyn. Dr. Caldwell Esselstyn, former Cleveland Clinic surgeon, Phi Beta Kappa from Yale, Olympic gold medalist in rowing, who spent the second half of his career reversing coronary artery disease through diet alone. One of his patients arrived with 100% occlusion of a major coronary artery. At 32 months on the protocol, the angiogram showed complete resolution. The vessel had reopened. He’s a healthy 92 year old still preaching his gospel to reverse heart disease through an oil free whole food plant-based diet. I am very grateful that he has explained why such a simple remedy works. It’s so simple, people will gloss over it. I did so as well, even after listening to his lectures dozens of times. I am rereading his book again with a new lens. How foolish we can be.
I adopted the Esselstyn protocol: whole food plant-based diet, fat held below 25 grams per day, no oils, no animal products.
Then after month one, I added to this foundation dietand layered fasting: 16 to 8 daily, one OMAD (one meal a day) weekly, and two to three days fast monthly.
The HIIT cycling continued, now understood as a targeted delivery of nitric oxide to every coronary endothelial cell with every pedal stroke. My pressure washes for the arteries, once I had established the right biochemical environment for my arteries.
And a synergy stack: Vitamin K2 MK-7 from natto with its nattokinase, fresh garlic, black garlic and aged garlic extract, pomegranate juice, green tea tablets and green tea, 1g of omega-3 fatty acids.
Full Reversal in Just Three Months
“The disease can be stopped and in many patients reversed by a plant-based diet that avoids all oils and significantly reduces fat intake. The body has the capacity to heal if we remove what is harming it.”
Caldwell B. Esselstyn Jr., MD, Cleveland Clinic
The carotid ultrasound at three months showed something I had hoped for but had not been certain enough to expect: both carotid arteries were completely clear. Not reduced. Clear. The plaques had resolved bilaterally in just three months. And the CIMT, the intima-media thickness that had read like an 85-year-old when I started, crossed into high-normal for age 55. By month ten, it was mid-normal. A 53% bilateral reduction in carotid arterial wall thickness, confirmed on imaging another three times afterwards, always improving.
My arterial age dropped 30 years in just 3 months.
The coronary picture is different. The D1 stenosis at 79% (slight increase from 77% and likely just measurement difference) on structural CT imaging. But the CT-FFR, the measure of actual blood flow past the obstruction, improved from 0.75 to 0.80. The pipe looks the same. The river is flowing better. Something is changing in the functional architecture of the vessel before the structural regression becomes visible on imaging. But I was still extremely disappointed that the coronary arteries didn’t regress like the carotids. Why not?
I felt delighted at the carotid result. And underneath the delight, the quieter pressure of a much larger question.
Why the Carotids and Not the Coronaries?
“The carotid artery is a straighter, larger vessel with predominantly laminar smooth flow. The coronary artery is a small, curved vessel embedded in contracting myocardium, subjected to cyclical compression 100,000 times daily. These are not the same biological environment. They are not the same plaque.”
Kevin Ham, MD
I wondered about this for months. Both carotid plaques had vanished on imaging in three months. The coronary plaque had not moved structurally, though the FFR had improved from 0.75 to 0.80, from a stentable reading to a low-normal one. Something was changing in the coronary territory. But not the same thing, and not at the same speed.
I had three hypotheses, and I turned each one over in my long therapeutic rides through the North Shore.
Hypothesis one: Vessel geometry and flow mechanics.
The carotid arteries are relatively straight vessels carrying blood upward to the brain in a predominantly slower laminar flow pattern. Laminar flow is protective: it delivers smooth, directional shear stress to the endothelium, which upregulates eNOS and nitric oxide production. The coronary arteries, by contrast, are small, curved vessels with multiple bifurcations and bends, where flow becomes turbulent and oscillatory at every curve. Turbulent flow creates the low-shear-stress environments that damage the endothelium and invite lipid deposition in the first place. The same turbulence that built the plaque may be slowing its reversal. I had to be prescriptive in my HIIT rides up mountains. I do that by throttling my heart rate to 150 bpm. Temporary rises to 170 bpm, I ease off. My Gran Fondo ride of 125 km last June 8 clocked my heart rate at 172 average for the 4 hours and 18 minutes. And I thought I was taking it easy. My heart was working extremely hard. At that time, I did not yet know the full extent of my disease. Now I do.
Hypothesis two: Vessel diameter.
The carotid arteries are substantially larger in diameter than the coronary arteries. A larger vessel means a given plaque volume represents a smaller fraction of the total wall. The reverse cholesterol transport machinery, the HDL particles and macrophage efflux mechanisms that extract cholesterol from the plaque, must work through a smaller absolute lipid burden relative to vessel size in the carotids than in the coronaries. In a small coronary artery, even a modest plaque represents an enormous proportion of the vessel wall. The biology has less room to work.
Hypothesis three: Plaque age.
This was the one that felt right from first principles. The ASAP study establishes that coronary disease develops earlier in life than carotid disease. The carotid territory follows the coronary in the anatomical sequence of progression. If the carotid plaques arrived later, they were younger lesions: softer, more lipid-rich, less fibrotic, less calcified, more biologically mobile. Young plaque reverses the way young bone heals, faster and more completely than older, denser, more mineralized tissue. My coronary plaques have been building since my teens. My carotid plaques began in my forties. Three decades of additional compounding had made the coronary lesions structurally different and much harder to reverse. Joe Crowe’s reversal happened at 44.
And then the calcification data settled it.
My coronary artery calcium score of 505 confirmed what first principles suggested. Two-thirds of my coronary plaque burden is calcified, Stage 5 in the AHA classification, the equivalent of mature rock. These are lesions that began accumulating calcium in my thirties and forties. The outer shell has mineralized. They are not going to dissolve in three months. They may not dissolve in three years. The biology of calcified plaque reversal is not the biology of soft plaque reversal.
But here is what I also concluded: the non-calcified third of my coronary plaque is still Stage 3 to Stage 4, still lipid-rich, still biologically active, still operating by the same rules that cleared my carotid arteries. Smaller vessels, older lesions, more demanding mechanical environment, yes. But the same reverse cholesterol transport mechanisms, the same nitric oxide pathway, the same eNOS upregulation from cycling, the same DDAH protection from pomegranate and EGCG. The biology does not change. Only the timeframe does.
My realistic expectation: 12 to 24 months to clear the non-calcified coronary component. And for the calcified component, not dissolution but stabilization, depleting the lipid core beneath the calcium so that what remains is an inert mineral shell in a vessel that flows freely. Think of it like osteoporosis in reverse: the mineral remains, but the biological danger inside it is gone.
I expect my coronary FFR to continue improving as the soft plaque recedes. The CT angiogram in June 2028 will either confirm this or refute it. I will report my thoughts and metrics weekly, with labs every 6 weeks and CT scans twice a year.
Where Else?
“Atherosclerotic degeneration progresses most rapidly in the abdominal aorta, followed by the thoracic aorta, coronary arteries, carotid arteries, ascending aorta, and finally the cerebral arteries. Both sexes develop atherosclerosis in the abdominal aorta in the first decade of life.”
ASAP Study, 3,400 Autopsies, Nature Scientific Reports, 2024
If the carotid plaques resolved in three months, when did they develop? If they developed, what was happening simultaneously in my coronary arteries, which the autopsy literature says accumulate disease earlier in the anatomical sequence? And if both territories carry disease that began when I was a teenager, what is happening right now in the arterial territories I cannot image with a simple ultrasound?
My cerebral vessels: the plaque that could embolize to my brain, the same pathway that put a clot in my father’s middle cerebral artery when he was 78, producing complete right hemiplegia he spent months recovering from. My father recovered 90%. I gave him high-dose green tea EGCG and omega-3 fatty acids from the first week, and the biology of both compounds supports recovery of that magnitude. That was in 2014 so I already knew how to reverse plaque. I didn’t realize how at that time, but now that I delve into the biochemical pathways, now I see.
My mesenteric arteries feeding the intestine. My femoral arteries feeding my legs, where I have never felt claudication because the collateral circulation has not yet reached its limit. My thoracic and abdominal aorta, where atherosclerosis weakens the arterial wall and produces aneurysmal dilatation that kills without warning when the wall gives way. I watched a man die of this in the CT scanner when I was a medical resident on my surgery rotation.
And then my eyes.
The Eyes Don’t See
“Wet macular degeneration. Coronary artery disease. Carotid plaque. All in the same body. All, at their biological root, diseases of the vessel wall. I am treating one disease in many locations simultaneously.”
Kevin Ham, MD
On May 10, 2020, I was diagnosed with wet macular degeneration in my right eye. Wet AMD involves abnormal vessel growth beneath the retina driven by VEGF (vascular endothelial growth factor) signaling in a hypoxic, ischemic environment. It progresses rapidly. Ophthalmology considers it chronic and irreversible, managed with regular anti-VEGF injections directly into the eye. A major and severe cause of blindness. My prognosis? Most likely blind in years… unless I receive monthly anti-VEGF shots in each eye until I go blind.
I treated it as a retinal disease, which at its biological root it is. But it’s also a vascular disease. The choroidal vessels beneath the retina are subject to the same atherosclerotic and endothelial dysfunction processes as every other vascular territory. A retina deprived of adequate choroidal blood flow becomes hypoxic. Hypoxia drives VEGF. VEGF drives neovascularization.
Since beginning my REVERSAL protocol, my vision has been improving. The mechanism is coherent: if the protocol restores endothelial function and improves choroidal perfusion the way it restored my carotid arteries and improved my coronary FFR, the hypoxic signal diminishes and the neovascularization recedes. I did not have any eye shots at all for three years. I had to get one last December as I was so focused on my heart, but now that I understand better, my protocol treats both, 80% with the same foundational treatment and 20% more specific for the organ.
How many diseases that medicine treats as isolated organ pathologies are actually systemic vascular disease wearing different masks?
What the Autopsies Declare
“Gross evidence of coronary arteriosclerosis was found in 77.3 percent of the hearts examined. These findings indicate that the development of coronary arteriosclerosis is not primarily a disease of old age.”
William F. Enos, Robert H. Holmes, James Beyer, JAMA, 1953. Autopsied 300 American Soldiers, Average age 22
The medical literature has understood the anatomical sequence of this disease for over seventy years, and has communicated it to the public with remarkable silence.
In 1953, pathologist William Enos (love his last name) published autopsies of 300 American soldiers killed in Korea.
Average age: 22.1 years.
Finding: 77.3% had gross evidence of coronary arteriosclerosis.
The paper should have reoriented how medicine thinks and talks about cardiovascular disease. It changed very little.
Gerald Berenson spent 38 years tracking the children of Bogalusa, Louisiana. When cohort members died of accidents, he examined their arteries. Fatty streaks in the aorta: present in every individual.Fatty streaks in the coronary arteries: present in half of the children between the ages of two and fifteen.
Two years old!
The ASAP study, 3,400 autopsies across six arterial territories, confirmed the sequence:
abdominal aorta in the first decade of life,
then thoracic aorta,
then coronary arteries,
then carotid arteries,
then ascending aorta,
then cerebral arteries.
By the sixth decade of life, 42% of individuals have Grade III coronary stenosis and 25% have Grade IV.
Everyone has this disease. Almost no one is told.
Why this Artery, Why this Stage?
The ASAP study did not just document that atherosclerosis is universal. It documented that it follows a fixed anatomical sequence with a precision that looks almost designed. The abdominal aorta before the thoracic. The coronary arteries before the carotid. The carotid before the cerebral. This sequence is not random. Each step follows from the physical mechanics of blood flow operating in that specific vascular territory.
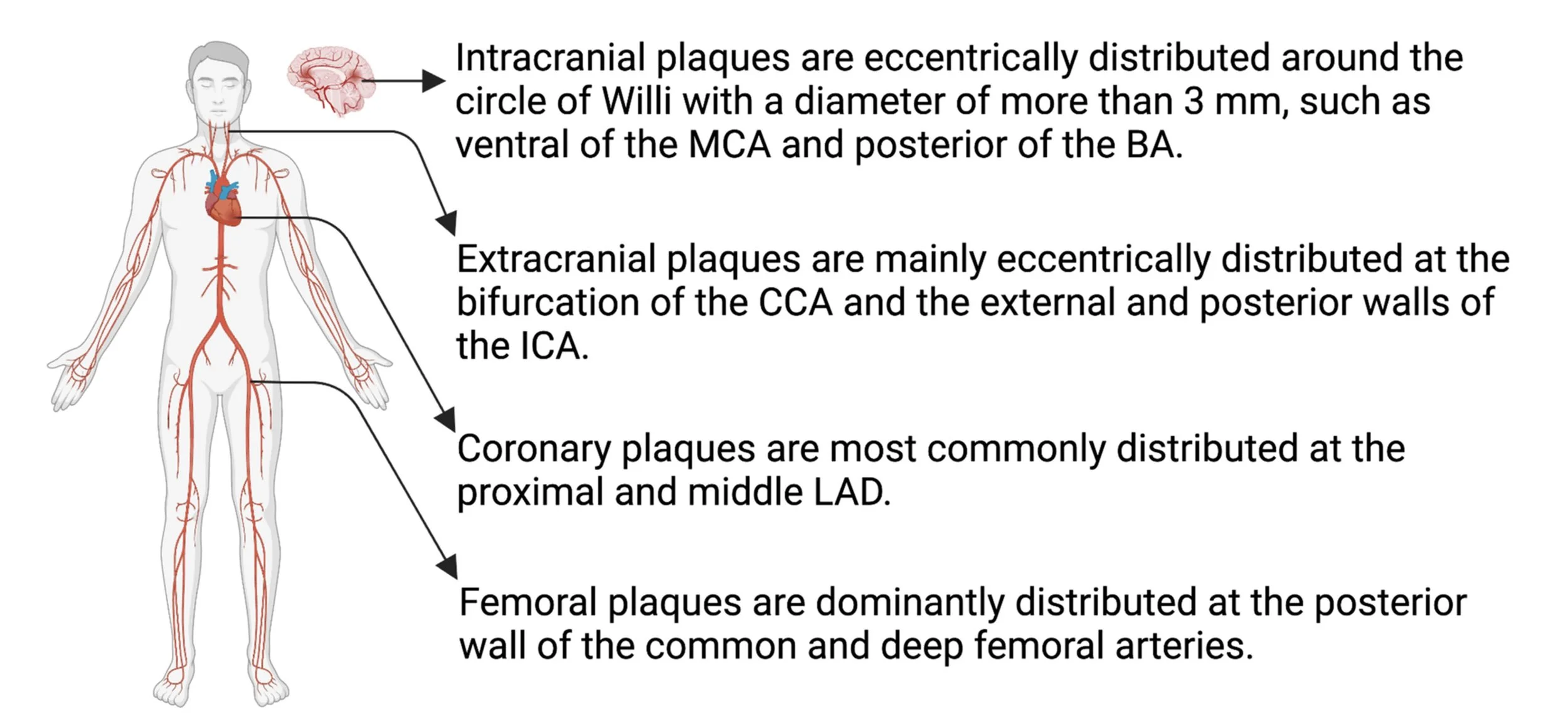
The Six Arterial Territories in Order
1. Abdominal Aorta : First Decade of Life
The abdominal aorta is the first territory because it experiences the greatest oscillatory shear stress in the body. Blood leaving the heart travels as a smooth column through the thoracic aorta, but when it reaches the aortic bifurcation and the origins of the renal and mesenteric branches, the flow becomes turbulent and disturbed. Turbulent flow does not polish the endothelium. It damages it. Lipids accumulate preferentially at the outer walls of branches and at the posterior intimal surface, exactly where the PDAY study found the earliest lesions. It becomes critical when aneurysmal dilatation exceeds 5.5 centimeters, at which point the law of Laplace dictates that wall tension is proportional to radius: the wider the aorta, the more force trying to burst it open. Rupture is catastrophic and nearly always fatal within minutes.
2. Thoracic Aorta : Decades One to Two
The thoracic aorta is large in diameter and exposed to the highest pulse pressure in the body: it receives the full force of every cardiac ejection. The mechanical stress on the intima is enormous. But because the thoracic aorta is also large in diameter, the disease progresses for decades before it becomes flow-limiting. It becomes critical when atherosclerosis weakens the medial layer enough to permit aortic dissection, the catastrophic tearing of the inner aortic wall that allows blood to enter and propagate through the wall itself. Thoracic dissection can shear off the coronary arteries, the carotid arteries, and the spinal arteries simultaneously. It is survivable only with immediate surgery and kills approximately 50% of patients before they reach the hospital. This occurred to our good neighbour’s husband last summer. It’s devastating!
3. Coronary Arteries : Decades Two to Three
The coronary arteries are small vessels with a biologically unique environment: they are compressed with every heartbeat, experiencing systolic compression and diastolic perfusion in a cycle that repeats 100,000 times per day. The bending points, the bifurcations of the left anterior descending artery, the origins of the diagonal branches (that’s me 77% at D1), the curve of the right coronary artery, are where low and oscillatory shear stress creates the endothelial vulnerability that lipid deposition exploits. The LAD is the most commonly and severely affected coronary artery in every autopsy series ever published. It becomes critical at 70% stenosis, where the CT-FFR begins to fall below 0.80 and resting perfusion starts to be impaired. My D1 is at 77%. Below 0.75 the territory is ischemic at rest. My FFR is 0.80, low normal now in a 77% obstruction. Remarkable!
4. Carotid Arteries : Decades Three to Four
The carotid arteries develop disease after the coronary arteries in the anatomical sequence. The relative ease of carotid ultrasound and low cost make the carotids the clinical indicator of systemic arterial age. The disease concentrates at the carotid bifurcation, where the common carotid artery divides into the internal and external carotid arteries. At this bifurcation, the geometry creates a flow separation zone on the outer wall of the internal carotid where shear stress is chronically low, the exact condition that promotes endothelial inflammation and lipid infiltration. Carotid plaques are 70 to 90% lipid-rich, making them the most biologically active and the most responsive to reversal. They become critical when they rupture and embolize upstream, producing embolic stroke, or when they cause critical stenosis above 70% that reduces cerebral perfusion.
5. Cerebral Arteries : Decades Four to Six
The cerebral arteries are the last territory to develop significant disease because they are intracranial vessels with structural properties different from extracranial arteries: thinner walls, no external elastic lamina, and a different smooth muscle architecture. The blood-brain barrier environment also partially shields them from the systemic lipid and inflammatory burden that damages peripheral vessels. But once the upstream disease in the carotid and aortic territories is established, the cerebral arteries receive two simultaneous threats: in-situ plaque formation within the intracranial vessels themselves, and embolic disease traveling from the carotid and aortic territories. It becomes critical when it produces lacunar infarction from small vessel occlusion, or when a cerebral aneurysm at the branching points of the Circle of Willis ruptures, causing subarachnoid hemorrhage, with a mortality rate exceeding 50% in the first 30 days.
6. Femoral and Peripheral Arteries : Decades Four and Beyond
The femoral arteries develop disease later than the coronary and carotid arteries in the sequence, yet in adults they carry more total plaque burden than any other arterial territory: 76% prevalence compared to 45% coronary and 35% carotid in population studies. This paradox exists because the legs have extraordinary collateral vascular capacity that compensates silently for decades. It becomes critical at 60 to 70% stenosis when the collateral reserve is exhausted and claudication appears: ischemic cramping in the calf or thigh with walking that resolves with rest. Beyond that: rest pain, non-healing ulcers, gangrene, and amputation.
The Six Stages of Plaque
Think of this the way oncologists think of cancer staging. Stage 1 breast cancer and Stage 4 breast cancer are different diseases wearing the same name. The staging communicates biological reality, urgency, and probability of reversal in a single number. Atherosclerotic plaque has never been routinely staged for patients. Medicine says coronary artery disease as though that phrase means something specific. It does not.
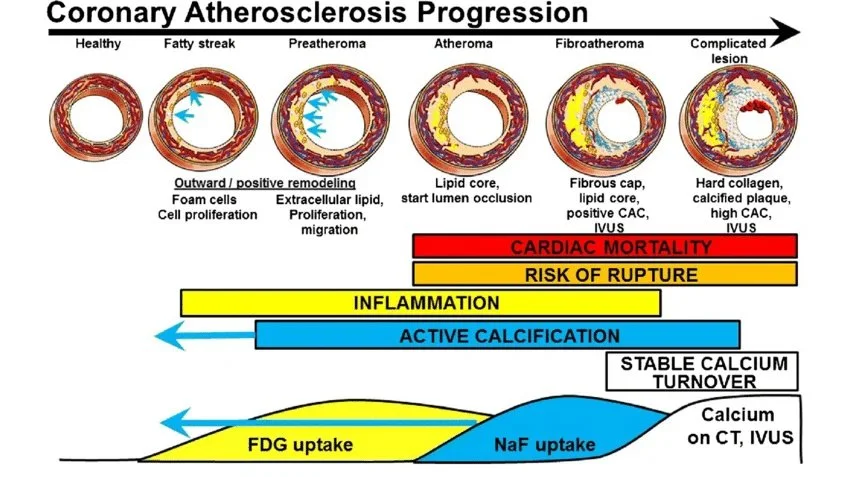
Stage 1: Fatty Streak
Isolated macrophage foam cells accumulate in the intima. No structural disruption. No fibrous tissue. No lipid core. Lipid is entirely intracellular.
When: Childhood and adolescence. Present in every individual in an industrial diet culture. Bogalusa found it in two-year-olds.
Threshold: None. Fully reversible.
Reversal probability: Near 100% with dietary intervention.
Stage 2: Preatheroma
Extracellular lipid pools begin to form. The arterial wall is thickening but no defined lipid core exists yet. CIMT begins to rise above age-expected norms.
When: Teens through early twenties in high-risk individuals.
Threshold: None, but this is the stage where CIMT imaging first becomes abnormal.
Reversal probability: Very high. The extracellular lipid pools are not yet organized into a necrotic core.
Stage 3: Soft Atheroma
A confluent lipid-rich necrotic core has formed, covered by normal-appearing intima. No fibrous cap yet. This is the stage most vulnerable to rupture because a large lipid core behind a thin or absent cap is structurally unstable.
When: Late twenties through forties. This was my carotid plaque stage. Three months of the REVERSAL protocol cleared it completely.
Threshold: Rupture risk is high despite often modest stenosis. The 2018 SCOT-HEART data showed that low-attenuation plaque volume, the CT signature of this stage, is the strongest single predictor of heart attack, outperforming calcium score, stenosis severity, and every standard risk calculator.
Reversal probability: High. 70 to 90% with aggressive protocol.
Stage 4: Fibroatheroma
A fibrous cap now covers the lipid-rich necrotic core. The plaque has organized into a two-layer architecture: lipid engine underneath, fibrous shield on top. Early calcification may be present.
When: Forties through sixties.
Critical threshold: The fibrous cap can thin and rupture, exposing the lipid core to flowing blood and triggering acute coronary syndrome. Thin-cap fibroatheroma with a cap under 65 microns is the architecture responsible for the majority of fatal heart attacks.
Reversal probability: Partial. The lipid core can regress through RCT (reverse cholesterol transport). The fibrous cap is more resistant to remodeling.
Stage 5: Calcified Plaque
Dense calcium deposition within the necrotic core and fibrous cap. The plaque has mineralized. This is where my coronary disease currently sits, with a CAC score of 505. The calcified component is structurally more stable against rupture, but it is hemodynamically significant when it causes stenosis.
When: Fifties through seventies.
Threshold: Stenosis above 70% with CT-FFR below 0.80 indicates hemodynamically significant flow limitation. My D1 is at 77%, CT-FFR 0.80.
Reversal strategy: deplete the lipid core and macrophage burden inside the calcified scaffold, leaving an inert calcium shell. The calcium does not have to disappear for the threat to be neutralized.
Stage 6: Complicated Lesion
Surface disruption, intraplaque hemorrhage, or superimposed thrombus. This is the plaque that has crossed the threshold into acute coronary syndrome. The fibrous cap has ruptured or eroded. The lipid core is exposed to flowing blood. Platelet aggregation and thrombus formation proceed within minutes. We call this a heart attack.
When: Can occur at any stage but is most common at Stage 3 and Stage 4. Paradoxically, Stage 5 calcified plaques are more structurally stable and less likely to rupture acutely.
Threshold: This is the event. Myocardial territory is lost proportional to the duration and completeness of occlusion.
Reversal probability: The acute event cannot be reversed. But the remaining disease in every other vessel can be. Where you need to stent, bypass.
The most dangerous plaque is not the most calcified. It is the softest, most lipid-rich, least conspicuous lesion in the vessel wall, the one that does not restrict flow enough to cause a stress test abnormality, does not produce a high calcium score, and produces no symptoms until it ruptures.
The Life of the Flesh is in the Blood
“Nitric oxide is the body’s natural cardiovascular wonder drug. Produced by the endothelium, it keeps blood vessels dilated, prevents clotting, and inhibits the inflammation that drives atherosclerosis. Every lifestyle choice either supports or destroys that capacity.”
Louis J. Ignarro, PhD, Nobel Prize in Physiology or Medicine, 1998
I have read Leviticus 17:11 a hundred times. The life of the flesh is in the blood. I always received it as theology: a truth about atonement, about sacrifice. I filed it under faith.
It was not until I sat with my CT angiogram in my hands that I understood what it is also saying at the biological level. The life of every organ, every cell, every tissue depends entirely on the blood reaching it. When the blood stops reaching, the flesh dies.
I had always thought about what was inside the blood: the red cells carrying oxygen, the white cells mounting immunity, the platelets sealing breaches, the hormones and nutrients riding the current. I thought of blood as the delivery truck and the garbage truck simultaneously. What I never thought about was the vessel itself.
The endothelial cell is the single layer of cells lining every blood vessel in the body. One cell thick. Covering more than 7,000 square meters of surface area in an adult. Not passive. Not the walls of the pipes. An active endocrine organ that produces nitric oxide, the master vasodilator and endothelial protector, that senses shear stress from blood flow and responds by remodeling the vessel wall.
When the endothelium is injured, everything downstream of it fails. Heart disease is endothelial disease. Stroke is endothelial disease. Aortic aneurysm, pulmonary embolism, deep vein thrombosis, cerebral aneurysm, and very likely wet macular degeneration: all begin, at the biological root, with an endothelium damaged beyond its capacity to repair.
“We have identified a naturally occurring compound that inhibits nitric oxide synthesis in blood vessels. Its concentration in blood is sufficient to tonically suppress nitric oxide production. When it accumulates, vascular tone increases, endothelium-dependent relaxation is impaired, and the stage is set for atherosclerosis.”
Patrick Vallance et al., The Lancet, 1992. First description of ADMA as an endogenous cardiovascular risk factor
The specific mechanism: the amino acid L-arginine, drawn from food, enters the endothelial cell and binds to eNOS, endothelial nitric oxide synthase. eNOS converts arginine to nitric oxide. The nitric oxide dilates the vessel, prevents platelet adhesion, inhibits inflammation, and keeps the arterial surface clean.
There is a molecule called ADMA. Asymmetric Dimethylarginine. It is produced in every cell as a byproduct of normal protein metabolism. ADMA is structurally almost identical to arginine. The only difference is two methyl groups added to the same nitrogen atom on the guanidino end. That difference is invisible to eNOS. The enzyme cannot distinguish arginine from ADMA until it is already bound. When ADMA occupies the eNOS active site, nothing is produced. No nitric oxide. The factory is running. Nothing comes out.
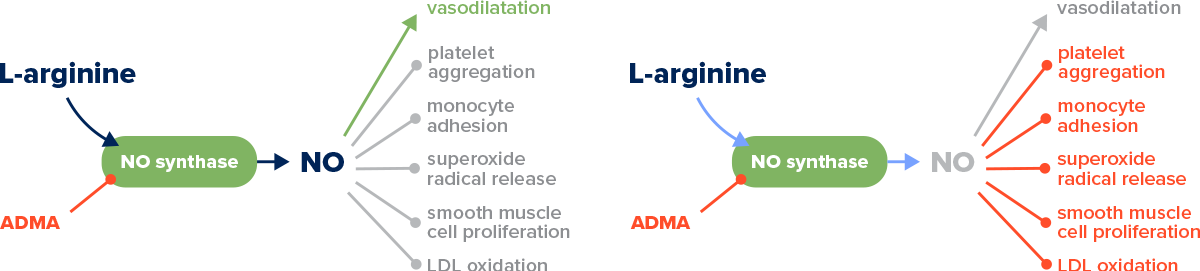
ADMA impersonates the molecule the endothelium needs to protect itself, and in that impersonation, silences the one signal that keeps the arterial wall from becoming the birthplace of plaque.
The rescue enzyme is DDAH, dimethylarginine dimethylaminohydrolase. DDAH breaks down ADMA into citrulline and dimethylamine, clearing more than 80% of circulating ADMA. A meta-analysis of 22 prospective studies found that individuals in the top third of ADMA values had a 42% higher risk of cardiovascular events, 39% higher risk of coronary heart disease, and 60% higher risk of stroke.
What destroys DDAH: the Western diet.
Oxidized LDL directly inactivates DDAH and elevates ADMA simultaneously, a spiraling feedback loop.
High homocysteine down-regulates DDAH production at the genetic level.
Smoking, hyperglycemia, hypertension, and chronic inflammation all independently inactivate DDAH through oxidative mechanisms.
The dietary countermeasure operates on both sides.
Plant foods stock the substrate:
Pumpkin seeds at 5,200 mg of arginine per 100g,
Soybeans at 2,300 mg,
Lentils at 1,900 mg,
Chickpeas at 1,300 mg,
Black beans at 1,000 mg.
On the other side, polyphenol antioxidants protect DDAH from oxidative destruction:
Green tea EGCG,
Pomegranate punicalagins, and
Omega-3 fatty acids.
Every element of the Reversal protocol targets this pathway as well.
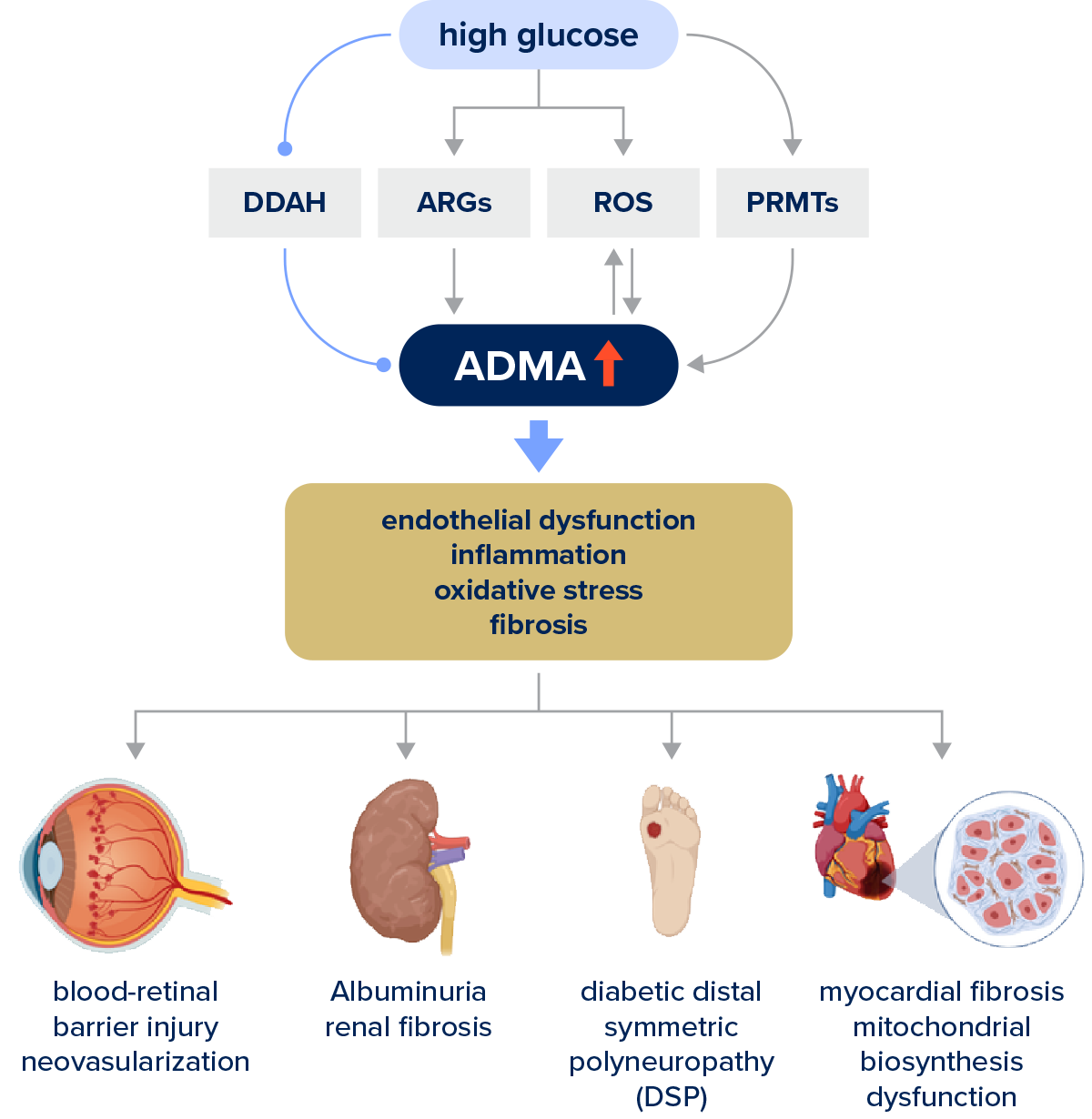
When I saw this diagram in a study, I thought, “Eureka!” Blood-retinal barrier injury neovascularization. That was my wet macular degeneration! And on the other side, heart. Same mechanism. Endothelial dysfunction. Increased ADMA.
Now I am sure I can heal my Wet AMD along with my heart disease. And not only I, but everyone who follows me.
The Question for Everyone
“Everyone has this disease. The question is not whether it has started. The question is whether it will be permitted to finish.”
Kevin Ham, MD
This is not only my question. The anatomy does not discriminate. If you are reading this, you almost certainly have this disease in some stage, in some arterial territory, accumulating silently. The question is not whether it has started. The question is which stage, which vessels, and whether the biological machinery of reversal can be activated before the disease reaches the threshold at which it announces itself.
The protocol I am running exists not as a personal experiment but as a proof of concept. If it works in my arteries, and the carotid data says it is working, then it works through mechanisms that are universal in human biology. The endothelium that repaired in my carotid territory responds to the same signals as the endothelium in your coronary arteries, your cerebral vessels, your retinal circulation.
My father is still here. Thank you God. My CT angiograms are scheduled every six months and my target for reversal is June 2028. That is the reckoning.
Water erodes rock. The river does not stop.
Your Questions
“Everyone has this disease. The question is not whether it has started. The question is whether it will be permitted to finish.”
Kevin Ham, MD
Questions worth sitting with
For yourself. For someone you love. Answer them in the quietness of your day.
1. When did you last have imaging of your arteries, not just blood tests?
A lipid panel tells you risk factors. A CAC score or CT angiogram tells you what has already built up in the vessel wall. These are not the same question. Call your physician tomorrow and ask for a coronary artery calcium scan.
2. What did you eat yesterday and what was that food doing to your nitric oxide production?
Every meal either elevates ADMA and silences eNOS, or it provides the arginine and polyphenols that protect DDAH and keep your endothelium producing the signal that keeps your arteries open. There is no neutral meal.
3. Who in your life has this disease right now and does not know it?
You thought of someone while reading this. Forward this to them. Ten seconds. It may matter more than either of you knows.
MORE READINGS YOU’LL ENJOY
Health
Watch: The 2 Foods That Reverse Heart Plaque (Half a Million Views)
Reversing My 77% Heart Plaques
Stats Say You Likely Have Heart Plaque
The Healing Power of Food: Nitric Oxide
Wealth
The Power of the Compound Effect
Relentless Iteration to Mastery
Meaning
The Courage to Your Magnum Opus
APPENDIX
The ten studies that anchor the science in this newsletter.
https://www.frontiersin.org/journals/endocrinology/articles/10.3389/fendo.2023.1183586/full
Elevated ADMA, an endogenous inhibitor of nitric oxide synthase, drives the onset and progression of diabetic microvascular complications including retinopathy, nephropathy, neuropathy, and cardiomyopathy through endothelial dysfunction, oxidative stress, inflammation, and fibrosis.
https://www.frontiersin.org/journals/physiology/articles/10.3389/fphys.2012.00132/full
Examines how vascular aging impairs endothelial function primarily through reduced nitric oxide bioavailability, identifying ADMA accumulation, oxidative stress, enhanced vasoconstrictor activity, and low-grade inflammation as the key mechanisms driving age-related cardiovascular dysfunction.
https://eaglebio.com/eaglebio-biomarker-spotlight-adma/
ADMA is an endogenous molecule detectable in human blood and urine that is structurally homologous to L-arginine and acts as an inhibitor of nitric oxide synthesis,positioning it as a clinically measurable biomarker of endothelial dysfunction and cardiovascular risk.
I pray you unlock your heart to reach the height of your full potential by discovering your calling.
Kevin Ham, MD
Subscribe to my Compounding Wisdom newsletter and start transforming your life. ham.com
Subscribe to my YouTube channel @DrKevinHam for videos on how I reversed my clogged arteries in 3 months, the top foods that clear your arteries, and the first principles of health that can save your life. Like, share and subscribe — it could save the life of someone you love.
Strike the Rock
And Let Your Waters Flow
And Let Your Waters Flow.
Dr. Kevin Ham, MD
The Signal
“The gap between what medicine knows and what people are told is where 695,000 Americans die every year. I started a YouTube channel because video was the fastest way to close it.”
Caldwell Esselstyn Jr., MD. Cleveland Clinic.
Three months ago, I started a YouTube channel. My daughter graduated from film school. Talented. She had an eye for it. And I had an artist at my company who understood how to build something visually. So we started shooting.
The idea was simple. Save lives. Help people understand what disease really is and how to reverse it through lifestyle medicine. More specifically, through food and exercise. I wanted to help prevent the number one global killer from doing what it does every single year: killing 20 million people. Not in a war. Not in a pandemic. Quietly. In gyms and kitchens and bedrooms and hospital corridors. People who did not know what was building inside them until the moment it was too late to stop.
Three weeks ago, I had 1,000 subscribers.
And then one video changed everything. Then two, then three videos. Viral. People were sharing it with their loved ones. Another answered prayer.
Within a week, it had 630,000 views and counting. My channel crossed 24,000 subscribers in under two weeks. The comments came in faster than I could read them. And what struck me, what has not stopped striking me, is what people were actually asking. They were not asking about the latest drug trial or the newest surgical technique. They were asking a much simpler question—a much older one.
Watch the channel: youtube.com/@DrKevinHam
Top video: 2 Foods That Dissolve Heart Plaque
How do I stop this from killing me? How do I separate what actually works from the noise? How do I find the signal?
That is what this newsletter is. A signal. Not a wellness guide. Not a supplement list. Here is what it covers:
✓ What the science says about what builds plaque
✓ What stabilizes it before it kills you
✓ What reverses it, documented in peer-reviewed studies
✓ What dramatically reduces the chance of a heart attack, stroke, or sudden cardiac death
✓ And now I am realizing, the principles that reverse heart disease reverse all our modern diseases.
I am a doctor who became a patient. And I am telling you what I wish someone had told Rob, had told me ten years ago.
Before you read further, I want to ask you something.
Is there anyone you know who has heart disease? Who has died of a heart attack? Who has had a stroke? Who has gone blind from vascular disease?
Do you believe that when you turn 50, you will have no plaque or disease in your arteries?
How about at 60? How about at 70? Will you spend the last decades of your life in disease and suffering?
If you even thought yes, then this is for you. Educate yourself. Don’t leave your valuable the health in the hands of others.
Here is what the people watching already know. These are just 3 comments from many:
Just had an endarterectomy. Left side still 50% blocked. Starting pomegranate juice and nattokinase. Thank you Doc. @averagejoe7333
Cleared 20 to 25% of plaque in 3 months. Incredibly inspiring. Focusing on lifestyle now. @SmartWellnessTips
74 years old. Better late than never. God bless your ministry because that is what this is. @princesstoby653
The Vow
“I will give you a new heart and put a new spirit within you; I will remove the heart of stone from your flesh and give you a heart of flesh.”
Ezekiel 36:26
I was 14 years old, lying in a hospital bed, genuinely believing I was dying. My immune system had declared war on my own body. The disease was Henoch-Schönlein Purpura, an autoimmune vasculitis in which the immune system attacks the blood vessels, causing them to leak. I was a child, frightened, and in that fear, I made a vow. If God, if the universe, allowed me to survive, I would become a doctor. I would spend my life doing for others what the doctors around me were trying to do for me: finding the cause, naming the disease, fighting back against it.
I survived. I kept the vow.
Then I got busy. The vow faded from my memory as I got busy with business. And for 25 years, I tried to understand medicine, but it was more theory than truth. I stood on the physician's side of the room and believed I understood what it meant to be sick. I did not. Not really.
Then I became a patient.
When I found out that I had a CT calcium score of 505, in the worst 90th percentile for heart attack risk, and that I had coronary plaques in every vessel, I was humbled into the depths of my life—77% stenosis, 55%, 45%, everywhere. The numbers did not feel like numbers. They felt like a verdict.
Before that, the warning shockwaves: on the morning of May 10, 2020, severe wet macular degeneration announced itself in my eyes—first the right, then the left. A straight line is bent. Vision distorted—the unmistakable signature of fluid beneath the retina. I was only 50 years old. Wet AMD is a disease of the 70s and 80s. I was 20 to 30 years too early. Even if I were able to live a long life, I was told, it would likely be in blindness—no cure yet known. I was looking at a future in the dark.
I had literally a heart of stone, in my coronary arteries and in my retina. Also, in my will, blocking my understanding and my purpose. The calcified endothelium, the resistant heart, the stiffened soul: all the same condition. And I had not seen it coming.
All of a Sudden
“Create in me a clean heart, O God, and renew a right spirit within me.”
Psalm 51, written after Nathan said: you are the man
On the morning of February 10, 2025, my friend Rob Thompson, 58, a 35-year Goldman Sachs veteran, got up at dawn, made his favourite black tea, went to his home gym to train, and died on the elliptical. He was supposed to fly to Vancouver that day to see me. We had texted the night before. See you tomorrow. He had no warning, no prior cardiac event, no alarming stress test. Inside his arterial walls, an internal mountain was building, one that he did not know he had to climb, with each effort he toiled upon his heart, until that morning of February 10, on his elliptical, he fell off the cliff inside—all of a sudden.
I want to tell you who Rob was. Rob was one of the most physically disciplined people I knew. He had attempted the Matterhorn twice before. The Matterhorn. A 14,692-foot pyramid of rock and ice on the Swiss-Italian border, one of the most iconic and demanding alpine climbs in the world. To attempt it, you train for months: back-to-back mountain days carrying a 30-pound pack, 3,500 feet of elevation gain on consecutive days, cardiovascular sessions of four to six hours at sustained effort, and rock climbing in boots on technical terrain. You build to a cardiovascular fitness level that puts you in the top fraction of the population. Summit day itself starts at 4 in the morning, in the dark, from the Hörnli Hut at 10,700 feet. You climb for eight to twelve hours. The ascent is 1,200 meters of vertical, with fixed ropes on the upper section, crampons on snow and ice near the top, exposed ridges where a fall means death, and thin air that taxes even elite athletes from the first hour. Your heart rate climbs and stays there. Your legs burn with lactic acid. Your fingers ache on cold rock. The descent, on the same technical terrain, exhausted and in fading light, demands more concentration than the ascent. The mountain has killed over 500 people since its first ascent in 1865. It does not forgive a lapse.
Rob attempted it twice. Both times, the mountain turned him back. Weather. Conditions that could not be negotiated with, the kind of danger that an experienced climber recognizes and respects and retreats from. He went home. He trained harder. He prepared again. And on his third attempt, despite difficult conditions on the upper mountain, Rob Thompson summited the Matterhorn. He told me it was one of the proudest moments of his life.
This was not a man with a hidden weakness. He was brilliant, financially exceptional, and by every external measure, in superb physical condition. A man who had trained his cardiovascular system to perform at 14,000 feet in thin alpine air for twelve hours at a time. And inside his arterial walls, for forty years, a mountain of disease had been building—all of a sudden.
Rob's death reminded me of the vow. Of what I had promised to do with this life if I was allowed to keep it. This newsletter, every video I make, every data point I track in my own body, is the vow made good. It is for Rob. And it is for you.
What Medicine Knows and What Medicine Does
“We require a new yardstick to measure cardiovascular excellence. No longer will the number or quality of interventions and their temporary benefits suffice. Heart disease is a toothless paper tiger that need not exist, and if it does exist, need not progress.”
Caldwell B. Esselstyn Jr., MD. Cleveland Clinic, 2000
Here is the indictment. Rob Thompson did not die because science failed him. Rob died because none of it reached him. Not from his cardiologist. Not from his annual physical. Not from a system that tracked his LDL, prescribed him a statin, and sent him back into the world with a clean bill of health.
The gap between what medicine knows and what medicine does is where people die. Heart disease kills approximately 695,000 Americans every year. The Esselstyn protocol was first published in 1995. That is thirty years of documented reversal evidence, and it still is not the standard of care. The number of people who have died in that gap is not a rounding error. It is a generation. They were not Goldman Sachs executives who climbed the Matterhorn. They were John, your neighbour, who mowed his lawn on Saturday and did not wake up on Sunday. John had no reason to believe he was running out of time. No one had told him to look at his arterial wall. They deserved at least the option to take the simple healing remedy, rather than just management and short-term fixes.
This is not a failure of knowledge. It is a failure of transmission. The only way to close the gap is to pass the knowledge directly, person to person, outside the system that has failed to carry it. This is why I am writing this. To inform and educate. And to have people join me in my journey to climb down the mountains in my own blood vessels.
What Has Been Pressed Upon Me
“I saw it and it has been pressed upon me. And I want to press it upon you. These studies, seen over and over again, ingrained in the brain. Imprinted in the heart. Move to action.”
Kevin Ham, MD
I want to press something upon you. Not gently. With the full weight of what I have seen in the imaging, the studies, and the grief of people whose losses were preventable.
Picture a room of 100 people over the age of 50. 91 of those 100 have measurable, visible plaque in their coronary arteries right now. 91 who consider themselves generally healthy, who have been told their cholesterol is fine, 91 who do not know.
And it starts earlier than we want to believe. Korea, 1950. Army pathologist William Enos autopsied 300 soldiers, average age 22, fighting a major war:
77% had visible, gross atherosclerosis in their coronary arteries
5% had 90% or greater obstruction of at least one major coronary artery
Virtually none had symptoms or knew anything was wrong
If the bullets had not killed them, the Western diet would slowly do so decades later.
“The wall is already building. The question is only whether you know it, and what you do next.”
In 2018, researchers found the mean area of ruptured lipid-rich plaque in sudden cardiac death hearts:
0.34 square millimeters.
When I first saw my coronary CT, my low-attenuation plaque was only 0.1 percent. That number sounded reassuring. It was not. Low-attenuation plaque accounts for 70 to 90 percent of all heart attacks that result in sudden death. The SCOT-HEART trial confirmed it beats every other predictor of heart attack, including the calcium score.
5× higher risk of heart attack for patients with low-attenuation plaque burden over 4% of coronary vessel volume. This single measure outperformed every other predictor: risk scores, calcium score, and stenosis severity—all of them.
24 Patients. 12 Years. One Cardiac Event.
“We both agreed. It is so simple. Anybody can do it. Just that. No one has the mindset to do so. Not to save even their own lives, or the lives of people around them.”
Kevin Ham, MD, reflecting on his call with Dr. Esselstyn at age 92
In 1985, Dr. Caldwell Esselstyn recruited 24 patients at the Cleveland Clinic, all with severe coronary artery disease, five of them told they had less than a year to live. No exercise protocol. No sleep program. No meditation. Just a low-fat, whole food, plant-based diet for 12 years.
The result: essentially one subsequent cardiac event among adherent patients. Among the six who returned to standard care, 13 new cardiac events occurred. Thirteen. Against one. In end-stage patients who could barely walk to the end of the block.
His oldest patient was Stanley. Eighty-seven years old. His cardiologist had told him he needed bypass surgery. The surgery might kill him. He was referred to Dr. Esselstyn not in hope, but because of the absence of alternatives. He was a grandfather. He had things he still wanted to do. Stanley started the diet. Within days, he felt better. One day, he called and said, "I just wanted to thank you. I never thought I would live to be 100.
He called every year after that. This year he called at 103. He is now 11 years older than the doctor who saved his life. What do you say to a man who gave you a life you were not supposed to have? Stanley says: I just wanted you to know I am still here. And Esselstyn says: I know, Stanley. I know.
I spoke to Dr. Esselstyn on a Zoom call two weeks ago. He looked at me and said something I have not stopped thinking about since: Can you get plaque from broccoli? From arugula? From beans? You cannot. The disease comes from what we feed the endothelium. Feed it whole plants, and it heals itself. Nobody in medicine argues with the data. They just do not change what they prescribe.
I cannot unsee the images from his book, Prevent and Reverse Heart Disease. That book is the foundation of my protocol. It is the manual I wish I had been given the day of my diagnosis. I hope to one day thank him in person for reversing my extensive plaque and for helping others do the same. I pray he lives a long and blessed life. I am so grateful to him. And to God. And to my family. Blessed beyond measure.
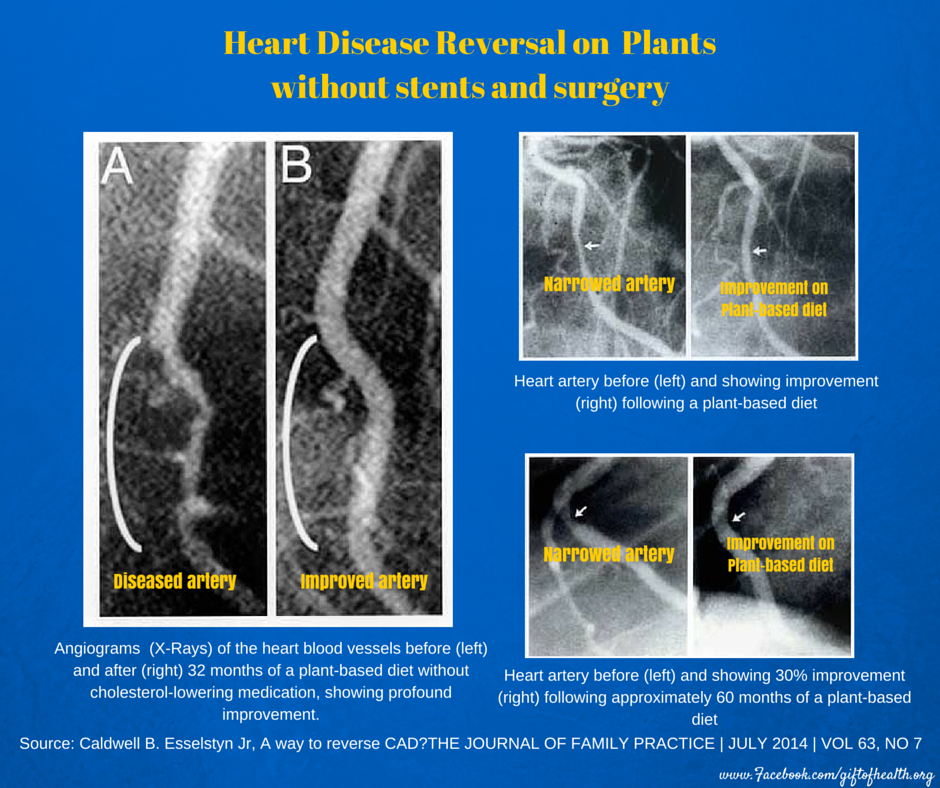
Dr. Joe Crowe: complete reversal of 100% LAD occlusion at 32 months on the Esselstyn WFPB protocol. Before and after angiogram. Cleveland Clinic. Esselstyn CB Jr. Prevent and Reverse Heart Disease. 2007.
Why It Did Not Tip
“The tipping point is that magic moment when an idea crosses a threshold, tips, and spreads like wildfire. There is a simple way to package information that, under the right circumstances, can make it irresistible. All you have to do is find it.”
Malcolm Gladwell, The Tipping Point. 2000
Here is the question that keeps me awake. William Enos published his autopsy findings on Korea in JAMA in 1953. Irrefutable data. The most respected journal in medicine. And nothing changed. Caldwell Esselstyn published his 12-year reversal data in 1999: one cardiac event among adherent patients versus thirteen among those who returned to standard care. Diet alone. And nothing changed.
Why did it take a doctor posting videos online to move 600,000 people in a week when peer-reviewed data could not move the cardiology establishment in seventy years? Because data is not sticky. Story is. Data is processed in the part of the brain that manages information. Story is processed in the part that manages identity. When you read that 91 percent of people over 50 have plaque, your brain files it. When you read about a 58-year-old man who got up at dawn, made his favourite tea, and fell off the cliff inside on his elliptical, your brain does not file it. It flinches. That flinch is the beginning of change. The Korea data had no face. Esselstyn's data did not have a YouTube channel. I am posting videos with my daughter and a gifted artist, telling you what happened to my arterial wall and what I did about it. Not more rigorous than the JAMA study. But stickier. And sticky is what saves lives.
This newsletter and these videos do not describe the tipping point. They are the tipping point. And I pray that you see that it is not only in others around you. But that it is in you. I made this grave error for 25 years. But now I know. And now you do too.
Strike the Rock
“I will stand before you there on the rock at Horeb, and you shall strike the rock, and water will come out of it, that the people may drink.”
Exodus 17:6
There is a moment in Exodus I keep returning to. The people are in the wilderness, catastrophically thirsty, no water in sight. Moses strikes a rock with his staff. Water pours out. The people drink. They live. What strikes me is not the miracle. It is the object. Not a river. A rock. The hardest thing. The most unyielding thing. And out of the rock, water.
I thought about this when I looked at my carotid images. What I had inside my arterial wall was not soft tissue. It was plaque that had hardened, visible on ultrasound, that a close physician friend described as among the worst he had seen in a 55-year-old man. When the arterial wall becomes rock, the blood cannot flow freely. The organs that depend on that flow begin to fail. The water of life is inside you. The question is whether the rock will yield it. Mine did.
The Rock Inside: What Calcification Is
“Your arteries are not passively accumulating calcium the way a kettle accumulates scale. They are actively building bone, running the same molecular program that builds your skeleton, reprogrammed by inflammation.”
Kevin Ham, MD
Atherosclerosis begins as an insult to the endothelium. LDL particles penetrate, oxidize, trigger foam cells, and build a necrotic core under a fibrous cap. When that cap tears, the clotting cascade activates instantly. This is a heart attack. Not a gradual blockage. A rupture. Calcification enters later, reprogramming smooth muscle cells into osteoblasts that deposit the same mineral as bone. Microcalcifications within the cap are volatile — stress concentrators that can trigger rupture without warning. Macrocalcifications deep in the plaque act as a stabilizing splint. This is why a rising calcium score can coexist with falling cardiac risk. They describe different stages of the same process.
The Fracture That Heals Stronger
“Before I saw my results, I thought of a broken bone. A fracture heals in six weeks, strengthens over twelve, and at the fracture point becomes even stronger than the bone that never broke. What if arterial plaque is a fracture that has never been given the conditions to heal?”
Kevin Ham, MD
The fracture point of a healed bone becomes measurably stronger than the surrounding tissue. What if arterial plaque is a fracture that has never been given the conditions to heal? Osteoclast-like cells have been detected in heavily calcified lesions. Remove the conditions driving osteoblastic transformation, and the wall can resume functioning as an arterial wall. 51 studies. 9,000+ patients. The evidence for plaque regression is now robust. The question is no longer whether it happens. It is whether you create the conditions.
And here is what reversal looks like. My carotid plaque. Gone. Remodeled. In three months. Bilateral carotid IMT of 1.8 mm and 1.6 mm with visible plaque on both sides, dropping to 0.84 mm and 0.86 mm with no visible plaque detectable on ultrasound. My CT-FFR on a dominant D1 diagonal with 77 percent stenosis: improved from 0.75 to 0.80, crossing from ischemic into the normal range. LDL: 61, a 64 percent reduction. ApoB: 45. The word my physician friends used: Unbelievable!
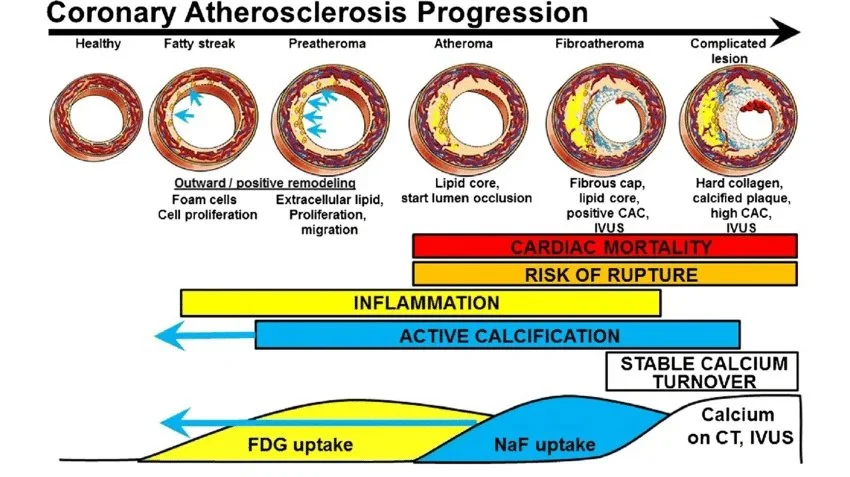
The six types of atherosclerotic plaque and their progression. My plaque is in stages 4 to 6. The later the stage, the more difficult to reverse. But not impossible. European Journal of Nuclear Medicine and Molecular Imaging, November 2018.
The Fracture That Heals Stronger
“Before I saw my results, I thought of a broken bone. A fracture heals in six weeks, strengthens over twelve, and at the fracture point becomes even stronger than the bone that never broke. What if arterial plaque is a fracture that has never been given the conditions to heal?”
Kevin Ham, MD
The fracture point of a healed bone becomes measurably stronger than the surrounding tissue. What if arterial plaque is a fracture that has never been given the conditions to heal? Osteoclast-like cells have been detected in heavily calcified lesions. Remove the conditions driving osteoblastic transformation and the wall can begin to function as arterial wall again. 51 studies. 9,000+ patients. The evidence for plaque regression is now robust. The question is no longer whether it happens. It is whether you create the conditions.
And here is what reversal looks like. My carotid plaque. Gone. Remodeled. In three months. Bilateral carotid IMT of 1.8 mm and 1.6 mm with visible plaque on both sides, dropping to 0.84 mm and 0.86 mm with no visible plaque detectable on ultrasound. My CT-FFR on a dominant D1 diagonal with 77 percent stenosis: improved from 0.75 to 0.80, crossing from ischemic into the normal range. LDL: 61, a 64 percent reduction. ApoB: 45. The word my physician friends used: Unbelievable!
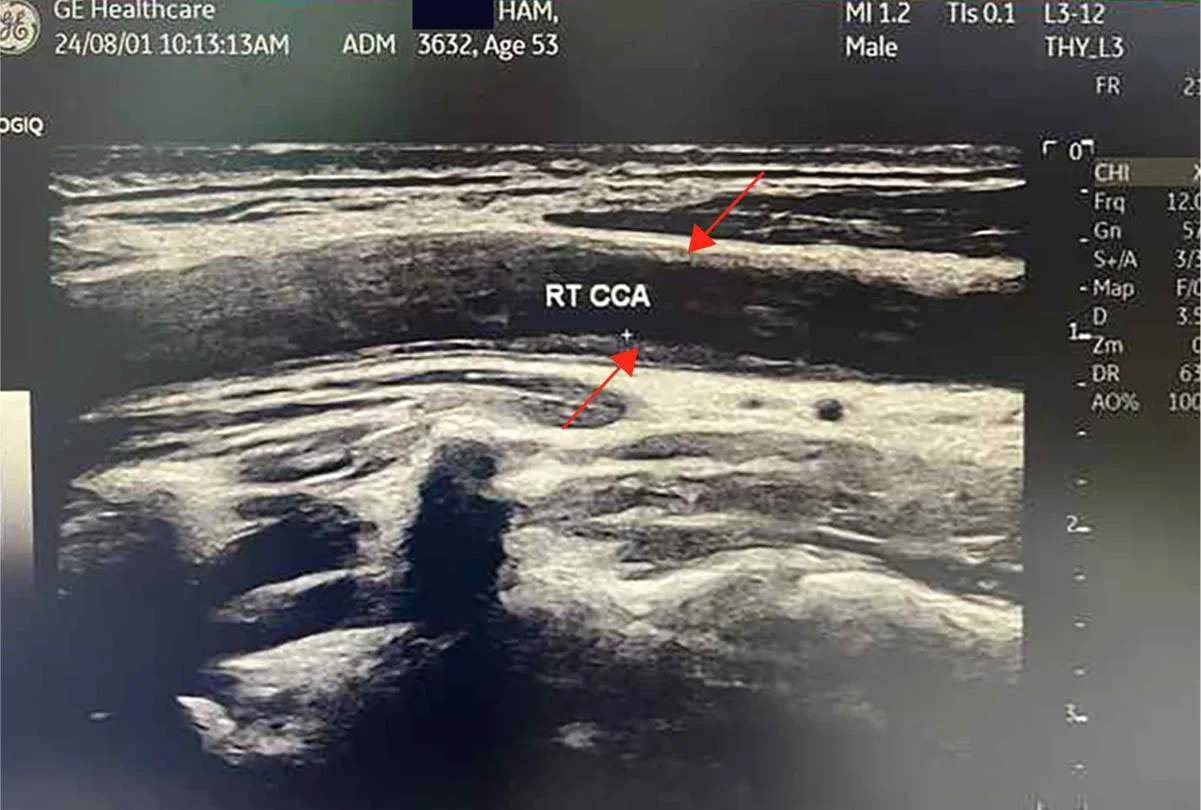
Before: RT CCA . Longitudinal . Baseline

Before: LT CCA . Longitudinal . Baseline
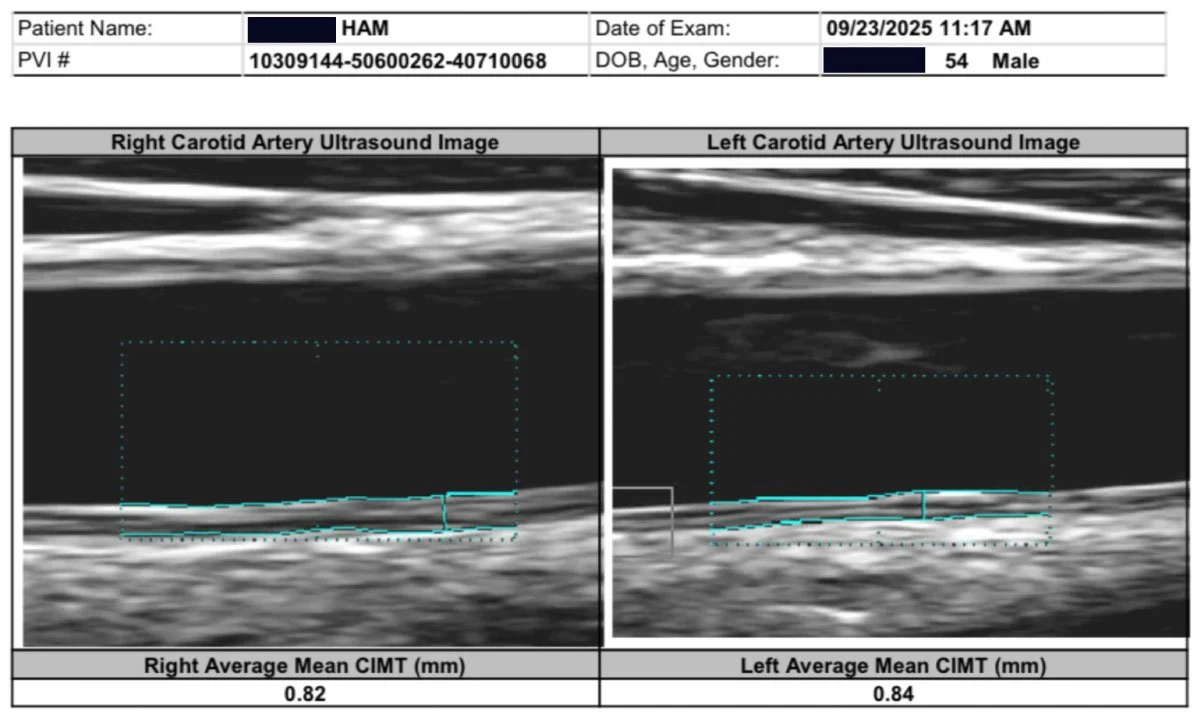
After: Plaque remodeling and reversal. B-mode ultrasound imaging of the carotid artery. Kevin Ham, MD, 2025. Three months on the CAST protocol: WFPB diet, high-intensity cycling, structured fasting, targeted supplementation.
The CAST Protocol
“Cast by removing the causes. Add the healers. Support and strengthen. Track and measure. Stop the damage, add what heals, strengthen the blood vessels, and track the results.”
Kevin Ham, MD
Four moves, in order. One sentence: stop the damage by removing the causes, add what heals, strengthen the blood vessels, and track the results.
C: Cast by Removing the Causes. Like a cast on a broken bone. Fractured arteries. Fractured endothelium. Fractured retina. Fractured health. Before any healing element can work, you must first stop the damage: processed food, oxidized lipids, sedentary life, and chronic stress. Cast it first, hold it still, and let the body begin its work.
A: Add the Healers. Healing foods that generate nitric oxide and reverse endothelial dysfunction. High-intensity exercise that drives macrophages toward the anti-inflammatory M2 phenotype. Fasting that activates autophagy and resets the immune system. These are not supplements to an otherwise unchanged life. They are the intervention.
S: Support and Strengthen. Build the three pillars as permanent lifestyle habits:
Diet. The Esselstyn whole food plant-based protocol. Total fat below 25 grams daily. No oils. No animal products. Greens six times a day, chewed thoroughly so the nitrates convert to nitric oxide, the molecule that protects your endothelium around the clock. Nattokinase at 6,000 FU. Aged garlic at 2,000 milligrams. Pomegranate juice. Curcumin. Spirulina. Algae-sourced EPA and DHA. Balsamic vinegar. A medicine cabinet made of food.
Exercise. HIIT: High Intensity Interval Training. Out-of-breath pace for 30 seconds to four minutes, then recover for 4 minutes. Repeat 1 to 4 times. Walk fast, jog, run, cycle, swim, squats, or jump rope. Whatever gets your heart rate up and blood flowing with good sheer force. This is nitric oxide-producing, artery-protecting exercise. Think of it as a good pressure wash for your arteries. High-intensity aerobic effort quiets the inflammatory fire inside the arterial wall. This is one of the most powerful prescriptions I have ever written.
Fasting. I fast to activate what 300,000 years of evolutionary biology encoded in every cell. Autophagy dismantles damaged cellular machinery. Extended fasting triggers hematopoietic stem cell activation, which gives rise to immune system precursors. My protocol: daily 16:8, one OMAD day per week, one extended fast of two to three days per month. Not asceticism. Seasonality. The ancient rhythm, reclaimed deliberately.
T: Track and Measure. Carotid IMT, CT-FFR, and coronary CT angiogram every six months. Lipid profile and metabolic profile every 30 to 45 days until you hit your targets, then every quarter. Without measurement, you are making changes into the void. Every image is a report from the front line.
Diet. Exercise. Fasting. The Ancient Flywheel.
“I am not fasting to lose weight. I am fasting to activate an ancient system of survival in our bodies. Autophagy. Stem cells. Immune cells reset. Regeneration. The power of our famine and feast seasonality.”
Kevin Ham, MD
I finally understand. Once I understood heart disease, I finally understood my eye disease. And almost all of the modern diseases of our civilization today. Including, I believe, an elementary understanding of how to begin dealing with cancer, understood as a metabolic and vascular disease with the same upstream roots.
These three levers, diet, exercise, and fasting, are not a wellness routine. They are a biological intervention targeting the upstream causes of the number one killer on earth. The protocol in the section above tells you what to take. These three pillars tell you how to live.
“The three together are not additive. They are multiplicative. A force multiplier. A flywheel that, once set in motion, compounds on itself.”
One Disease. Many Organs. One Protocol.
“I was surprised all of a sudden with wet macular degeneration. To me they are the same disease, just different organs. I am reversing both, so help me God.”
Kevin Ham, MD
I am the doctor who became the patient. And because I became the patient, I began to see what I could not see from the other side of the room.
I was diagnosed with severe wet macular degeneration in both eyes on the morning of May 10, 2020. I was only 50 years old. It announced itself suddenly: a straight line bent, vision distorted, fluid beneath the retina. Wet AMD is a disease of the 70s and 80s. I was 20 to 30 years too young for this diagnosis. Even if I lived a long life, I was told it would likely be in blindness—no cure yet known. And no one could explain why it had arrived so early. But I could. When I looked at the biology, I saw the same driving mechanism as coronary artery disease: endothelial dysfunction in the microvasculature. The same inflammatory cascade. The same oxidized lipid injury. The same nitric oxide deficiency. The retina was simply the first organ that made the disease visible. My arteries had been telling the same story for years. It is the same disease presenting in a different organ.
Wet macular degeneration. Coronary artery disease. Type 2 diabetes. Hypertension. Non-alcoholic fatty liver disease. And I believe, in due time, certain autoimmune diseases. Cancer is understood as a metabolic disease.
These are not separate diseases coexisting in the same aging body. They are expressions of one underlying condition: chronic metabolic inflammation driving endothelial dysfunction across different organ systems. Medicine treats each in a separate department, with a different specialist, and a different drug. But the root is the same root. And if the root is the same, the protocol that addresses the root addresses them all.
Circumcise Your Heart
“Circumcise yourselves to the LORD; remove the foreskin of your heart.”
Jeremiah 4:4
The command to circumcise the heart runs through Scripture like a surgical instruction. In Ezekiel 36, God promises not merely to command this change but to perform it: I will remove the heart of stone from your flesh and give you a heart of flesh. The surgery is divine. The rock does not yield on its own. It requires an instrument applied from outside the system. The same is true in biology.
The circumcision of the heart is the cutting away of what covers and hardens the living tissue underneath. The removal of the calcified layer of habit and assumption that prevents the blood of grace from flowing freely. In both dimensions, spiritual and biological, the grammar is identical: remove the cause, restore the inhibitors, allow the program of reversal to run. What was rock yields water. What was rigid becomes responsive. What was closed becomes open to flow.
Strike the rock.
“I will give you a new heart and put a new spirit within you; I will remove the heart of stone from your flesh and give you a heart of flesh.”
Ezekiel 36:26
Your Questions
Questions worth sitting with.
One action. In the next 24 hours, book a CT calcium score or a Carotid IMT ultrasound. Call your doctor today and ask for it by name. That single image will tell you more about your arterial health than every blood test you have ever had.
1. Is there someone in your life whose sudden death you would not recover from? Do they know what is building inside their arterial wall?
Rob Thompson's wife stood at his memorial and said: he had a stress test every day. Every workout, every climb. He passed everyone. And then he died. She asked every person in that room to get a CT calcium score. You can give someone you love the gift that Rob's wife was never able to give Rob. Send them this. Ten seconds
2. If 91 percent of people over 50 have measurable plaque right now, and most of them have never been told, what are the odds that you are the exception?
You are probably not the exception. Neither was Rob. Neither was I. The imaging that would tell you the truth about your arterial wall takes 30 minutes and is available in most cities. The question is not whether you can afford to find out. The question is whether you can afford not to.
3. When is the last time you ate a meal that was designed to heal your endothelium rather than injure it?
Every meal is a vote: either for the endothelium that keeps plaque from starting, or against it. Dr. Esselstyn kept the worst heart patients alive for 12 years with just diet. No surgery. No procedure. No prescription. Just food chosen deliberately. That power is available to you at the next meal.
4. If your body has the biological machinery to reverse this, what is the one thing you are willing to change today to let it begin?
Not everything. Just one thing. Today. I started the whole food plant-based diet on May 9, 2025, the morning after I saw my calcium score of 505. Within three months, my carotid plaque was gone. One meal in the right direction is the beginning of fracture healing. Start there.
Someone You Love
“The greatest single threat to the cardiac health of each individual is his own coronary arteries. And the greatest threat is not that we lack the knowledge to prevent the disease. It is that we lack the will to act on what we already know.”
Paul Dudley White, MD Presidential physician, founder of the American Heart Association, 1956
You thought of someone while reading this. Their name came to you. Maybe it is the person who has never had arterial imaging. Maybe it is the one who was told their cholesterol is fine and sent home with nothing else. Maybe it is you. Rob Thompson passed every stress test he ever took. His LDL was normal. And on February 10, 2025, he died of a process that had been building for forty years inside a wall that no standard test was looking at. The gift Rob's wife never got to give him takes ten seconds to send.
This is my ministry. This is my gospel of your heart.Send this to the person you thought of. Better late than never.
Strike the rock. I pray that the rock yields its waters for you.
MORE READINGS YOU’LL ENJOY
Health
Watch: The 2 Foods That Reverse Heart Plaque (Half a Million Views)
Reversing My 77% Heart Plaques
Stats Say You Likely Have Heart Plaque
The Healing Power of Food: Nitric Oxide
Wealth
The Power of the Compound Effect
Relentless Iteration to Mastery
Meaning
The Courage to Your Magnum Opus
APPENDIX
The ten studies that anchor the science in this newsletter.
1. Esselstyn CB Jr, et al. A Strategy to Arrest and Reverse Coronary Artery Disease: A 5-Year Longitudinal Study. J Fam Pract. 1995;41:560-568.
The foundational study. Severe coronary disease arrested and reversed in human patients through plant-based diet alone. The study medicine still does not know what to do with.
"Heart disease isn't some great mystery. We are empowered to take control of it. Patients are often furious that they were not made aware of this option earlier." — Caldwell B. Esselstyn Jr., MD
2. Esselstyn CB Jr. Updating a 12-Year Experience With Arrest and Reversal Therapy for Coronary Heart Disease. Am J Cardiol. 1999;84:339-341.
Twelve-year follow-up of the original 24-patient cohort: one cardiac event among adherent patients versus thirteen among those who returned to standard care.
"Coronary artery disease need not exist, and if it does exist, it need not progress. We have documented not merely the arrest but the reversal of this disease in human beings." — Caldwell B. Esselstyn Jr., MD
3. Ihle-Hansen H, et al. Prevalence of Carotid Plaque in a 63 to 65-Year-Old Norwegian Cohort: The ACE 1950 Study. J Am Heart Assoc. 2018;7:e008562.
Carotid ultrasound of 3,683 generally healthy adults: plaque in 87 percent overall, 92 percent of men. The 91 percent figure cited in this newsletter.
"Atherosclerotic carotid plaques were present in 87% of the participants. The carotid plaque score was more strongly associated with incident ischemic stroke than established cardiovascular risk scores." — Ihle-Hansen H, et al.
4. Enos WF, Holmes RH, Beyer J. Coronary disease among United States soldiers killed in action in Korea. JAMA. 1953;158:912-914.
Autopsies of 300 soldiers, average age 22. Gross atherosclerosis in 77.3 percent. The study that should have tipped in 1953 and did not.
"Gross evidence of coronary arteriosclerosis was found in 77.3 percent of 300 American soldiers killed in Korea, average age 22. It is no wonder that at the time of death the process was far advanced." — Enos WF, Holmes RH, Beyer J.
5. Han D, Torii S, et al. Quantitative measurement of lipid rich plaque: correlation of histology in sudden cardiac death. Atherosclerosis. 2018;275:426-433.
Post-mortem CT correlation with histology in sudden cardiac death hearts: mean ruptured lipid-rich plaque area of 0.34 square millimeters. A whisper of tissue. Sufficient to kill.
"Mean lipid-rich plaque area per coronary cross-section in sudden cardiac death hearts: 0.34 square millimeters. A whisper of vulnerable tissue sufficient to kill." — Han D, Torii S, et al.
6. Williams MC, et al. Low-Attenuation Noncalcified Plaque Predicts Myocardial Infarction: SCOT-HEART Trial. Circulation. 2020;141:1452-1462.
1,769 patients followed for nearly five years. Low-attenuation plaque burden outperformed every other predictor of heart attack: better than calcium score, risk scores, and stenosis severity combined.
"An increased burden of low-attenuation plaque is the principal predictor of increased coronary events, above and beyond other established classic markers of cardiovascular risk." — Williams MC, et al.
7. Schurgers LJ, Cranenburg ECM, Vermeer C. Matrix Gla-protein: the calcification inhibitor in need of vitamin K. Thromb Haemost. 2008;100:593-603.
Established Matrix Gla Protein, activated by vitamin K2, as the dominant inhibitor of arterial calcification. High vitamin K intake not only prevents but regresses existing vascular calcium.
"There seems to be no effective alternative mechanism for calcification inhibition in the vasculature. High vitamin K intake not only prevents calcification, but even regresses arterial calcifications." — Leon J. Schurgers, PhD
8. Xu Z, et al. Osteoclastogenesis and Osteoblastogenesis in Vascular Calcification. Front Cardiovasc Med. 2021;8:639740.
Demonstrated that arterial calcification is reversible: osteoclast-like cells can resorb mineral from the arterial wall, establishing the cellular basis for the reversal documented in this newsletter.
"Arterial calcification is a cell-mediated, reversible and actively regulated process. Tilting the balance toward osteoclast-like cells may be a promising therapeutic strategy." — Xu Z, et al.
9. Banach M, et al. Atherosclerotic coronary plaque regression from lipid-lowering therapies: a meta-analysis. Atherosclerosis Plus. 2024.
Meta-analysis of 51 studies and 9,113 patients. Plaque regression is real, reproducible, and documented. The question is no longer whether it happens. It is how aggressively we pursue it.
"The evidence for plaque regression is now robust. The question is no longer whether plaque regresses, but how aggressively we pursue the conditions that allow it." — Banach M, et al.
10. Longo VD, Mattson MP. Fasting: molecular mechanisms and clinical applications. Cell Metab. 2014;19:181-192.
The molecular mechanism review behind the fasting component of the CAST protocol: autophagy, apoptosis of damaged cells, and stem cell activation. The most extensive cellular renewal process available to the human body.
"During prolonged fasting, the body survives by eliminating unnecessary cells. These cells will be replaced when food becomes available. This regeneration process, the most extensive since birth, is a powerful feature of prolonged fasting." — Valter D. Longo, PhD
I pray you unlock your heart to reach the height of your full potential by discovering your calling.
Kevin Ham, MD
Subscribe to my Compounding Wisdom newsletter and start transforming your life. ham.com
Subscribe to my YouTube channel @DrKevinHamfor videos on how I reversed my clogged arteries in 3 months, the top foods that clear your arteries, and the first principles of health that can save your life. Like, share and subscribe — it could save the life of someone you love.
Reversing the Disease Flywheel
First Principles on Reversing the Biology of Disease
First Principles on Reversing the Biology of Disease
Dr. Kevin Ham, MD
The Architecture of a Cure
“Some people think that the plant-based, whole foods diet is extreme. Half a million people a year will have their chests opened up and a vein taken from their leg and sewn onto their coronary artery. Some people would call that extreme.”
Caldwell Esselstyn Jr., MD. Cleveland Clinic.
I am a physician turned entrepreneur. Twenty-five years of building companies taught me mental models that have nothing to do with balance sheets and everything to do with how complex systems actually work. When my heart scan came back, I did what I always do when I do not know something. I studied. I studied the data, the mechanistic pathways, the constraints and the 80/20 levers. And I applied the same four principles to heart disease that I have used in business. This is the methodology behind my results.
Principle 1: The Flywheel
“The flywheel effect is not the result of one defining action, one grand program, one killer innovation, one solitary lucky break. It comes from the cumulative effect of pushing the flywheel forward, turn after turn, building momentum until a point of breakthrough and beyond.”
Jim Collins. Good to Great.
A flywheel is a rotating mass that stores momentum. In physics, it is the heavy disc on an engine that keeps the crankshaft turning smoothly between combustion strokes. The critical property of a flywheel is this: it resists change in both directions. It is hard to accelerate from rest. But once it is spinning, it is equally hard to stop.
Disease is a flywheel. Not a sudden event. Not bad luck. A self-reinforcing vicious cycle that builds speed over the course of many years, each revolution making the next one faster and harder to interrupt. Endothelial damage invites oxidized LDL. Oxidized LDL triggers inflammation. Inflammation damages the endothelium further. The cycle closes, tightens, and accelerates. This is the vicious flywheel, running in the dark for decades before it announces itself.
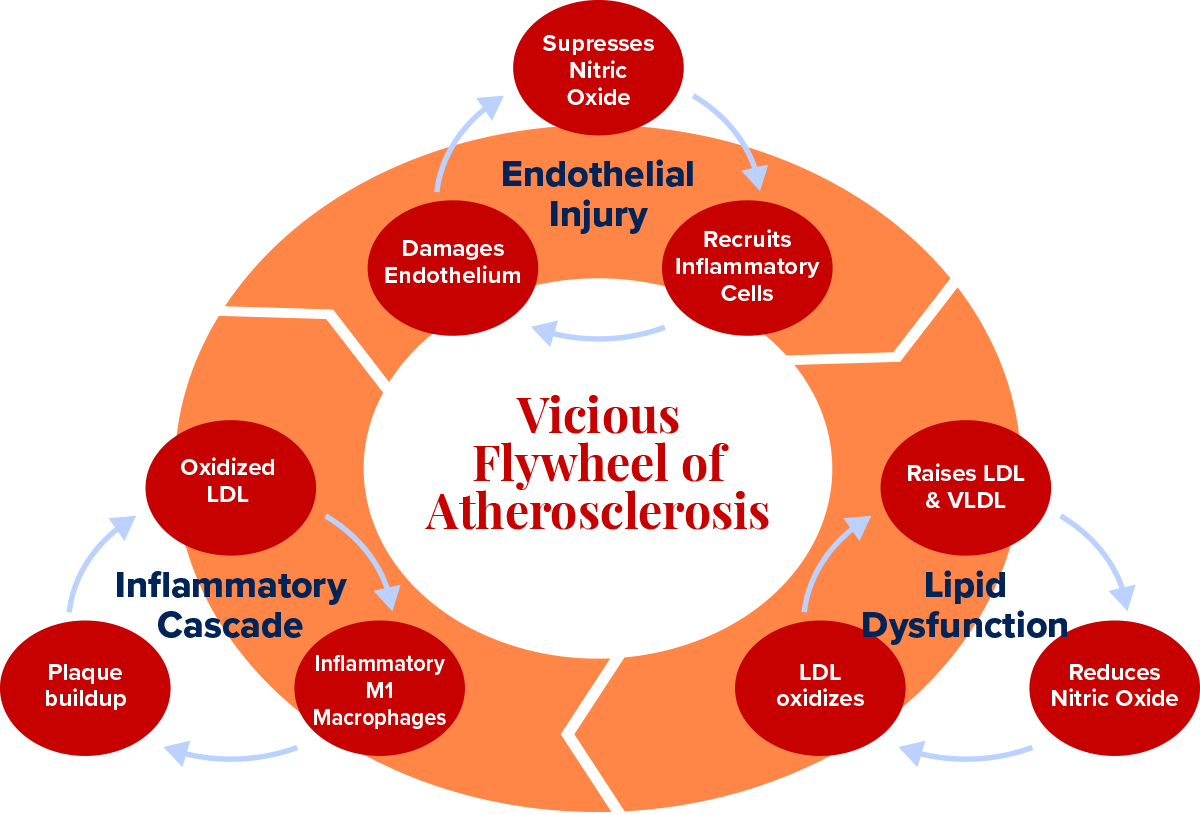
Health is also a flywheel, turning in the right direction. A healthy endothelium produces nitric oxide. Nitric oxide blocks LDL oxidation and suppresses the adhesion molecules that recruit inflammatory cells. With less inflammation, the endothelium can repair itself. A repaired endothelium produces more nitric oxide. Each revolution reinforces the next. This is the virtuous flywheel.
The central question of my protocol is not: what supplements should I take? It is: how do I stop the vicious flywheel and start the virtuous one? Because the biology of the flywheel tells you something important. You do not need to fix everything simultaneously. You need sufficient force, applied at the right entry point, and the system will do the rest. Get the flywheel turning in the right direction, and it gains its own momentum.
Principle 2: The Judo Strategy
“The goal of judo is not to defeat your opponent. It is to understand the principles of life itself. Maximum efficiency with minimum effort. Mutual welfare and benefit. Yield to win.”
Jigoro Kano. Founder of Kodokan Judo. 1882.
In judo, strength is irrelevant. The principle is leverage: you use your opponent’s own force against them. When they push, you pull in the same direction, adding your force to theirs, and suddenly their own momentum carries them off balance. Then you use your body as a lever, redirect the energy, and throw them with a fraction of the effort it would take in a direct confrontation. When they pull, you push, and the same geometry applies. The opponent’s strength becomes your weapon.
I apply this to disease with one question: what forces is the disease already using, and how do I redirect them? In atherosclerosis, the immune system recruits macrophages into the arterial wall to clear oxidized LDL. In a chronically inflamed environment, those macrophages become overloaded, switch to a destructive M1 phenotype, and begin releasing enzymes that digest the fibrous cap of existing plaque from within. The very system designed to protect you is now accelerating your destruction.
The judo move is not to suppress the immune system. It is to shift the macrophage phenotype from M1 to M2, from inflammatory to healing, so that the same cells that were building disease begin participating in its reversal. Polyphenols, exercise, and fasting all apply force at this exact switch. You are not fighting your immune system. You are redirecting it. The opposition’s strength becomes your treatment.
Principle 3: The Fractal 80/20
“The 80/20 principle says that a minority of causes, inputs or effort usually leads to a majority of results, outputs or rewards. Taken to its logical conclusion, it means that a great deal of what we do is of low value and a little of what we do is of high value. The more we can concentrate on the high-value activities, the more effective we become.”
Richard Koch. The 80/20 Principle.
Vilfredo Pareto noticed in 1896 that 20 percent of the peapods in his garden produced 80 percent of the peas. The same ratio appeared in land ownership across Italy. Economists found it in income distribution. Engineers found it in software defects. Athletes find it in training adaptation. The specific numbers vary. The underlying principle does not: inputs are not created equal. A small number of causes drive the vast majority of effects.
In medicine, this means that among the hundreds of factors that might contribute to your cardiovascular disease, roughly 20 are responsible for 80 percent of what is happening. The other 80 contribute the remaining 20 percent. If you pursue all of them with equal effort, you are dramatically misallocating your time and energy. The 80/20 principle is not an excuse for laziness. It is a demand for precision. Find the 20 that matter most and address those first.
But here is where it becomes remarkable, and where most people stop too soon: the 80/20 principle is fractal. It repeats inside itself, at every level of magnification, like a coastline that shows the same jagged complexity whether you view it from a satellite or from a clifftop or from your knees in the sand.
Take those top 20 factors, the ones producing 80 percent of your disease. Apply the 80/20 lens to that group alone. Twenty percent of those 20 factors, which is 4 factors, will produce 80 percent of that 80 percent of results. Run the arithmetic: 4 things account for 64 percent of your total disease burden. You have gone from 100 inputs to 4 and captured nearly two-thirds of the problem.
Apply the fractal one more time. Of those 4 high-leverage factors, one accounts for 80 percent of that 64 percent. Which means: one single factor accounts for roughly 51 percent of the total. One thing. Half the problem. If you can identify it and remove it, you have done more than any other single intervention could possibly achieve. This is not a shortcut. It is the highest form of strategic thinking: the relentless reduction of complexity until the single most powerful lever is visible.
In cardiovascular disease, that one thing is endothelial dysfunction. The endothelium is the initiating event. It is the gate that, when compromised, lets the Trojan horse through. It is the surface that, when inflamed, becomes a magnet for plaque formation. It is the organ that, when healthy, produces nitric oxide, which prevents nearly every downstream step in the cascade.
Heal the endothelium, and you have addressed 51 percent of the disease through a single biological mechanism. Every other intervention in my protocol is downstream of this one.
Find the one thing.
In disease: it is the cause. Remove the cause and you remove half the disease.
In health: it is the highest-leverage intervention. Find it and you gain half the results.
The fractal 80/20 is not a formula. It is a philosophy of precision.
Principle 4: The Theory of Constraints
“An hour lost at a bottleneck is an hour lost for the entire system. An hour saved at a non-bottleneck is a mirage. It saves nothing. It changes nothing. Only the constraint matters.”
Eliyahu Goldratt, PhD. The Goal.
Eliyahu Goldratt introduced this framework in manufacturing. Every production system has a bottleneck, a single point that limits the throughput of the entire process more than any other. You can optimize every other step to perfection, but if the bottleneck remains, overall output does not improve. The constraint governs everything. The only productive action is to find it, elevate it, and then look for the next constraint.
In cardiovascular disease, the bottleneck is blood flow. Specifically, its interruption. Heart attacks occur when a clot or a ruptured plaque causes sudden, complete obstruction of a coronary artery. Strokes occur when the same happens in cerebral circulation or when a vessel ruptures. The common thread is not the size of the blockage. It is the stability of the plaque and the thrombogenicity of its contents. A 90 percent stenosis with a thick fibrous cap and a quiescent inflammatory environment may never rupture. A 30 percent stenosis with a thin cap and an activated immune infiltrate can kill you on a Tuesday morning.
The constraint in heart disease is not cholesterol. It is not even stenosis percentage. The constraint is the biology that makes a plaque vulnerable to rupture: inflammation, a thin fibrous cap, a large necrotic core, and the matrix metalloproteinases produced by M1 macrophages that digest the cap from within. Remove that constraint, and you remove the mechanism of the acute event, regardless of what is on your lipid panel.
These four principles are not independent ideas. They are a single system of thought.
The flywheel gives you the architecture of disease and health.
The judo strategy tells you how to redirect the disease’s own forces.
The fractal 80/20 tells you where to apply force first.
The theory of constraints tells you what to remove.
Together, they produced my protocol. And together they produced my results.
“Atherosclerosis is not a lipid storage disease. It is a chronic inflammatory disease of the arterial wall, initiated by injury to the endothelium.”
“Atherosclerosis is not a lipid storage disease. It is a chronic inflammatory disease of the arterial wall, initiated by injury to the endothelium.”
Russell Ross, MD. University of Washington. New England Journal of Medicine, 1999.
Your Blood Vessel Wall is Already Burning
“The lesion of atherosclerosis is the most common cause of death in Western societies. It is also, in principle, preventable. It begins not with cholesterol, but with injury. Remove the injury and you remove the disease.”
Russell Ross. New England Journal of Medicine, 1999.
Most people, when they think about heart disease, think about cholesterol. But cholesterol is an ingredient of plaque, not the cause. Think of the arterial wall as a fortified city. The endothelium is the city wall, the sentinel layer. If the wall is intact, the city is defended. When it is damaged, the Trojan horse gets through.
The man who proved this was Russell Ross, a pathologist at the University of Washington, working in 1973 on what most of his colleagues considered a settled question. Atherosclerosis, the prevailing view held, was essentially a passive process: cholesterol circulating in excess would simply seep through vessel walls and accumulate, like sediment settling at the bottom of a river. Ross did not believe it. He had been studying platelet-derived growth factor and noticed something that did not fit the sediment theory: the arterial lesions he was examining looked less like passive deposits and more like wound responses. The tissue was reacting. The wall was responding to something.
He published what he called the ‘response to injury’ hypothesis in 1973 and expanded it through two subsequent decades of work. The injury he meant was not a cut or a bruise. It was a molecular insult to the endothelium: the inner lining of the blood vessel, a structure so thin it had largely been treated as irrelevant scaffolding. Ross proposed that this single-cell layer was not passive scaffolding at all. It was an active, signalling, immunological frontier. Damage it, and you initiate a cascade that looks far more like chronic inflammation than passive lipid deposition. The medical establishment received this idea with the same generous skepticism it reserves for all ideas that require reconsidering everything. But Ross was right. And the cascade he described is the vicious flywheel.
The Trojan horse is LDL cholesterol. Once inside the damaged wall, LDL can oxidize. Oxidized LDL is a danger signal that summons the immune system. Monocytes flood in and become macrophages, tasked with cleaning up the mess. But in a chronically inflamed environment, they become overwhelmed. They shift to the M1 inflammatory phenotype, releasing cytokines that further damage the endothelium, allowing more LDL through, driving more oxidation, and recruiting more monocytes. The macrophages die, full of lipids, forming foam cells and the necrotic core of the growing plaque. And the cycle accelerates.
This flywheel runs on three pillars, each driving the next. Endothelial damage is where it begins:
saturated fat suppresses eNOS within hours of consumption,
hypertension shears the vessel wall at arterial branch points, and
oxidative stress depletes the antioxidant defences that protect the inner lining.
When the wall fails, LDL slips through. Once inside, in the changed chemical environment of the subendothelial space, it oxidizes. Oxidized LDL is a danger signal. It summons the immune system.
That summoning is the second pillar: chronic inflammation.
Monocytes migrate into the wall and become macrophages, tasked with neutralizing the oxidized LDL. In an acute situation, this works. In a chronic one, it fails catastrophically. The macrophages become overwhelmed, switch to the M1 inflammatory phenotype, and begin releasing cytokines, IL-6, TNF-alpha, and matrix metalloproteinases that dissolve the fibrous cap protecting the growing plaque from the bloodstream. They recruit more monocytes. More monocytes damage the endothelium further. The gate opens wider.
The third pillar is atherogenic lipoproteins, and the most important measure here is not LDL cholesterol but ApoB: one molecule per particle, present on every atherogenic lipoprotein in circulation, a direct count of the Trojan horses circling the arterial wall.
Saturated fat downregulates the hepatic receptors that clear these particles.
Insulin resistance drives the liver to overproduce VLDL.
The oxidized form of these particles, once inside the inflamed wall, is the direct trigger of the foam cell cascade that forms the necrotic core of plaque.
The most dangerous heart attack is not caused by the most obstructed artery. This shattered my prior intuition. The most dangerous lesion is a vulnerable plaque: a small to medium deposit with a large necrotic core, a thin fibrous cap, and a crown of activated M1 macrophages digesting the cap from within. When that cap ruptures, the contents contact circulating blood and trigger the explosive thrombosis that produces a heart attack within minutes. The most dangerous plaques are the most inflamed, not the largest.
The disease has been running its program for forty years. The flywheel is already spinning. The question is not whether it has started. The question is whether you will stop it.
“Our genes are not our fate. Even older adults with severe coronary artery disease can begin to reverse it. Not slow it. Reverse it. Within weeks, most patients feel so much better, so quickly, that these new behaviours become sustainable.”
Dean Ornish, MD. Lifestyle Heart Trial. The Lancet, 1990.
The Disease that Reverses
“Joy is a more powerful motivator than fear. In my experience, most people don't want to be told what to stop doing. They want to be told what they can start doing that will make them feel better right away.”
Dean Ornish’ Program for Reversing Heart Disease, 1990.
In the late 1980s, a young physician named Dean Ornish proposed something that the cardiological establishment found almost impolite. He wanted to know whether coronary artery disease could be reversed, not slowed, not stabilized, but actually reversed, through diet, exercise, stress management, and group support alone. No drugs. No surgery. No stents. The proposal drew skepticism that ranged from condescension to amusement. Coronary artery disease was a one-way street. Everyone knew that. Ornish apparently did not.
He ran the Lifestyle Heart Trial anyway. Twenty-eight patients with documented coronary artery disease were randomized to his intensive program. Twenty patients served as controls. Coronary angiography was performed at baseline and at one year, measuring the actual diameter of the coronary arteries, the same vessels in which plaque had been growing for decades. The results, published in The Lancet in 1990, were unambiguous: in the treatment group, arteries had grown wider. In the control group, following standard American Heart Association guidelines, they had continued to narrow. At five years, the divergence had increased. The patients who had reversed their disease most completely were the ones who had followed the protocol most strictly. The lifestyle intervention was dose-dependent, like a drug, except it had no patent and no sales force and required no prescription.
The medical community acknowledged the data and largely declined to change its practice. The mechanisms were not yet understood. The trial was small. The diet was extreme. These were the arguments. What they amounted to was: we believe you, but we are not ready to believe you. What Ornish had found, though neither he nor his contemporaries could fully name it in 1990, was the virtuous flywheel. Apply enough force at the right entry points, and the biology reverses its own direction.
The virtuous flywheel has the same architecture as the vicious one, but the direction of causation reverses. The three pillars now amplify healing instead of disease. I experienced this in three months. My carotid plaque: gone. My LDL is down 64%. My ApoB at 45. My D1 CT-FFR improved from 0.75 to 0.80, moving from functionally significant stenosis into the low-normal range. The virtuous flywheel is turning.
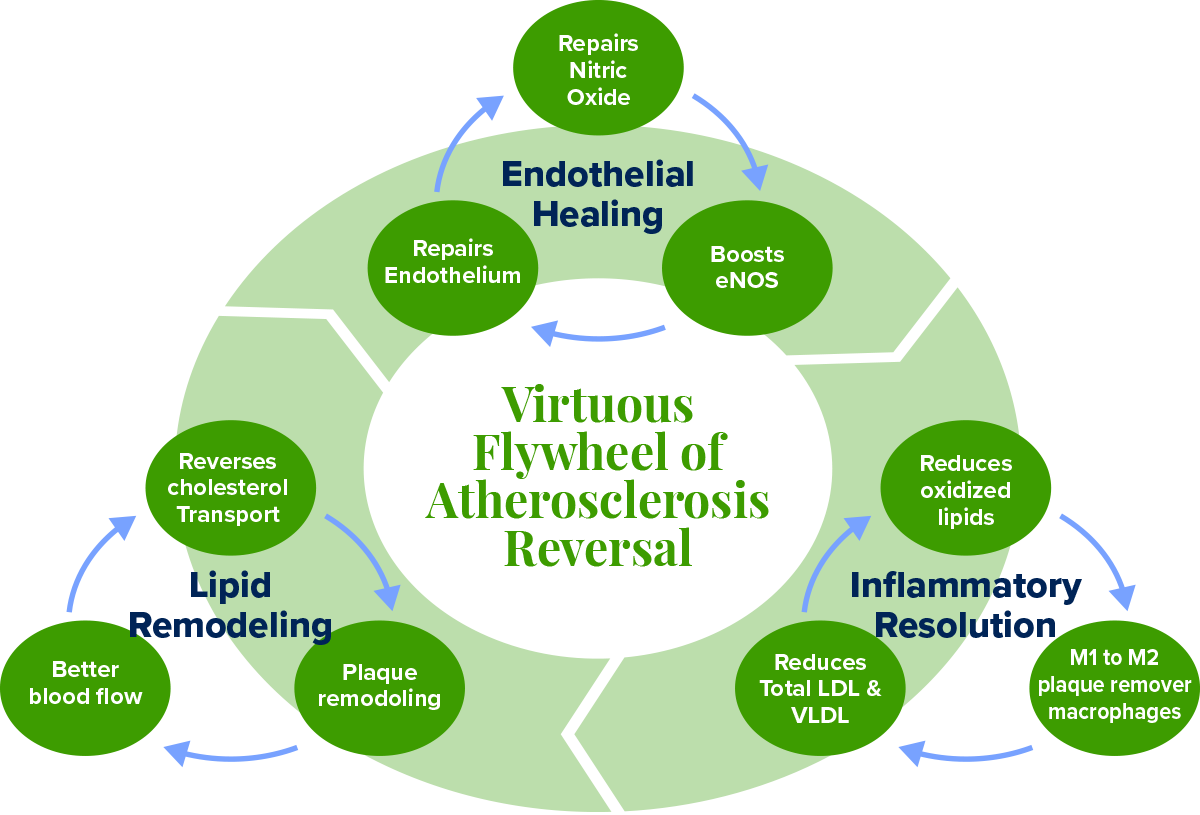
Figure 1. The Virtuous Flywheel of Atherosclerosis Reversal, running clockwise from Endothelial Healing through Lipid Remodeling to Inflammation Resolution. Each master node contains its own three-part sub-cycle.
1. Endothelial Healing. The endothelium does not heal passively. It heals through nitric oxide production, eNOS activation, and endothelial progenitor cell repair. These three mechanisms form their own sub-cycle:
Nitric oxide relaxes the vessel wall and reduces shear-induced injury;
Reduced injury preserves eNOS coupling so it produces more nitric oxide rather than superoxide;
More nitric oxide mobilizes bone-marrow endothelial progenitor cells that replace dead cells and close the breach.
Exercise upregulates eNOS through pulsatile blood flow.
Dietary nitrates from leafy greens feed the oral-gastric pathway, an eNOS-independent route to nitric oxide that works all day as long as you keep eating greens.
Deep sleep pulses growth hormone that drives progenitor cell mobilization overnight.
2. Lipid Remodelling. The right target is not LDL-C but ApoB: the count of every atherogenic particle capable of entering the arterial wall. And the real goal is not merely reducing entry but activating reverse cholesterol transport (RCT): the ABCA1-mediated extraction of cholesterol from foam cells inside the plaque, loaded onto HDL particles, returned to the liver for excretion. This is the mechanism of plaque regression.
Eliminating saturated fat upregulates hepatic LDL receptors.
Exercise activates lipoprotein lipase and improves HDL function.
Intermittent fasting reduces intrahepatic fat and VLDL overproduction.
When efflux exceeds influx, the necrotic core shrinks, and the fibrous cap thickens.
Two upstream drivers of this node are almost never discussed in standard cardiology.
The first is HbA1c. Hyperglycemia glycates LDL particles, and glycated LDL is taken up by macrophages at a far higher rate than native LDL, accelerating foam cell formation regardless of your ApoB count. It also generates advanced glycation end products that cross-link collagen in the arterial wall, stiffening it and making the endothelium less responsive to nitric oxide. Insulin resistance simultaneously drives hepatic VLDL overproduction, directly raising ApoB burden. Target HbA1c for cardiovascular protection is below 5.4%, well below the conventional pre-diabetes threshold of 5.7.
The whole food plant-based diet and
16:8 fasting are the two most powerful interventions.
The post-meal walk serves the same purpose acutely, clearing glucose from circulation before it can glycate anything.
The second overlooked driver is Vitamin K2 (MK-7).
Without sufficient K2, calcium that circulates in the bloodstream deposits into arterial walls and inside existing plaque, hardening the necrotic core and converting soft, potentially reversible plaque into fixed calcified lesions. K2 activates Matrix Gla Protein (MGP), the most potent known inhibitor of vascular calcification, which redirects that calcium back into bone instead. The Rotterdam Study demonstrated that K2 specifically, not K1, significantly reduced cardiovascular mortality and aortic calcification. The natto I already eat as an MK-7 source does double duty: the nattokinase degrades fibrin and the K2 inhibits calcification. These are distinct mechanisms from the same food, and worth tracking separately in any serious protocol.
3. Inflammation Resolution. The CANTOS trial proved that targeting inflammation alone, with no lipid lowering whatsoever, reduced major cardiovascular events by 15%. This is co-primary biology. The judo move is to shift macrophages from the M1 (inflammatory, cap-degrading) phenotype to the M2 (healing, collagen-depositing) phenotype.
Curcumin suppresses NF-kB and drives M2 polarization.
EGCG from high-catechin green tea reduces foam cell formation.
Ellagitannins from pomegranate juice upregulate ABCA1 expression in macrophages, directly increasing their capacity for cholesterol efflux.
Exercise myokines shift the immune environment toward M2.
Intermittent fasting activates autophagy to clear permanently inflamed senescent macrophages that no diet can repolarize.
The direct blood readout of this node is hs-CRP. High-sensitivity C-reactive protein is produced by the liver in response to IL-6, which is secreted by activated M1 macrophages and visceral adipose tissue. It is the most accessible systemic signal of whether your inflammatory node is moving in the right direction. Target is below 1.0 mg/L for optimal cardiovascular protection. Your polyphenol stack, your HIIT sessions, and your fasting protocol all suppress IL-6 at the source, and hs-CRP should track downward as a consequence. I measure it quarterly alongside ApoB and HbA1c as the three primary biomarker proxies for flywheel direction.
“Nitric oxide is arguably the most important molecule in the cardiovascular system. It is the endothelium’s primary defence against virtually every step in the development of atherosclerosis. You want more of it. Almost everything about modern life gives you less.”
Louis J. Ignarro, PhD. Nobel Laureate in Physiology or Medicine, 1998.
The Polluted Gas is Your Saviour
“I spent my career studying a gas that everyone assumed was just a pollutant. It turned out to be the most important signaling molecule the body makes. The lesson is: never assume you know what something is before you study it.”
Louis Ignarro, PhD. Nobel Laureate, 1998.
In 1980, before statin drugs were approved in 1987, a pharmacologist named Robert Furchgott was running experiments on strips of rabbit aorta in his laboratory at the State University of New York. He was studying how the blood vessel relaxed in response to acetylcholine, a signalling molecule that, according to the textbooks, should cause smooth muscle to dilate. It did. Except that sometimes it did not. Sometimes it caused contraction instead. Furchgott could not account for the inconsistency, and inconsistency in a careful scientist’s data is not noise to be discarded. It is a signal to be followed.
He eventually traced the discrepancy to a preparation error. When his laboratory assistants accidentally scraped the inner surface of the aorta during dissection, stripping away the single-cell endothelial lining, the acetylcholine caused contraction. When the endothelium was intact, it caused relaxation. The endothelium, he concluded, was producing something: a chemical messenger that told the smooth muscle underneath it to relax and let blood flow freely. He had no idea what it was. He called it EDRF: Endothelium-Derived Relaxing Factor. The name was a placeholder for a mystery.
It took seven more years to solve it. Louis Ignarro in California and Ferid Murad in Texas, working independently and sometimes in competition, converged on the same answer: EDRF was nitric oxide. A gas. A molecule of one nitrogen atom and one oxygen atom. In the brain, it acts as a neurotransmitter, in the immune system, it can kill cancer cells, and in the blood vessels, it can dilate them and prevent platelet aggregation and plaques.
At the time, nitric oxide was known primarily as an atmospheric pollutant and a component of smog. The idea that the human body was producing it deliberately, in the precise inner lining of every blood vessel, and using it to regulate blood flow, prevent clotting, suppress inflammation, and protect the arterial wall from disease, was received as implausible. It was implausible in the way that the best biological discoveries always are: it seemed impossible until the moment it seemed obvious. In 1998, Furchgott, Ignarro, and Murad shared the Nobel Prize in Physiology or Medicine. The molecule they had discovered was not a drug. It was a birthright. And most people are running chronically deficient in it because of what they eat.
I sat across from Dr. Caldwell B. Esselstyn Jr. on a Zoom call two weeks ago. 92 years old. Sharp as a blade. He had reversed heart disease in patients so severe they could not shave without triggering angina. His oldest patient, Stanley, came to him at age 87 on his last days of life due to severe heart disease requiring a bypass which would most likely end his life, changed to the Esselstyn diet protocol. Stanley called him at 103 to say thank you. Esselstyn leaned forward into the screen and said four words that reorganized everything I thought I knew about diet: “You need to revive your endothelium. There is an enzyme in the endothelial cells called eNOS, endothelial nitric oxide synthase, that produces nitric oxide. This is the miracle gas that will revive your endothelium.”
The pathway is simpler than any drug. Leafy greens carry dietary nitrates. The bacteria in your mouth convert those nitrates to nitrites. Stomach acid converts nitrites to nitric oxide, the same molecule your endothelium desperately needs, delivered directly to your circulation for hours after every meal. This is why Dr. Esselstyn prescribes greens six times daily, balsamic vinegar to amplify the conversion, and the removal of antiseptic mouthwash and antacids, both of which destroy the biological machinery that runs this pathway. “So your blood vessels are anointed with nitric oxide all day long.” Say YES to NO (nitric oxide). It is the simplest, most powerful cardiovascular intervention available to you today, and it requires no prescription.
“We have been measuring the wrong things. Cholesterol is the fuel. Inflammation is the fire. You can reduce the fuel all you want, but if the fire is still burning, the house still burns down.”
Paul Ridker, MD. Brigham and Women’s Hospital.
My Health Reversal Flywheel
“The doctor of the future will give no medicine, but will interest patients in the care of the human frame, in diet, and in the cause and prevention of disease.”
Thomas Edison, 1903. He was 123 years early.
I want to be specific, because the gap between principle and practice is where most protocols fail. So here is exactly what I do, and why each piece is there.
Diet is the foundation, and I follow Dr. Esselstyn’s whole food plant-based protocol without modification:
No saturated fats, which removes the primary dietary suppressor of eNOS and the main driver of ApoB particle production.
Leafy greens six times daily, boiled briefly and eaten with balsamic vinegar or lemon juice, which fuels the oral-gastric nitrate pathway continuously throughout the day.
50 millilitres of pomegranate juice with each meal, for the ellagitannins that upregulate ABCA1 in macrophages and directly support reverse cholesterol transport.
No antiseptic mouthwash, no antacids, because both destroy the biological machinery, the oral bacteria and gastric acid, that converts dietary nitrates into nitric oxide.
15-30 minute walk after each meal to activate lipoprotein lipase before triglyceride-rich particles can oxidize and reduce post-meal glucose spikes.
Exercise is non-negotiable and irreplaceable. I do HIIT three times weekly at 60 to 80 percent of my maximum heart rate for at least 1 hour. I keep the 4 x 4 minute High Intensity protocol in mind, but I do this for three reps up hills on my bicycle. I often wonder exactly what is happening to the blood flow and my heart blockages every time I go up that hill during these efforts. Theoretically, I know they are helping, but I often wonder.
This is not aesthetics. Pulsatile blood flow during sustained aerobic work is the most potent physiological stimulus for eNOS upregulation that exists. A single bout measurably improves endothelial function within hours. Sustained over months,
it upregulates eNOS expression,
mobilizes endothelial progenitor cells from bone marrow,
produces M2-polarizing myokines, and
improves both LDL receptor activity and
lipoprotein lipase-mediated triglyceride clearance.
No drug achieves this breadth of mechanism simultaneously.
I fast 16 hours daily, eating within an 8-hour window. This is not primarily about weight.
Fasting suppresses mTOR, the molecular driver of the M1 inflammatory macrophage phenotype.
It activates autophagy, the cellular recycling process that clears the senescent, permanently inflamed macrophages that no dietary intervention can repolarize.
It reduces intrahepatic fat, the primary driver of VLDL overproduction, and
reliably lowers fasting triglycerides.
Combined with the dietary protocol, it shifts the entire lipoprotein landscape.
Sleep is my acknowledged weak point, and I am correcting it. During slow-wave sleep, the pituitary releases growth hormone in pulses that drive endothelial progenitor cell mobilization. Every night of disrupted sleep is a night without the repair crew. I optimize for deep sleep duration before any other sleep metric.
My supplement stack is built around mechanism, not marketing. Every item has a specific address in the flywheel:
Nattokinase 6,000 FU: fibrin degradation, microvascular flow, thrombotic risk reduction
Aged garlic extract 2,000mg: most human-trial-validated natural agent for endothelial function and eNOS support
Algae-derived EPA and DHA: ABCA1 upregulation, M2 macrophage polarization, no oxidized fat burden of fish oil
Curcumin: direct NF-κB inhibition, M1-to-M2 macrophage shift
Vitamin C 1 to 3g daily: nitric oxide stabilization, antioxidant protection of eNOS coupling
Spirulina: phycocyanin for eNOS upregulation and anti-inflammatory activity
From natto and green tea
Vitamin K2 as MK-7 (from natto): activates Matrix Gla Protein to block vascular calcification and redirect calcium to bone
High-EGCG green tea tablets: foam cell reduction, eNOS activation, NF-κB suppression
The three biomarkers I track quarterly as flywheel proxies are
ApoB (lipid remodelling node),
hs-CRP (inflammation resolution node), and
HbA1c (upstream metabolic driver of both lipid and inflammation nodes).
Together, they tell you which direction each sub-cycle is turning without waiting for the next imaging study.
The results, in five months of this protocol:
D1 stenosis of 77%: CT-FFR improved from 0.75 to 0.80, moving from functionally significant into the low-normal range.
Bilateral carotid CIMT reduced by 53 percent in the first three months.
All carotid plaque (~20%): gone.
LDL down 64 percent. ApoB at 45. In 12 weeks
My physician friends use the word ‘unbelievable.’ What they mean is: I don’t truly believe it.
Rob Thompson did not have this wisdom. He had a cup of tea on a February morning and an arterial wall that had been accumulating evidence against him for forty years. You have what Rob did not have. I pray you do something with this wisdom for you and your loved ones.
Your Questions
Questions worth sitting with. Answer them honestly.
1. Which flywheel are you on right now?
Not as a metaphor. Mechanically. Is your endothelium being damaged by what you eat and how you sleep, or is it being repaired? Are your macrophages in M1 inflammatory mode or shifting toward M2? The flywheel does not pause while you decide. It is spinning right now, in one direction or the other. The fractal 80/20 says you do not need to fix everything. You need to find your one thing. For most people reading this, that one thing is what they eat for breakfast.
2. What is your number one constraint?
In the theory of constraints, identifying the bottleneck is the entire game. For your cardiovascular health specifically, is it diet, and you know it? Is it sleep, which you have been meaning to address for two years? Is it that you have never had imaging and are operating on assumptions? The constraint you do not name is the one that governs everything. Name it. Then remove it. Everything else is secondary until that one is solved.
3. What is the one action you will take this week that your endothelium will thank you for?
Not a lifestyle overhaul. One thing. Order a CT calcium scan if you have never had one. Replace one saturated-fat meal with leafy greens and balsamic vinegar. Start a post-dinner walk. Ask your doctor for an ApoB measurement at your next appointment. The virtuous flywheel does not require a dramatic first push. It requires a real one. Small, specific, this week.
Someone You Love
There is someone in your life with this right now.
You thought of them somewhere in this story.
Maybe it is you.
Send this to the person you thought of while reading it. Ten seconds. It may matter more than either of you knows.
MORE READINGS YOU’LL ENJOY
Health
Reversing My 77% Heart Plaques
Stats Say You Likely Have Heart Plaque
The Healing Power of Food: Nitric Oxide
Wealth
The Power of the Compound Effect
Relentless Iteration to Mastery
Meaning
The Courage to Your Magnum Opus
APPENDIX
Key Studies in Atherosclerosis, Reversal and Cardiovascular Biology
All studies cited are peer-reviewed publications. Human trial data is prioritized throughout. This appendix reflects the evidentiary basis of the REVERSAL Protocol.
Foundational Science: The Inflammatory Basis of Atherosclerosis
1. Ross R. (1999). Atherosclerosis: an inflammatory disease. New England Journal of Medicine. Established the foundational framework that atherosclerosis is a chronic inflammatory disease of the arterial wall, not a lipid storage disorder.
2. Libby P, Ridker PM, Maseri A. (2002). Inflammation and atherosclerosis. Circulation. Detailed the molecular mechanisms by which inflammatory pathways drive every stage of plaque formation, from initial endothelial activation through vulnerable plaque and rupture.
3. Tabas I. (2010). Macrophage death and defective inflammation resolution in atherosclerosis. Nature Reviews Immunology. Demonstrated that macrophage apoptosis and defective efferocytosis drive the formation of the necrotic core that makes plaques vulnerable to rupture, independent of lipid accumulation.
4. Ridker PM et al. (2017). Antiinflammatory therapy with canakinumab for atherosclerotic disease (CANTOS Trial). New England Journal of Medicine. Proved that targeting IL-1 beta reduced cardiovascular events independent of any lipid lowering, establishing vascular inflammation as a standalone therapeutic target.
Endothelial Biology and Nitric Oxide
5. Lundberg JO, Weitzberg E, Gladwin MT. (2008). The nitrate-nitrite-nitric oxide pathway in physiology and therapeutics. Nature Reviews Drug Discovery. Established the oral-gastric dietary nitrate pathway as a clinically significant, eNOS-independent source of nitric oxide directly activated by leafy green vegetable consumption.
6. Fukai T, Ushio-Fukai M. (2011). Superoxide dismutases: role in redox signaling, vascular function and diseases. Antioxidants and Redox Signaling. Explained how oxidative stress uncouples eNOS, converting it from a nitric oxide producer to a superoxide generator that accelerates endothelial injury.
7. Werner N et al. (2003). Intravenous transfusion of endothelial progenitor cells reduces neointima formation after vascular injury. Circulation Research. Demonstrated that endothelial progenitor cells actively repair damaged vessel walls and that exercise is a primary driver of their mobilization from bone marrow.
Diet and Plaque Reversal
8. Ornish D et al. (1998). Intensive lifestyle changes for reversal of coronary heart disease (Lifestyle Heart Trial). JAMA. Showed measurable angiographic coronary artery disease regression in 82% of participants at one year and continued regression at five years, without lipid-lowering drugs.
9. Esselstyn CB Jr et al. (2014). A way to reverse CAD?. Journal of Family Practice. Found that 99.4% of compliant patients with established, angiographically confirmed coronary artery disease avoided major cardiovascular events over 3.7 years on a whole food plant-based diet.
10. Estruch R et al. (2013). Primary prevention of cardiovascular disease with a Mediterranean diet (PREDIMED Trial). New England Journal of Medicine. Demonstrated that a Mediterranean dietary pattern significantly reduced major cardiovascular events, particularly stroke, compared to a low-fat control diet.
11. Aviram M et al. (2004). Pomegranate juice consumption for 3 years by patients with carotid artery stenosis. Clinical Nutrition. Showed a 35% reduction in carotid intima-media thickness and significantly reduced LDL oxidation and blood pressure over three years of pomegranate juice consumption in a human trial.
12. Mensink RP, Katan MB. (1992). Effect of dietary fatty acids on serum lipids and lipoproteins. Arteriosclerosis and Thrombosis. Established the quantitative relationship between saturated fatty acid intake and LDL receptor downregulation, explaining the mechanistic link between dietary saturated fat and elevated ApoB particle count.
Exercise and Cardiovascular Reversal
13. Hambrecht R et al. (2004). Percutaneous coronary angioplasty compared with exercise training in patients with stable coronary artery disease. Circulation. Showed in a randomized trial that regular aerobic exercise was superior to PCI in preventing death and recurrent MI at 12 months in patients with stable coronary artery disease.
14. Pedersen BK, Febbraio MA. (2012). Muscles, exercise and obesity: skeletal muscle as a secretory organ. Nature Reviews Endocrinology. Described the myokine system by which contracting skeletal muscle releases anti-inflammatory signals including IL-10 that polarize macrophages toward the M2 healing phenotype.
15. Tall AR. (2008). Cholesterol efflux pathways and other potential mechanisms involved in the link between HDL and antiatherosclerotic effects. Journal of Internal Medicine. Reviewed ABCA1-mediated cholesterol efflux from macrophages as the rate-limiting step in reverse cholesterol transport and plaque regression, establishing why HDL function matters more than HDL-C level.
Fasting, Macrophage Biology and Polyphenols
16. Longo VD, Mattson MP. (2014). Fasting: molecular mechanisms and clinical applications. Cell Metabolism. Summarized the molecular effects of intermittent fasting including mTOR suppression, autophagy induction, and reduction of inflammatory markers relevant to macrophage phenotype and plaque stability.
17. Mantovani A et al. (2004). The chemokine system in diverse forms of macrophage activation and polarization. Trends in Immunology. Established the M1/M2 macrophage polarization framework and the cytokine environments that drive each phenotype, providing the mechanistic basis for dietary and exercise interventions targeting inflammatory macrophage behavior.
Epidemiology and Imaging
18. Enos WF, Holmes RH, Beyer J. (1953). Coronary disease among United States soldiers killed in action in Korea. JAMA. Found gross atherosclerosis in 77% of 300 American combat soldiers with an average age of 22 years, establishing that coronary artery disease begins in youth.
19. Detrano R et al. (2008). Coronary calcium as a predictor of coronary events in four racial or ethnic groups (MESA Study). New England Journal of Medicine. Demonstrated that coronary artery calcium score independently predicted cardiovascular events across diverse populations, validating CT calcium scoring as a primary risk stratification tool.
20. Fuster V et al. (2014). Progression of Early Subclinical Atherosclerosis (PESA) study design. Journal of the American College of Cardiology. Found measurable atherosclerotic plaque in 49.7% of middle-aged adults with no conventional risk factors, demonstrating that standard clinical thresholds vastly underestimate subclinical disease burden.
21. Loree HM et al. (1992). Effects of fibrous cap thickness on peak circumferential stress in model atherosclerotic vessels. Circulation Research. Established the biomechanical basis for why thin-capped, inflamed plaques rupture at low stenosis percentages, explaining why inflammation control is more important than stenosis reduction in preventing acute events.
I pray you unlock your heart to reach the height of your full potential by discovering your calling.
Kevin Ham, MD
Subscribe to my Compounding Wisdom newsletter and start transforming your life. ham.com
Subscribe to my YouTube channel @DrKevinHam for videos on how I reversed my clogged arteries in 3 months, the top foods that clear your arteries, and the first principles of health that can save your life. Like, share and subscribe — it could save the life of someone you love.
Sudden Heart Attack
Why normal people suddenly die
Why normal people suddenly die
Kevin Ham, MD
All of a Sudden
“Create in me a clean heart, O God, and renew a right spirit within me. Cast me not away from your presence, and take not your Holy Spirit from me.”
Psalm 51, written after Nathan said: you are the man
Some of you have heard this story. Many of you have not. For me, I often replay the scenes in my head as I reflect. It’s almost become like a gospel of the heart to me now. There are some stories that we care about more than others, and some that catch our fancy and then pass like the wind. I pray that this story gets caught in your heart, because for me it did, by force, to shake me and tell me to open my eyes and, really, simply ask, “Why?”
On the morning of February 10, 2025, my friend Rob Thompson got up at dawn. It was a beautiful morning. He was excited to come and see me in Vancouver. The sun rose to greet him at home in San Francisco as he made his favourite black tea, part of a Christmas gift basket I sent him every year. I always sent him a gift of healthy teas. Then he went to his home gym to train for his next European mountain summit. He had attempted to summit the Matterhorn twice, abandoning both times due to bad conditions, until he finally reached the summit on his third attempt. He was so proud. He had trained so hard. I could only imagine his grip strength and the intensity of his training.
I once tried rock climbing, which looked so easy as I watched children climb almost effortlessly, like spiders. But I had only gotten halfway, and my hands and my legs were petrified and shaking, and helplessly, I had to let go. I looked at Rob basking in his glory and understood all of the sacrifices he and his family had made for him to reach the peak. I saw the powerful physique of a mountain climber; he looked like a teenager by comparison. He was 58 years old, just three years older than me. A 35-year veteran at Goldman Sachs. He taught me much about life and his philosophy on wealth.
He died on the elliptical that morning. So suddenly it didn’t even look like he had time to break his fall. He was supposed to fly to Vancouver that day to visit me. February 10, 2025. Lunch at Sushi Nori at 12-ish. See you tomorrow, we texted the evening before, excited.
I met Rob in 2011. He had come to meet me as a potential client of Goldman Sachs. We never got to the business of banking. We became good friends instead, over years of conversations that ranged far beyond finance, the kind of friendship that accumulates compound interest quietly over time. A week before he died, Rob had invested a sizable amount in my AI company. We jested that if I had become a client of his, he would not have been able to invest due to conflict. I told him I will become his client in due time. I just believed I would have better returns investing myself, but in my 60s, we will finish what brought us together. We had been talking about what we were going to build together. That was the sentiment between us: that the best was still ahead. That we would work together. That there was time.
Rob had no warning. No prior cardiac event. No alarming stress test. He was brilliant, vigorous, and by every external measure the picture of a man with decades ahead of him. He died of a heart attack, which is to say he died of a process that had been operating inside his arterial walls for forty years with all the discretion of a well-kept secret, accumulating silently, asymptomatically, inexorably, until it declared itself, all of a sudden.
I asked God, “Why? Why now? Why Rob?”
Silence.
Inside every blood vessel you have is a single cell layer called the endothelium. One cell thick. Eight tennis courts of surface area. It produces a molecule called nitric oxide, and that molecule is what stands between a healthy arterial wall and a diseased one. When the endothelium is functioning, LDL cannot oxidize inside its walls, platelets cannot aggregate, inflammation cannot adhere, and plaque cannot start. When the endothelium is suppressed or damaged, all four protections fail simultaneously. This is where the disease begins. Not in the cholesterol number on your lab report. In this one cell layer, in this one molecule, decades before any scan would show anything at all. This is the biology that was operating in Rob, and in my father, and almost certainly in you, right now. The rest of this story is about what I’ve discovered and what that means to not only me, but more importantly, you and your loved ones. This is my gospel of the heart.
“The first clinical presentation of coronary artery disease is sudden death. In 63.5% of those who die suddenly from a cardiac cause, there is no prior diagnosis of heart disease.”
ARIC Study. Atherosclerosis Risk in Communities, 4 US communities, 1987 to 2004
The Heart of ENOS
“These men had been exposed to atherogenic factors for most of their short lives. It is no wonder that at the time of death the process was far advanced. Of 300 American soldiers killed in Korea, average age 22, 77% showed gross evidence of coronary artery disease at autopsy.”
Enos, Holmes and Beyer, JAMA, 1953
When I was in medical school, I read a study which was seared into my heart and my brain. The nature of this disease, as well as what these young soldiers did for the country in which my parents were born and raised. This study changed what cardiology believed about heart disease in the young.
Korea, 1950. An Army pathologist named William Enos is conducting autopsies on 300 soldiers killed in combat. The men are young, with an average age of 22. Too young. This was my parents’ country. My father, from a small village of just 1300 people in the eastern countryside, migrated from the poverty-stricken nation in the 60s through mining, and my mother through nursing. These young men had fought for the freedom of a people they did not know, and so I am here in Canada, grateful and forever indebted not only to my parents but also to all the soldiers who fought in the war. God bless their souls. God bless their parents. I can only imagine…
They were healthy enough to fight a war just three weeks prior. What was going through their young minds, what was in their hearts? I am heartbroken just at the thought of them. There is, by every expectation of mid-century cardiology, nothing interesting to find in their coronary arteries.
Enos opens the first vessel. He sees something that should not be there. He opens another. There it is again. He keeps going, with the methodical patience of a man who understands that what he is looking at must be documented precisely because no one will believe it. 300 autopsies. Gross atherosclerosis in 231 of them. Visible to the naked eye. In the coronary arteries of 22-year-olds?!
The finding was published in JAMA on July 18, 1953. The medical establishment responded as establishments typically do when confronted with data that would require reconsidering everything they believe: they suggested an error. They proposed artifacts of the Korean diet, the cold, and the conditions of the autopsy field. What they could not propose was an alternative explanation for 231 diseased hearts in men whose average age was 22. Because there was none. It was true then.
Every study conducted since has confirmed it. The disease does not wait for age. It does not wait for symptoms. It does not wait for your annual physical to suggest that something might be wrong.
I had seen this study in medical school, and I knew instantly that I would also have coronary plaque, likely lots, for I ate the American or Western diet. I like the acronym for Standard American Diet: SAD.
But that knowledge just passed into the void of my mind. I assumed that if I ate organic, exercised regularly, it would be fine. No deep thought given, and like the Vancouver rain, just dissipated into the sewers of my mind.
William Enos, back in 1953. Enos would become a significant word for me.
Then recently, I saw a few other studies, and I could no longer unsee or erase them. They stuck, just like the plaque that is in almost everyone over the age of 50.
In coronary arteries that measure just 1.5 mm to 6.0 mm:
85% have 0.5 mm plaque
91% have 0.3 mm plaque
Then I found other studies that were even more alarming.
The PESA study (Progression of Early Subclinical Atherosclerosis) followed 4,184 middle-aged employees. all with no conventional risk factors by clinical definition. Researchers imaged every arterial territory in the body. What they found:
49.7% had measurable atherosclerotic plaque in people the system had already cleared
Even in the most pristine subgroup (BP < 120/80, cholesterol < 200), plaque was still present
LDL within the “normal” range was independently associated with plaque presence and extent
The damage begins at 120/80. The prescription starts at 140/90. In between: years of silent endothelial injury.
But what was even more alarming:
Arterial plaque didn’t just affect the middle-aged and older; it started in childhood. The McDonald’s, Tim Hortons, fast food. The SAD diet was truly that. No wonder heart disease is the worldwide #1 killer.
Plaque Reversal
“Let food be thy medicine, and medicine be thy food. Every time we eat, we are choosing either to feed disease or to fight it. The kitchen is the most powerful pharmacy ever built. We simply stopped treating it as one.”
Caldwell B. Esselstyn Jr., MD
Prevent and Reverse Heart Disease, 2007. 20-year Cleveland Clinic study
I had read his book 11 years before I found out I had severe arterial plaque. I too set it aside, but it also resonated and echoed that I had considered trying his, what I thought was a very challenging low-fat, whole-food, plant-based diet (WFPB). But I was quickly talked out of it by friends, much too easily. I wish I had followed my intuition back then. Perhaps I would have no plaque at all, as I was only 45 then.
I had always had so many questions for its author, Dr. Esselstyn. I had never thought plaque reversal was possible until I saw the angiograms, before and after, showing how a 100% obstructed LAD had 100% blood flow just 32 months later. Dr. Joe Crowe had had a heart attack at age 44. No risk factors. Exercised. Fit. Normal labs. Normal bp. He was a fellow surgeon working together with Dr. Esselstyn at the renowned Cleveland Clinic, known for its cardiovascular department. Cleveland Clinic pioneered the first coronary bypass surgery. In fact, the doctor who performed it in 1967, Dr. Rene Favarolo, shared a surgical locker with Dr. Esselstyn.
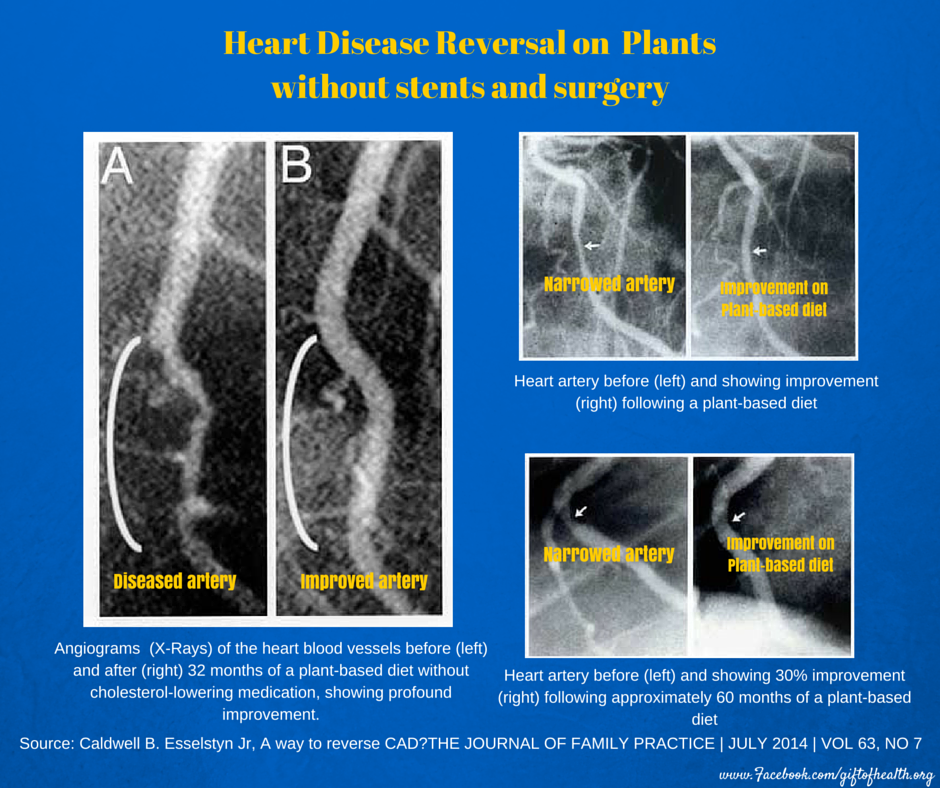
I never felt quite ready to speak with Dr. Esselstyn. Why? I felt my questions would either be too elementary or too foolish. Why not walnuts? Why not olive oil? Why not avocados? I had seen studies that show they reduce LDL. I wanted to understand more before I would ask my plethora of questions. But in the past two weeks, I really wanted to speak with him.
My friend Paulo, a former professional triathlete, had competed together with Dr. Esselstyn’s son, Rip. Paulo connected us by email. I had a great chat with Rip. Wow. He’s built a food line that espouses his father’s low-fat WFPB called Plant Strong. In all the Whole Foods and some Walmarts.
The following week, just a week ago now, I was on a Zoom call with Dr. Caldwell Esselstyn Jr. Except he wasn’t so junior anymore. 92, fit and sharp, just as he was in all the videos I watched. I devoured so many of his talks. He logically and elegantly laid out how to reverse heart disease in the most severe patients at the Cleveland Clinic. With 70 cardiologists there, he asked them for patients they could no longer treat medically or surgically. In other words, they were hopeless causes at the end of their life. So much so that some could not even endure the exertion of shaving, which could induce angina and a potential heart attack. Most could not walk a few feet without experiencing angina or claudication, pain in the legs due to plaque obstruction in the leg arteries. This was how severe their heart disease was. They also had many co-morbid diseases. The metabolic syndrome. Hypertension, diabetes, obesity, and maxed out on all the meds and already had so many bypasses and stents that their heart vessels were full of metal alloys.
His oldest patient was Stanley, an 87-year-old man who desperately needed a bypass, but the surgery for the bypass could also end his life. He elected to go to Dr. Esselstyn with a faint hope. Within days of starting the Esselstyn diet and WFPD, he was feeling better. By the end of one month, he was hopeful.
He called Dr. Esselstyn. I just wanted to thank you. I never thought I’d live to be 100. He would call each year. This year, he called. 103 years old. Now 11 years older than Dr. Esselstyn.
It was the most hopeful and miraculous story I have heard in medicine in a long time. Direct from Dr. Esselstyn. I knew I was in the presence of a very wise and great healer.
I told him my story. My multi-vessel arteries with severe plaque obstructions. He listened. I told him how I decided on May 9, 2025, after seeing the results of my CT Calcium heart scan, a shocking score of 505, putting me in the worst 90% percentile risk for a heart attack in the next 2 to 5 years, that I recalled his book from a decade prior and decided to start on his diet the very next morning. And in just 3 months, my LDL cholesterol dropped to 61, a 64% reduction, and my apoB 45, a particle measure of the potential for atherogenic lipoprotein, put me in plaque reversal mode. All of my carotid plaque: All gone! Seemingly just melted away. The word my doctor friends use is “Unbelievable.” But what I realized was that they really meant “I don’t believe it.” No curiosity. No interest in applying it to their own heart patients. And no interest in wondering if they might have heart disease.
He smiled and then started to talk. I immediately thought, I have heard this dozens of times in his videos. It almost seemed as if he was on autopilot, rehearsing a script he had told thousands of times. I was about to tell him I knew what he was going to say, but something deep down told me to just listen.
The Endothelium
“The endothelial cell is the ultimate regulator of vascular homeostasis. Its dysfunction is not merely a marker of cardiovascular disease. It is the initiating event.”
Salvador Moncada, FRS B. Esselstyn Jr., MD
Discoverer of endothelial nitric oxide.
Enos. Yes, William Enos, the pathologist. But this word would hold even more significance for you. Not only that, you may have been silently laying down the layers of plaque since your teenage years, but eNOS can also save you. This is the word he would stress. Endothelial Nitric Oxide Synthase. eNOS. The enzyme that makes this miracle transient gas we call nitric oxide. The discovery of how nitric oxide does this was awarded the Nobel Prize to three scientists I wrote in depth about, and it may be one of the most important things you read this year.
The Healing Power of Food: Nitric Oxide.
The blood vessels have an inner lining called the endothelium. It produces the most wonderful gas called Nitric Oxide. This protects, heals and supports the blood vessel wall in the smooth muscle layer. It is what allows the blood vessel to expand and allow more blood flow.”
Yes, I knew all this. He looked me directly in the eyes, leaning forward. You need to revive your endothelium. How you do that is by eating the following. He started listing off swiss chard, arugula, kale, spinach, and other foods from his whole-food, low-fat, plant-based diet. Then what not to eat. This is where he hit me hard.
No oils. No oils of any kind. Not in a cracker, not in bread, not in any food, no canola oil, sunflower oil, coconut oil, no olive oil. No oil in an animal. No oil in seafood. No oil from eggs or dairy. No oil from avocados, coconut or nuts of any kind. Do you eat oils, Kevin?
I was surprised. I did not expect him to ask me directly. I thought for a second, then declared, “No, sir.” while trying to recall the few times I ‘cheated’, thinking, ‘How could some little oil harm me?’
My patients were so sick that if they had a drop of oil, it could trigger a heart attack. No oils.
I recalled how I respected the famous coach John Wooden, winning 10 NCAA championships in just 12 years. He would get the best graduating high school players in the country. When they came to their first practice, he would get them to take off their shoes and socks and teach them how to put them on properly. Then he said lateness is not tolerated. The bus will leave on time, with or without you.
Dr. Esselstyn was the coach of heart disease. He was my coach and mentor. I had read his book multiple times and watched so many of his videos. But having him teach me to put my socks and shoes on and not show up late for my heart and my food was … well, humbling, and I was deeply grateful.
I decided I would rededicate myself to following his dietary protocol as best as I could. There were still so many questions I wanted to ask him. It was not yet time to ask them.
What damages the endothelium? He went on in his great talk.
Then he said that there was something new. I perked up. He learned that people recovered faster when they ate greens 6 times a day. A handful or cupful in boiled water for 5 and a half minutes. And liberal amounts of balsamic vinegar.
Greens 6 times a day? I had heard this in his videos. Hmmm, I wanted to intermittent fast, that is, not to eat for 18 hours and eat my two big meals at noon and 6. This would break my fast, the breakfast. He went on to explain that it was so important to chew my greens, as the nitrates in them would be converted to nitrites by the bacteria in my mouth. I need to remove mouthwash, fluoride in my toothpaste, and any antacids, as the stomach acid converts the nitrites to nitric oxide. This occurs for hours. So greens 6x per day. All day long, so your blood vessels are anointed with nitric oxide. It made so much sense. The vinegar would enhance the nitric oxide from the food.
I need to do this. I need to sacrifice my intermittent fasting and do this.
In the am, mid morning, lunch (big salad), mid afternoon, dinner (big salad), and he said it would make him really happy if I could have a handful of greens a few hours after dinner.
I thought that was a no-no… to eat too close to bedtime. But he proved it in the worst heart patients. I was not as bad as they were, but I did have a 77% blockage.
I still ride my bike up mountains. No symptoms. My latest CT angiogram showed an 80% FFR, down from 75% five months prior. This is now normal blood flow. Low normal but normal. My carotid plaques were long gone. No more low-attenuated plaque, the dangerous plaque that can burst.
I’m going to do it.
The Ostrich in the Room
“Coronary artery disease need not exist, and if it does exist, it need not progress. With rigorous cholesterol reduction and a plant-based diet, we have documented not merely the arrest but the reversal of this disease in human beings.”
Caldwell B. Esselstyn Jr., MD 20+ years of outcomes data. American Journal of Cardiology
What has been silently and slowly building from childhood starts to declare itself on lab tests, on scans starting in your 40s, progressing into your 50s and typically declaring its coming of age debut as a disease in your 60s for men and 70s for women.
It often seems all of a sudden. It was declarative for Rob. It was shocking for me, and I had learned this as a doctor. Yet the brutal reality of what is happening and how long it has been happening is almost hard to believe. Unbelievable.
At Rob’s memorial, an impressive hall for the Freemasons in downtown San Francisco, there were thousands gathered to pay their respects. We stood in line, waiting to sign the book with our heartfelt wishes to Rob and his family. A line full of suits, and you could tell professional, wealthy and their families. This was the impact Rob had. His Goldman clientele, as he managed the wealthiest people on the West Coast, including the epicentre of tech, Silicon Valley.
I saw the self-driving taxis ushering people to the memorial. No driver seen. It was uncanny. It was like I was now living in the age of the Jetsons.
Anita, Rob’s wife, came to the stage, and the room was hushed, waiting for her heart to speak. It was one of the most impactful talks I have listened to. Then she said, “Let’s speak about the elephant in the room. Rob had a stress test every day. Every workout, every climb was more than a stress test, and he passed it every day. He had more energy and fitness than anyone in this room. He had 90% blocked arteries, and he would pass any ECG stress test. He had slightly elevated LDL cholesterol that was brought to the normal range by a statin. There was nothing to indicate that he would die of a heart attack. Many of you may be the same. I ask each of you to go and get a CT calcium heart scan. It will tell you if you have plaque and your risk of a heart attack.”
So my wife and I both got one. You know the story. Wife: score 0. No calcified plaque. Me: score 505. Severe calcified plaque. Later, I found out that it was in every heart vessel and every branch. 77%, 55%, 45%, 29%, 28%, 21%, 20% etc. Everywhere. I could be dead, all of a sudden, riding up the mountain in 1 to 5 years if I had not known. Now I do, and I am reversing my plaque.
The elephant is a powerful analogy. It’s a big thing, but no one is actively talking about it. But I also think there is a world full of ostriches. They don’t want to even think about it, let alone discuss it. The elephant everyone thinks about. But the ostrich buries its head to escape the predator. So many people I speak to don’t want to discuss even the possibility that they might have plaque. But whether you bury your head in the sand, biology follows the laws of health. When these laws are transgressed, that health unravels, slowly but surely. It’s better to know earlier rather than all of a sudden. I am glad I know I have clogged arteries. I was surprised all of a sudden with wet macular degeneration. To me, they are the same disease, just different organs. Same with diabetes, high blood pressure and metabolic diseases. Just different organ systems. I’m reversing both, so help me God.
Here is a picture of how a plaque in the carotid artery in the neck builds up over ten years, from age 45 to 55. A seemingly healthy person. Normal lipids: Cholesterol 165 mg/dL, HDL 71, Triglycerides 64. Normal blood pressure. No symptoms. At 45 years old, he had a small plaque, 1.3 mm. Ten years later, at age 55, he had a type 5 plaque, a thin-cap fibrous plaque indicating a high risk of plaque rupture, that could result in an embolic stroke. His risk of a heart attack due to similar plaque in the heart would be high as well. All of a sudden.
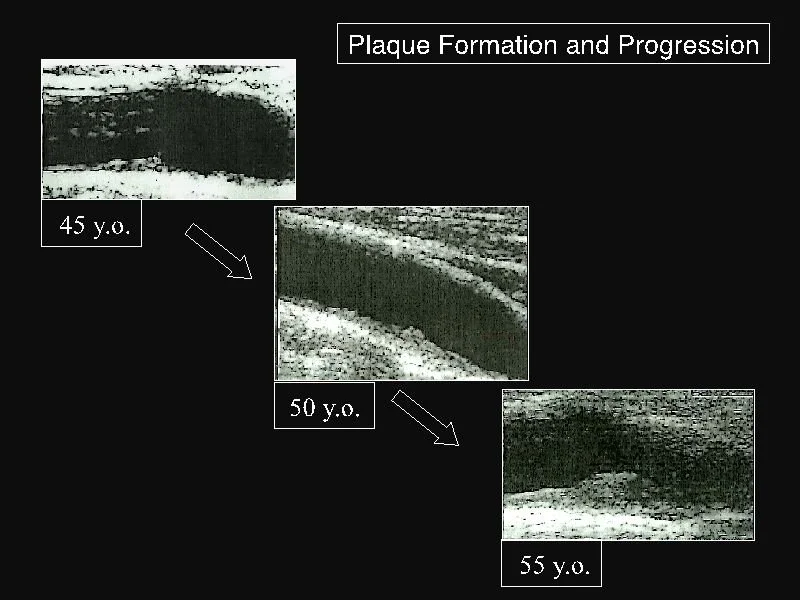
Plaque formation and progression in the carotid artery.
Ultrasound imaging of the left carotid artery in a long-axis during a 10 years period follow-up (1998-2008) in a healthy man from 45 to 55 years of age.
And below are the six types of plaque and their progression. My plaque is in stages 4-6. The later the stage, the more difficult to reverse. I am not sure the calcified plaque can be reversed, but my thought is that if bone can demineralize, what we call osteoporosis, why can’t diseased calcified plaque be demineralized? I have some really good leads on how the body can do this if you set the right healing conditions.
What goes up must come down. What has been building in me for 40 years can reverse in as little as 3 years. I do not know if I can attain the full 100% blood flow that Dr. Joe Crowe experienced in his mid to late forties. I believe I can. Might take longer to break down the more mature plaque.
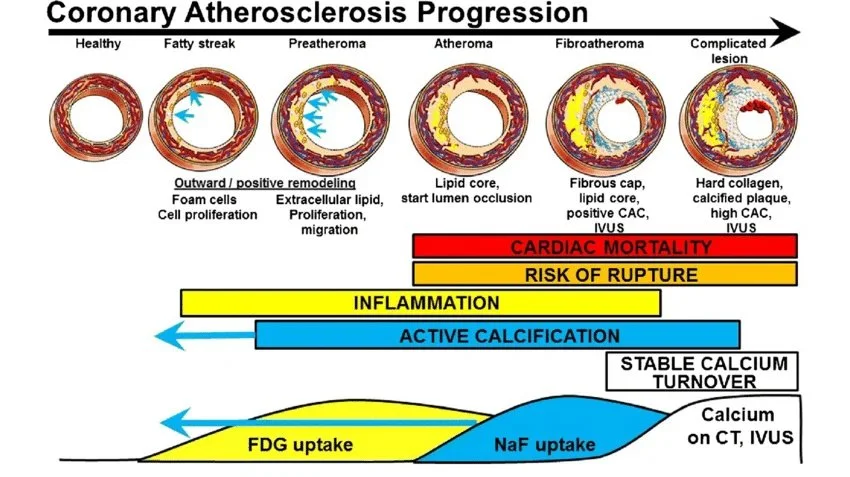
European Journal of Nuclear Medicine and Molecular Imaging November 2018: 45(Suppl 3):1-11
I think of it like the stages of cancer but applied to plaque. But plaque doesn’t fight back like cancer and if I fight it with everything that has been shown to reverse plaque, I will attack it at all levels. I will find every weak link in the plaque and the pathways for plaque buildup and plaque reversal.
And this is what plaque looks like as it remodels. My carotid plaque remodeled so quickly and disappeared.
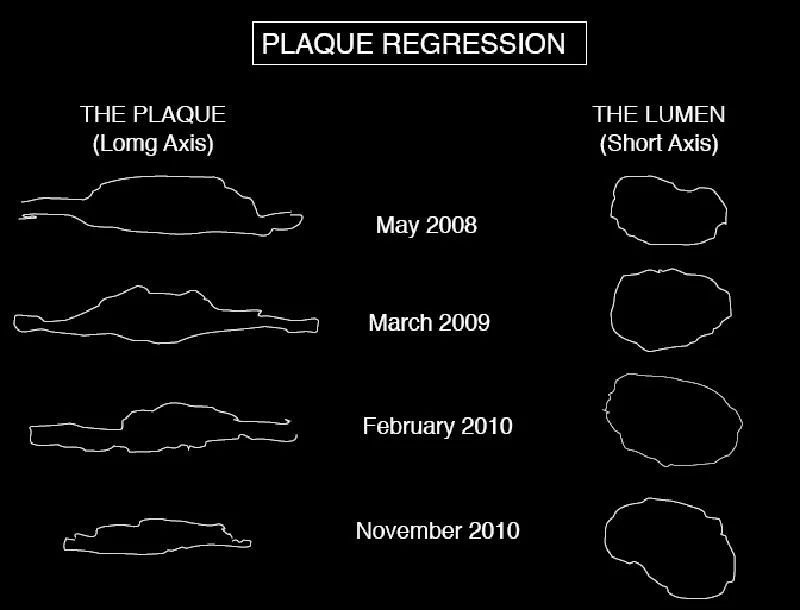
Plaque remodeling and reversal. B-mode ultrasound imaging of the carotid artery.
I started a YouTube channel. Not only for me, but also for Rob, and for almost everyone who is willing to fight.
Maybe you’ve seen it. My latest video, The Three Blood Tests that is better than cholesterol, went viral. This then led to an older video going viral. So I went from 0 subscribers to now over 8000. I will likely be ~20,000 by the end of this March. My goal is to educate people. I have found that this gospel of the heart I preach falls short.
So I do what I always do when I don’t know. I study. I study the data, the studies. I think I have figured out the biochemical pathways, the constraints and the 80/20 levers. As I learn the details, I realize how amazingly complex the body is, but also how remarkable. We just need to stop preventing it from healing itself and then find natural remedies to speed it up.
The good news, the gospel, is that this progression to the cliff of death, the top killers, heart attacks and strokes, can be arrested and, more importantly, reversed.
Just like the body can heal a fracture, it can recover from a stroke; your body has the means to reverse plaque.
It’s called Reverse Cholesterol Transport.
I've already proved it in my carotid arteries. In just three months. I haven’t found anything as fast and complete as mine in case studies or randomized controlled trials… yet. Did I set a world record in plaque reversal?
My hypothesis was that, just as a fractured bone heals in 3 months, why can’t plaque reverse in three months? Then I created a three-phase attack leveraging everything I learned from Esselstyn. Diet x Exercise x Fasting. My big weak point: sleep. I will solve that too.
You’ve all seen this by now. My plaque reversal. I believe it will make its rounds around the world as I continue to preach the gospel of your heart. I feel it is part of my calling. Doctor. Patient. Friend. I understand better now. I pray to God that I will understand more.
Your Questions
“Before I formed you in the womb I knew you, before you were born I set you apart.”
Jeremiah 1:5
Questions worth sitting with
For yourself. For someone you love. Answer them in the quietness of your day.
1. When did you last have imaging of your arteries, not just blood tests?
A lipid panel tells you what is circulating in your blood. A CAC score or CT angiogram tells you what has already built up inside the vessel wall. These are not the same question. One answer: What are your risk factors? The other answers: what has already happened. Most people have been asked only the first one.
2. Do you know your ApoB?
LDL-cholesterol is a proxy. ApoB is the actual count of atherogenic particles in your blood. It correlates more directly with plaque burden and cardiovascular events than any standard lipid panel number. Most annual physicals never measure it. Ask for it by name at your next appointment.
3. What did you eat yesterday, and what was that food saying to your endothelium?
Not a moral question. A molecular one. Every meal either upregulates eNOS or suppresses it. Either raises postprandial triglycerides or keeps them controlled. Either accelerates the disease or begins to reverse it. You made that decision yesterday. You will make it again in a few hours. The endothelium is listening to every meal.
Someone You Love
“The greatest single threat to the cardiac health of each individual is his own coronary arteries. And the greatest threat is not that we lack the knowledge to prevent the disease. It is that we lack the will to act on what we already know.”
Paul Dudley White, MD Presidential physician, founder of the American Heart Association. 1956, the year coronary disease became the leading cause of death in America
There is someone in your life with this right now.
You thought of them somewhere in this story.
Maybe it is the friend who is 53 and has not had a cardiac scan since his annual physical 5 years ago, which came back fine. That tells him nothing about what is in his vessel wall.
Maybe it is your parent, who has a family history of heart disease that came up briefly at one appointment and was never followed up with imaging.
Maybe it is your son, who lifts weights and believes the body he has built exempts him. The PDAY data do not agree. The wall does not negotiate.
Maybe it is you.
Rob Thompson did not have this wisdom. He had a cup of tea on a February morning, an investment in a company we were going to build together, and an arterial wall that had been accumulating evidence against him for forty years without producing a single symptom he could have acted on. He had been thinking about the future. The disease had been thinking about nothing. It does not think. It does not hesitate. It simply completes the process it began in the vessel wall.
You have what Rob did not have. Send this to the person you thought of while reading it. Ten seconds. It may matter more than either of you knows.
MORE READINGS YOU’LL ENJOY
Health
Reversing My 77% Heart Plaques
Stats Say You Likely Have Heart Plaque
The Healing Power of Food: Nitric Oxide
Wealth
The Power of the Compound Effect
Relentless Iteration to Mastery
Meaning
I pray you unlock your heart to reach the height of your full potential by discovering your calling.
Kevin Ham, MD
Subscribe to my Compounding Wisdom newsletter and start transforming your life. ham.com
Subscribe to my YouTube channel @DrKevinHam for videos on how I reversed my clogged arteries in 3 months, the top foods that clear your arteries, and the first principles of health that can save your life. Like, share and subscribe — it could save the life of someone you love.
Descent of the Soul
The valleys everyone must pass through.
The valleys everyone must pass through.
Kevin Ham, MD
The Last One Picked
I was usually one of the last ones picked.
I always felt so relieved when I was not the very last one picked. It meant I was more highly valued than at least one other person.
Last. That distinction belonged to someone else. And I was always grateful for it, as one is grateful for anything that distracts from obvious humiliation. But I was still late. The last of a handful of picks. The teams would form with the obvious stars first, down to those who seemingly didn’t matter.
I would apprehensively stand at the edge of that contracting pickup line, waiting. Tiny for my age. Just peeking over five feet in Grade 6. Quiet in a way that registered as invisible rather than deep. Easy to overlook.
I once fought the toughest kid at school. The biggest guy in Grade 5. Not because I was brave. Because something inside me wanted to show the others I was present. And the only language available for what I needed to say was physical. Words could not express the depths of my loneliness. I got him on the ground. A kid yelled, “Punch him!” I did. Right in the nose. He started to bleed. I got up and walked away. Afterward, the other kids looked at me differently, and that shift mattered more than the outcome. I could go up against the biggest and prevail.
Inside was not what the outside suggested. I had a creative spark inside of me that was insatiable. I was devouring Tolkien, reliving the Shire and the Mines of Moria with a completeness that left little room for the world requiring me to be smaller than I was. I was on that journey to Mount Mordor. I could visualize every scene. Peter Jackson did it almost as well as the visuals that played in my head. Then C.S. Lewis. The Narnia series. I did not know at the time that he was also a great philosopher. Then the Thomas Covenant series, which nobody else I knew had read, except my older brother Don, who introduced that and Terry Brooks’ elven series to me, which was precisely why I loved it: a leper, unclean, rejected, transported into a world where his very disease became a form of power. Then the Black Stallion. Then everything I could find. I was not reading to escape. I was reading to locate something I could not yet name. A self that the exterior world could not translate, but that I could feel the shape of, pressing outward from the inside.
The word I would have used, if I had known it then, was anointed. This word is special to me. Not in the religious sense. There was something in me that had been set apart before the setting apart had been made visible. The overlooking was not the verdict. The field was not the destination.
I did not know that word. But I found the men who did.
I David
“Create in me a clean heart, O God, and renew a right spirit within me. Cast me not away from your presence, and take not your Holy Spirit from me.”
Psalm 51, written after Nathan said: you are the man
My mother sent me to church with another Korean family with the same last name, Ham. I don’t recall much except that I had memorized some verses from the book of Proverbs and won a Bible as the prize. I read one of my favourite Bible stories, David and Goliath. The shepherd teenager who went against the giant and beat him. I found David the way you find something you had been looking for without knowing you were looking.
Here was a young boy who had been left in the field while his father presented the other sons before the prophet Samuel. The youngest, the smallest, the one not considered worth summoning until the prophet asked: Are these all of your children? And even then, David arrived covered in the smell of the field, ruddy and wild-eyed, not the picture of an anointed king.
This is the one, said the Lord.
The oil was poured. And David simply went back to the sheep.
What reached me was not the crown. It was the dozen or more years between the anointing and the crown. David returned to the same life he had lived before Samuel came. Anointed and unknown. Carrying an authority that had no external expression yet. Hunted through the wilderness by the king he served and would replace. Building an army out of men who had been cast out by the world and found him worth following. He was thirty years old before anyone outside his circle saw the fruits of the oil that had been poured.
I understood it then, not as theology, but that this pattern could also be in my life and everyone else’s, too. The field is not the failure. The obscurity is not the verdict. The anointing precedes the confirmation, sometimes by decades, sometimes a lifetime, and the work of the valley years is not to convince the world that the anointing is real. It is to become, through the pressing, the person capable of carrying what the anointing requires.
“You have shed much blood and have fought many wars. You are not to build a house for my Name, because you have shed much blood on the earth in my sight.”
1 Chronicles 22:8
But there is something anguishing in David’s story more than the valley years. The dream he longed for most, the longing that sat at the centre of his life like a fire that never doused, was to build a house of peace. The Temple. Jerusalem: the city of peace. He conquered the Jebusites, the last bastion and city, after centuries and rebuilt the city of David. He had the plans for the Temple. Glorious. Magnificent. Worthy of God. He had gathered the materials. He had devoted his life to making the kingdom secure enough that the Temple could stand.
Then God told him: You cannot build it. You have shed much blood. A man of war shall not build a house for my name.
There is no more heartbreaking sentence in the Hebrew Bible. Not because David was denied the Temple through failure. But because the very quality that made him great was precisely what disqualified him from the work his soul had been desiring his entire life. He was too good at the wrong thing. His greatest strength was the door the Lord closed. For peace, he had to go to war and shed blood.
When Nathan came with a different reckoning, the Bathsheba reckoning, David did not argue. Using power for deceit, adultery, dishonour, murder and evil. He said just five words, in remorse.
I have sinned against the Lord.
That instant recognition and humility is the priest-work still alive beneath everything, no matter how vile or grievous. His Psalm 51 became the language of confession for every generation that followed. The king-work was diminished by what he had done. The prophet-voice was deepened by what the valley stripped away.
I read the Psalms, all 150 of them, when I feel what I felt in that circle. Passed over. Misjudged. Or when I have sinned greatly. When I am late to be picked, or not picked, or pick myself and discover the self I have picked is smaller than the one I feel pressing from the inside. They do not resolve the feeling. They name it. Which is something more useful than resolution.
II Solomon
“Vanity of vanities, says the Preacher. All is vanity. I have seen all the works that are done under the sun, and behold, all is vanity and chasing after wind.”
Ecclesiastes 1, written at the end of everything
Solomon, the ‘illegitimate’ son of David, unlikely to be heir and king, did become king. He had the kingdom set up for him by his father. Anointed in David’s last days. He was so young that when God asked him at Gibeon what he wanted, he asked for wisdom to rule the people. And he got plenty of wisdom. More wisdom than anyone in history, a direct gift, in exchange for nothing. You can feel and read that wisdom in his Song of Songs, the most ecstatic love poem in any language, and in his three thousand Proverbs, aphorisms crystallized from a man who observed human nature and nature with an eternal eye. He built the Temple that David had been forbidden to build, and his writings on the vanity of life and its conclusion in Ecclesiastes. I ponder these books daily. I have a dream to inscribe them in my heart so I may have a heart of wisdom. But I wondered, how could someone so wise have become so foolish, especially when he had everything given to him?
I was foolish, so it was understandable, and so I seek wisdom, but once you have wisdom, can you become so foolish as to completely unclothe wisdom?
“He must not take many wives, or his heart will be led astray. He must not accumulate large amounts of silver and gold.”
Deuteronomy 17:17. The law written for kings, before Solomon was born
Before any of it, God had given the kings four laws specifically for kings. Four prohibitions, each one a warning written in advance against the temptations specific to the man who sits on the throne. Do not multiply wives. Do not multiply horses. Do not multiply gold. Do not place your trust in foreign alliances above the Lord.
Solomon opened all four doors.
Seven hundred wives. Three hundred concubines. The Temple of the Lord and the altars of Moloch, the same man, the same city, the same life. The wisest man who ever lived warned specifically against his specific temptations, violating every warning systematically.
Vanity of vanities. All is vanity.
I have built companies. I have assembled a kingdom, three hundred thousand premium domains bought during the dot-com bust while everyone else was fleeing. I have read Solomon’s reckoning, the way a man reads a story that could have been written about him. Not the wives. But the accumulation. The building of structures that kept the deepest question at a horizon’s distance. The way achievement, if you build enough of it, functions as insulation from the self that was anointed before the building began.
Solomon found his way back. At the end of Ecclesiastes, stripped of every layer, the thread he had buried under a thousand coverings became visible again. What he had known at Gibeon, before the wives and the horses and the gold: fear God and keep his commandments.
The descent made it recoverable. This is not consolation. It is architecture.
III Marcus Aurelius
“You have power over your mind, not outside events. Realize this, and you will find strength. What stands in the way becomes the way.”
Meditations, written in a military tent on the Danube frontier, never intended to be read
I was introduced to Marcus Aurelius through a film.
Gladiator. 2000. Nominated for 12 Oscars, winning five. It blew me away. It was the evening I had just written my medical exams for my Medical Residency Certification, FRCP. I had the practicums the next day, but because I was building my Internet businesses at the same time, I thought that I would roll the dice. If I passed, I would continue in medicine. If not, I would continue being an entrepreneur. Surely I could not do both well.
I passed.
The old emperor at the edge of the screen, tired in a way that power cannot cure, gives Maximus a commission he knows cannot be kept. What struck me was not the tragedy. It was the face. The face of an aging man who has been required to live a life other than the one he was made for, and who has been living it with such sustained integrity that the requirement and the man have become indistinguishable, and who is still, somehow, the man underneath.
I later read Aurelius’ Meditations. I was not prepared for what I found. I should go back and reread it with new eyes.
This was not mere philosophy. This is a man talking to himself in a military tent on the Danube frontier, in the second person, as if the person he is addressing cannot quite be trusted to remain himself under war and politics. He writes the same principles many times. He is not working out a new thought. He is holding the thread against a current that continually pulls it downstream. Repetition is the cost of maintenance.
Marcus had wanted to be a philosopher. He had built an interior practice of extraordinary depth by his late twenties. Then the emperor died, and Marcus was emperor, and the life he had been building was over. Fourteen of his nineteen years on the throne were spent on the Danube frontier, managing wars necessary but not meaningful, watching his son Commodus developing year by year into the catastrophe he could foresee and could not prevent.
In the margins of the king-life, the priest-work survived. The Meditations were never meant to be read. Originally named Ta eis heauton ("to himself"). They are the private 12-book journal of a man striving to stay true to himself from the demanding life the world required of him. They have been read continuously for eighteen hundred years by people in exactly his situation: formed for one life, living another, trying to hold the thread.
The king-work of the Roman Empire is archaeology. The priest-work of the margins is alive.
The Oil and the Gap
“Even though I walk through the valley of the shadow of death, I will fear no evil, for you are with me.”
Psalm 23:4
My mind always seeks to weave threads in the seemingly unrelated. The brain works this way. Neural networks. Logic on the left brain with creativity on the right. I found the oldest framework to connect these three men and many others, me and you as well: the ancient world had a name for the three offices every anointed life must pass through, and a name for the valley between them. The prophet. The priest. The king. In that order. Each requiring a ceremony before the work could begin. Each requiring the valley before the office could be inhabited.
Three different descents. Three different reasons for the crushing. The same discovery at the bottom: the thing you buried is still there. The oil does not evaporate during the years in the field. It waits.
There was an art teacher who handed back an assignment I had worked hard on and was proud of. I can’t even recall what it was anymore because, for me, it was a traumatic experience.
I was thirteen. I had drawn something I cared about. The grade? C+. Not failure: worse than failure. Failure, you can argue with. C+ is a verdict without appeal: you are here, slightly above mediocre, and that is all you will ever be.
I eliminated art and any subjective courses from my future selections when possible. I decided to focus on exact, objective courses: math and sciences. I became a doctor. Then, a man who built a kingdom where no one would ever be in a position to give me a C+ again.
What I did not know: you cannot remove an anointing. It remains dormant, much like shingles, the chicken pox virus that appears when you are weak. You can only forget it. You bury it deep in your soul. It’s buried in the field. But it arises in the dark. In the valley. Every patient attended to beyond the clinical. Every conversation that became more than business. Every time I reached past the kingdom toward the story underneath it. The drycleaning shop. The three hundred thousand domains. The cardiovascular scan on the wall. All of it pressing. All of its formation.
The olive must be crushed to yield oil. The pressing is essential to the oil’s production. It is the mechanism of production. The crushing is not the destruction of the olive. It is the fulfilment of the olive’s purpose. The oil was always there, latent in the fruit. The pressure does not create it. The pressure releases what was always present but had no way of expression.
I did not know this when I was the boy at the edge of the circle, waiting to be picked. I did not know it when I gave up on my dreams after the C+. I did not know it when I built the first company, or the second, or when I assembled a portfolio of three hundred thousand domains while the internet was collapsing around me and told myself that this was what I had been made for. You do not know it during the pressing. You only know it when the oil appears, and you recognize it, and you understand that it was there the whole time.
I am somewhere between Bethlehem and Hebron. Between the private ceremony and the public confirmation. Between the anointing and the crown. Forty years in the field is a long time pressing. I am beginning, now, to feel what it has done.
Which Descent Is Yours
“The Lord does not look at the things people look at. People look at the outward appearance, but the Lord looks at the heart.”
Leo Tolstoy
Every person reading this is in one of these three descents.
The disqualification: the thing you long for most is what your life has made you unworthy to build.
The disobedience: the laws written specifically for you, warning you against your specific temptations.
The assignment: no fault, no drift, only the wrong life handed to the right person, and the question of whether the right life survives inside it.
The pattern is not coincidental. It is architectural. The spirit speaks first. The soul translates. The body builds. In that sequence, properly esteemed, the result outlasts the builder.
The valley is not punishment. It is the expression.
I do not know how this ends. Just as the other side of the summit cannot be seen from the valleys. I do not know what the crown looks like or whether I will recognize it when it comes. I do not know whether the books in my heart get written, whether companies become what I dream about, whether the musical playing in my heart manifests, or whether the cardiac scan in 2028 shows what I believe it will show. I do not know if the anointing I felt pressing outward from the inside at thirteen, in East Vancouver, in the line waiting to be picked, was the real thing or only the wish for it.
What I know is that the oil is not gone. That the pressing has a purpose. That Samuel came to Bethlehem looking for something the world had not confirmed yet, and found it in a field, and that the field is not the end of the story.
The dream did not die with the C+. It went into the field.
It is still there.
Prophet. Priest. King. In that order.
The spirit first. Always the spirit first.
Your Question and Your Assignment
“Before I formed you in the womb I knew you, before you were born I set you apart.”
Jeremiah 1:5
The Life Question
Which of the three descents is yours right now?
Not which one you prefer. Not which one is most exciting. Which one is actually operating in your life at this moment? The disqualification: the thing you long for most is precisely what your formation has made you unable to build yet. The disobedience: the laws written specifically for you, warning you against your specific weakness, and whether you are inside them or outside them. The assignment: the life you are living is not the life you were made for, and the question is whether the life you were made for is surviving inside it.
Write the answer down. One sentence. The descent has a name. Name it.
Three Applications
Find the buried thread. Every person reading this has buried something. A vocation, a longing, a creative life, a calling heard before the world had a category for it. The oil is not gone. Name the thing that was buried. Write it on a piece of paper and put it somewhere you will see it every morning for one week. You do not have to act on it yet. You only have to stop pretending it is not there.
Audit the laws written for you. Solomon had four specific prohibitions. Each one was a door his particular weakness would be tempted to open. You have your own four. They are probably not the same as Solomon’s, but they are equally specific and equally predictive. What are the four things that, if you allow them, will bury the thread? Write them. Post them. Not as shame but as intelligence. You are not weaker than Solomon. You are the same kind of person, facing the same kind of doors.
Do the priest-work in the margins. Marcus Aurelius kept his interior life alive in whatever margin the king-life left. Fifteen minutes in the morning. A journal entry on the commute. A walk without a podcast. The priest-work does not require a monastery. It requires a margin you can write on and the decision to protect it. Identify your margin. Name the time. Defend it the way you defend a meeting with someone you cannot afford to disappoint. Because you cannot. This newsletter is my margin. It pulls on the thread buried deep in the field. I am threading and weaving it through me to you.
There is someone in your life who is in one of these three descents.
You already know who it is. You thought of them while reading this.
Send it to them. It will take you ten seconds. It may matter for years.
MORE READINGS YOU’LL LOVE
Meaning
The Courage to Your Magnum Opus
Wealth
The Power of the Compound Effect
Relentless Iteration to Mastery
Health
Reversing My 77% Heart Plaques
I pray you unlock your heart to reach the height of your full potential by discovering your calling.
Kevin Ham, MD
Subscribe to my Compounding Wisdom newsletter and start transforming your life. ham.com
Subscribe to my YouTube channel @DrKevinHam for videos on how I reversed my clogged arteries in 3 months, the top foods that clear your arteries, and the first principles of health that can save your life. Like, share and subscribe — it could save the life of someone you love.
The Cocoon of Wealth
Wealth is the Obesity of the Spirit
Wealth is the Obesity of the Spirit
I. The Borrowed Dollars
Hope is nature's veil for hiding truth's nakedness.
Alfred Nobel
My father came to Canada with $100 borrowed.
Not from the South Korea you know now—K-pop, K-dramas, K-beauty, and the 14th-largest economy on earth. He came from South Korea of the 1960s. War-torn after the civil Korean War. A country trying to rebuild itself from rubble. A country where the path to a better life was a plane ticket to a nation cold enough to need the work ethic Koreans carry wherever they settle. First, he went to the mines of Germany, then to Toronto, then to Vancouver. The east side.
“Charlie” (my father’s nickname because his Korean name was hard to remember) was an entrepreneur with no “higher education” and no safety net. He built a chain of laundromats and dry cleaning stores. One, then two, then several.
He handled strangers' clothing and made them look new again, 7 am to 11 pm, seven days a week, year after year, for most of my life. No days off. Never sick. The only time his kids (my brothers and I) saw him was when we helped out at the laundromat after school or on weekends.
My mother was a nurse. She worked graveyard shifts. Always sleep-deprived. Which, as we know now, is a recipe for disease, a shorter healthspan, and a shorter lifespan.
My father strove for financial freedom. For the family. He came from a country town of just 1300 people. He strove with everything he had. He never fully attained it. That fact sat inside my soul the way a stone sits at the bottom of a river. Our conversations today (he’s 90 now) still hinge around making money.
I am a physician. I left clinical practice twenty-five years ago to build companies. I acquired domain names during the dot-com collapse, built businesses to eight- and nine-figure revenues, assembled a 300,000 premium domain name portfolio that a magazine once profiled under the headline "The Man Who Owns the Internet." This was not ambition. It was a son finishing what his father started, on an internet his father could not have imagined. The body inherits more than genes. It inherits unfinished sentences.
I finished the sentence. With exclamation marks (!!!), fulfilling all the dreams in my heart. I attribute this success mostly to God’s providence. And afterwards, I stood inside the resounding silence that followed to discover a question nobody had prepared me for:
What do you do when you have accomplished your dreams of wealth? What is higher than wealth? To whom do you look up when you are wealthy beyond your imagination?
At 53, an ultrasound revealed plaque in my carotid arteries. I ride a bicycle 7000 km a year with 100,000 metres of climbing (like climbing Mt Everest 9 times). I now eat with the molecular-level paranoia of a man who is on the edge of the cliff of life.
The #1 killer disease does not care about your cycling mileage. It is interested only in the endothelium, the single-cell-thick lining of your blood vessels, and whether you have been paying attention to it.
I have spent nine months establishing a reversal protocol. Aggressive dietary intervention, paired with exercise and fasting, topics that make dinner parties very uncomfortable. Three months later, my carotid plaque was gone. The ultrasound was clean. My cardiologist and doctor friends called it remarkable. Actually, the right word would be Unbelievable! I can tell that most of my doctor friends do find it unbelievable.
I call it terrifying because what the reversal proved was that I had spent years finishing my father's sentence while my own arterial walls were quietly calcifying and obstructing. I was too busy accumulating to ask what the accumulation was for.
The plaque was the visible issue. But behind it was an invisible one—a question neither my father's borrowed $100 could have purchased, nor my wealth could have answered:
What is wealth for?
I found the answer in three rooms, in three different centuries, occupied by three men who had nothing in common except the thing that was destroying them.
II. The Merchant of Death
Contentment is the only real wealth.
Alfred Nobel
On a Tuesday morning in 1888, Alfred Nobel unfolded a newspaper in his suite at the Grand Hôtel in Paris and read his own obituary. A French journalist had confused Alfred with his recently deceased brother Ludvig. The obituary’s headline called Alfred “the Merchant of Death”. Alfred had found new ways to kill people faster than ever before. He had gotten rich doing it. That was the whole story.
Nobel was 54. He held 355 patents, factories in 20 countries. He owned Bofors, the Swedish arms manufacturer. He had stabilized nitroglycerin with diatomaceous earth, called the result dynamite, and within a decade had reshaped mining, construction, and warfare. His personal fortune was worth 31.5 million Swedish kronor in 1896, equivalent to $200 million USD today.
He also had no children, no lasting romantic relationship, and no home. He lived out of hotels, not as a cosmopolitan but as a man without a country. He suffered from depression so persistent it was like air. To his sister-in-law, he wrote that she lived a warm, glowing life with loved ones, while he drifted without a compass, a wreck on the sea of life.
This, from a man who could purchase anything on earth. He had no real meaning, calling or purpose.
Nobel set the newspaper down. He did not call his lawyers. He sat with it the way a patient sits with a diagnosis. And in that silence, something structural broke. Not his health. Not his mind. The wall between the life he had built and the life he wanted to mean something more than himself.
III. The Rope Behind the Bookshelves
Is there any meaning in my life that the inevitable death awaiting me does not destroy?
Leo Tolstoy, A Confession
In the winter of 1879, behind the bookshelves in his study at Yasnaya Polyana, Count Leo Tolstoy concealed a length of rope. He also removed his hunting rifle from his own reach. Not because he distrusted the weapon. Because he distrusted himself.
He was 51. War and Peace had remade the European novel. Anna Karenina was complete. He owned 4,000 acres, had 13 children, and possessed the kind of fame that makes further achievement feel meaningless. What he was experiencing was not depression in the clinical sense but something more dangerous: a crisis of meaning in the presence of utmost abundance.
He did not use the rope. The novelist became a philosopher. The aristocrat became an ascetic. He renounced his copyrights, tried to give away his estate, dressed as a peasant, made his own boots, and was excommunicated by the Orthodox Church. The Kingdom of God Is Within You, published when he was 65, became the foundational text of nonviolent resistance. Gandhi read it in South Africa and felt a political philosophy lock into place. Martin Luther King traced his lineage through Gandhi back to Tolstoy's study. That chain began with a man who put down a rope.
In his final years, Tolstoy decided that War and Peace and Anna Karenina were not his greatest works. He spent fifteen years compiling A Calendar of Wisdom, a day-by-day collection of the world's deepest thoughts on how to live, drawn from Epictetus, Marcus Aurelius, Lao-Tzu, the Gospels. He called it his most important contribution to humanity and reread it daily for the last seven years of his life.
At 82, he fled his estate in the middle of the night. Died ten days later at a railway junction called Astapovo, in a stationmaster's bed, owning nothing.
IV. Christmas Eve
I read in a book that a man called Christ went about doing good. It is very disconcerting to me that I am so easily satisfied with just going about.
Toyohiko Kagawa
Kobe, Japan. Christmas Eve, 1909.
A 21-year-old seminary student loads his belongings into a bamboo box on a hand cart. His name is Toyohiko Kagawa, and in forty-five minutes, he will walk through a doorway into a place that even the police have abandoned.
The Shinkawa district. The worst slum in Japan. Open sewers, endemic tuberculosis, and ambient violence so constant that the municipal authorities had classified the district as unrecoverable. A place you quarantined and waited to see die.
Kagawa was walking in.
He was the illegitimate son of a Cabinet minister and a concubine. Both parents died before five. Two American Presbyterian missionaries, Harry Myers and Charles Logan, had taken him in, taught him English, and shown him a faith that would cost him everything he had. He was disowned at fifteen for converting to Christianity in Meiji-era Japan, which was less a religious act than a social execution. His inheritance evaporated overnight. Those same missionaries would later send him to Princeton Theological Seminary, where he studied the mechanisms of poverty with the precision his contemporaries reserved for the mechanisms of profit.
On that Christmas Eve, before Princeton, before the degrees and the movements, Kagawa did something no seminary could teach. He walked into the slum and gave away everything he had. First, his clothing. Then his food. Then his money. He took in a beggar with trachoma, a bacterial infection that scars the cornea into opacity, and contracted it himself. His vision began to fail.
From that tiny room, blind in one eye and sleeping on bare floors, he built a movement. Organized the first major labour strike in Kobe's shipyards. Launched cooperatives that became the foundation of Japan's cooperative economy. Organized earthquake relief. Won universal suffrage. Founded the Japanese Federation of Labour. Wrote over 150 books. Was imprisoned. Went back to the slums. Was threatened. Kept preaching. Publicly apologized to China for Japan's occupation and was arrested again.
Arthur Miller, hearing him speak at the University of Michigan in 1935, called him a merchant of the sublime.
By 1920, Kagawa was functionally blind in one eye, lungs scarred by tuberculosis, and malnourished to the point of organ failure. He was 32 with the body of a man in his sixties. And he was more productive than he had ever been.
V. The Dissolution
I would not leave anything to a man of action as he would be tempted to give up work; on the other hand, I would like to help dreamers as they find it difficult to get on in life.
Alfred Nobel
In cellular biology, metabolic syndrome is a constellation of pathologies that emerge not from scarcity but from excess. The cell is flooded with more energy than it can process. The system starves in the presence of abundance. It does not lack fuel. It lacks the capacity to convert fuel into function.
Nobel had more fuel than any man in Europe. 355 patents. Factories on five continents. And no destination for any of it. A full tank and an empty map.
Tolstoy had fuel and he had the engine. 4,000 acres, 13 children, the most celebrated mind in Russian literature. What he did not have, what drove him to hide a rope behind the bookshelves, was any reason to keep driving.
Kagawa had a destination so clear it burned like a fixed star. He had no fuel at all. No inheritance, no health, no institutional power. And he moved faster than either of them.
In cellular biology, apoptosis is programmed cell death: a cell, having received a signal that it has become dangerous to the organism, dismantles itself. It does not explode. It folds its membranes inward, packages its contents, and delivers them to neighbouring cells. A cell that recognizes it must die so the organism can live.
Nobel read his obituary and began his apoptosis. Over eight years, he restructured everything. When he died in 1896, his will directed ninety-four percent of his fortune to five annual prizes for those who confer the greatest benefit on humankind. His family fought it viciously. It took five years before the first prizes were awarded. The five Nobel Prizes, each granting a million dollars to its winner.
And the prize he created would, 58 years later, be offered 5 times to a half-blind Japanese preacher who had given away everything he owned, and who didn't need it, because he had found a wealth the prize could not confer. Kagawa was nominated twice for Literature, three times for the Peace Prize. He never won. The institution could measure dynamite. It could measure literary technique. What it could not measure was what Kagawa was running on.
In entomology, when a caterpillar enters a cocoon, it does not improve. It dissolves. The cellular structure liquefies completely, every familiar form destroyed, and from that dissolution something emerges that bears no resemblance to what entered. The remarkable butterfly. From crawling to flying.
Nobel dissolved. 94% of everything he had, converted into a perpetual engine of human aspiration that has been running for over a century.
Tolstoy dissolved. His copyrights, his estate, his reputation. His ideas travelled from a Russian study to South Africa to Montgomery, Alabama, a chain reaction of moral force that has not yet spent itself.
Kagawa dissolved. His health, his sight, his inheritance, his safety. His cooperatives still operate. His theology still hums through churches on five continents, invisible as music, but positive as sound.
Each gave everything. Each created a wealth the visible world cannot measure, because what they gave was not to the present but to future generations, to people not yet born, to societies not yet built. A transfer of energy across the barrier of death itself.
VI. The Climb
For man to be able to live he must either not see the infinite, or have such an explanation of the meaning of life as will connect the finite with the infinite.
Leo Tolstoy
I think about Kagawa on long climbs. There is a point on the mountains north of Vancouver, about an hour in, where the grade tilts past 20% and the body begins to negotiate with the mind. The legs say stop. The lungs say stop. Everything measurable says stop. And occasionally something else says keep going, and the something else is not cardiovascular fitness or glycogen reserves. It is something the power meter cannot register, and I have never been able to name it precisely, except to say that it feels like the reason I am riding.
Kagawa lived there permanently. His entire existence was the last kilometer of a climb that never ends. The optimization industry would look at his biomarkers and call him a failure. He was also more alive than anyone in the room.
I think about my father pressing the clothing of strangers, 7 days a week, for decades. I think about the borrowed $100 that became 300,000 domains. My father was building a vehicle for his children. I was building a vehicle for my health dreams. Nobel was building a vehicle for his genius. Tolstoy was building a vehicle for Russian literature. Each of us building, building, building. And Kagawa, who had no vehicle at all, who had given away even the wheels, was the one who arrived.
The question I keep returning to is the one Nobel faced in a hotel suite, Tolstoy faced behind the bookshelves, and Kagawa faced on a hand cart on Christmas Eve.
It is not how much you have accumulated. It is not whether the vehicle is strong enough, though you should maintain it with the seriousness of a man who has read his own imaging and knows what the endothelium can do when you stop paying attention.
The question is what you are willing to give, all of it, every last molecule, to the generations who will come after you.
Nobel answered with his will. Tolstoy answered with his ideas. Kagawa answered with his life.
I have a company to build and a book to write and a documentary to make with my daughter and thousands more kilometers to ride this year. And I have, somewhere in the architecture of my days, a destination I am still trying to make worthy of everything I have been given, and everything my father gave so that I could be here to give it away.
VI. What Will Profit Me?
What would it profit a man if he gains the whole world but loses his soul?
Jesus
That question is over 2,000 years old. It has never been more urgent than now, in an era that has perfected the science of gaining the world and forgotten entirely what the soul requires.
The wealth that stays inside you is not wealth. It is a pathology. The wealth that pours out of you, that you release until the caterpillar has dissolved completely and something unrecognizable emerges from the cocoon: that is the only wealth that compounds across centuries.
And it does not matter how much or how little you have. Start giving it away.
If you have physical wealth, the vitality in your body, pour it into service. Show up. Carry what others cannot. Use your hands, your hours, the sheer stubborn fact of your presence to lighten the weight on someone who is breaking.
If you have financial wealth, redirect it. Not from surplus. From the center. Fund what outlasts you. Build for people you will never meet.
If you have intellectual wealth, the clarity of your mind, give it freely. Teach what you know. Write it down. Make the complex simple for those who come after you, the way Tolstoy spent fifteen years compiling wisdom for millions of people he would never see.
If you have emotional wealth, the resilience, the grit, the steadiness that holds when everything shakes, offer it to those who have none. Sit with the broken. Absorb the shock. Be the wall that does not move.
And if you have spiritual wealth, the faith that the invisible is more real than the visible, transmit it. Across generations. Across death itself. The way Kagawa transmitted it from a six-mat room in a slum the world had abandoned, blind, starving, and more alive than anyone in the room.
Nobel answered with his will. Tolstoy answered with his ideas. Kagawa answered with his life. My father answered with a borrowed $100 and 55 years of pressing the clothing of strangers so that his children could stand where he could not.
The question is not what you have. The question is what you are willing to give. And the giving will feel, against every instinct the visible world has trained into you, like the first moment you have ever been fully alive.
Save a Loved One
Forward my newsletter and YouTube channel to your friends and family.
122 million Americans have high blood pressure. 1.3 billion worldwide. Most don't know. Many are your loved ones.
You may be able to help save someone's life with knowledge alone. It could be your father, your spouse, your best friend. It could have been my friend Rob who wasn’t aware and suddenly died. It could have been me. That’s why I started my Youtube channel, for you and your loved ones.
You'll find these articles essential reading:
In Wealth
In Health
Reversing High Blood Pressure in 2 Weeks! — How I reversed a 71-year-old diabetic's high blood pressure so quickly
Reversing Diabetes in a Month! — How I reversed a 71-year-old's diabetes so quickly
The Diabetes Reversal Flywheel — Emptying the liver to live fully
Life-Changing Question
What do you do when you have accomplished your dreams of wealth?
Dr. Kevin Ham
First acquire all the five forms of wealth above with the goal of compounding it for your next generation and give it all away to them.
Next issue:
An Essay on Compounding Wealth
Subscribe to my Compounding Wisdom newsletter and start transforming your life. ham.com
Subscribe to my YouTube channel @DrKevinHam for videos on how I reversed my clogged arteries in 3 months, the top foods that clear your arteries, and the first principles of health that can save your life. Like, share and subscribe — it could save the life of someone you love.
Reversing High Blood Pressure in a Week
What most doctors don’t know about high blood pressure.
What most doctors don’t know.
The Life-Changing Text Message
Healing is a matter of time, but it is sometimes also a matter of opportunity.
Hippocrates
It was a Sunday afternoon, December 7, 2025, when my phone buzzed. Kim, a 41-year-old male friend, was in Vancouver on business and wanted to catch up. I said, let's have dinner at 123Dough.
Kim was on his way back from Korea and Japan, en route to Toronto. While in Korea, he had a full-body exam, the kind of thorough checkup Koreans routinely get for just $1500. His sisters said it was a good opportunity to get one done and get a baseline. He otherwise looked and felt fine. Completely asymptomatic.
Over dinner, he told me the story that changed his life.
The morning after his exam, at 7:30 am, the Korean doctor called him. Urgently. The doctor was shocked that Kim hadn't already had a heart attack. He told Kim to see a physician immediately upon his return home.
His numbers:
HbA1c: 11.2% (diabetes is diagnosed at 6.5%. This is catastrophically high.)
Fasting blood glucose: over 11 mmol/L (200 mg/dL)
Blood pressure: 160/90 (considered stage 2 hypertension)
High cholesterol. High liver enzymes.
Slightly overweight with a growing abdomen.
I was shocked. I told Kim they must have gotten the blood tests mixed up. An HbA1c of 11.2 at 41? With zero symptoms? That's the kind of number you see in uncontrolled diabetics headed for dialysis, blindness, and amputation.
I said, "Let's go to the drug store right after dinner and get a continuous glucose monitor and verify."
To my surprise, his glucose was over 12 mmol/L and climbing. It was real.
Kim had been reading my newsletter for a year. He had read the science. He read the principles. But it was abstract. It didn’t feel applicable to him (yet). It was an interesting read, but it wasn't personal until now. That's the nature of the Grim Reapers. They wait until you're looking the other way, and then they tap you on the shoulder to either wake you up or invite you to go with them to the other side forever.
It is one thing to read about fire. It is another to get burned by it. The paradigm shifts only when the ground beneath your feet shakes.
Dr. Kevin Ham
I explained to Kim that I had three reversal protocols:
Pro (1 week): aggressive, rapid results
Medium (1 month): substantial but more sustainable
Easier (3 months): gradual, still powerful
Kim quickly chose Pro. He was highly motivated. His doctor in Korea had scared him straight. I told him Pro was based on my first principled thinking, as no one had yet chosen Pro. He would be my first client. I told him it would be hard. Suffer for a week, but results should come very quickly. Unlike anything any doctor or patient has seen. I was comfortable as he was still young, and I knew he had a strong mindset if supported. I suggested we set up a daily chatroom for him to post his daily glucose, weight, and blood pressure, and to note his feelings and symptoms.
The Pro protocol: a low-caloric, low-fat diet. One meal a day. On the 7th day, no meals. And if possible, a 2-3 day fast near the end of the week.
We drove straight to Whole Foods and bought everything he needed for his one daily meal:
Steel-cut oatmeal with chia seeds and ground flaxseed
Salad mix
Lentils and black beans
Natto (2-3 tablespoons)
Blueberries
Half a red grapefruit
50 ml pomegranate juice
Ginger/turmeric drinks
Spirulina
The protocol still included carbs, which is usually a no-no for diabetics, but our goal was specific and strategic: reduce his visceral fat rapidly and make room in his liver for glucose. His liver was so fatty and insulin-resistant that glucose had nowhere to go. It was backing up in his blood like a traffic jam. First, we had to clear the road. Then, we could consider a low-carb diet.
Kim was a pro, and he executed like one. He did a two-day fast in the middle of the week. He wore the glucose monitor and adjusted his meals when he noticed his glucose spiked with grapefruit. He low-carbed his diet himself. His visceral fat essentially melted. I estimated that over 50% visceral fat around his organs would be gone in a week, based on studies I have read.
In just five days:
Fasting glucose dropped from over 12 mmol/L to 5 mmol/L (216+ mg/dL → 90 mg/dL)
Blood pressure plummeted from 160/90 (stage 2 hypertension) to 110/70 (normal and healthy for adult males)
All this in five days. His post-meal glucose still spiked, but this was to be expected, as the insulin resistance hadn't fully resolved.
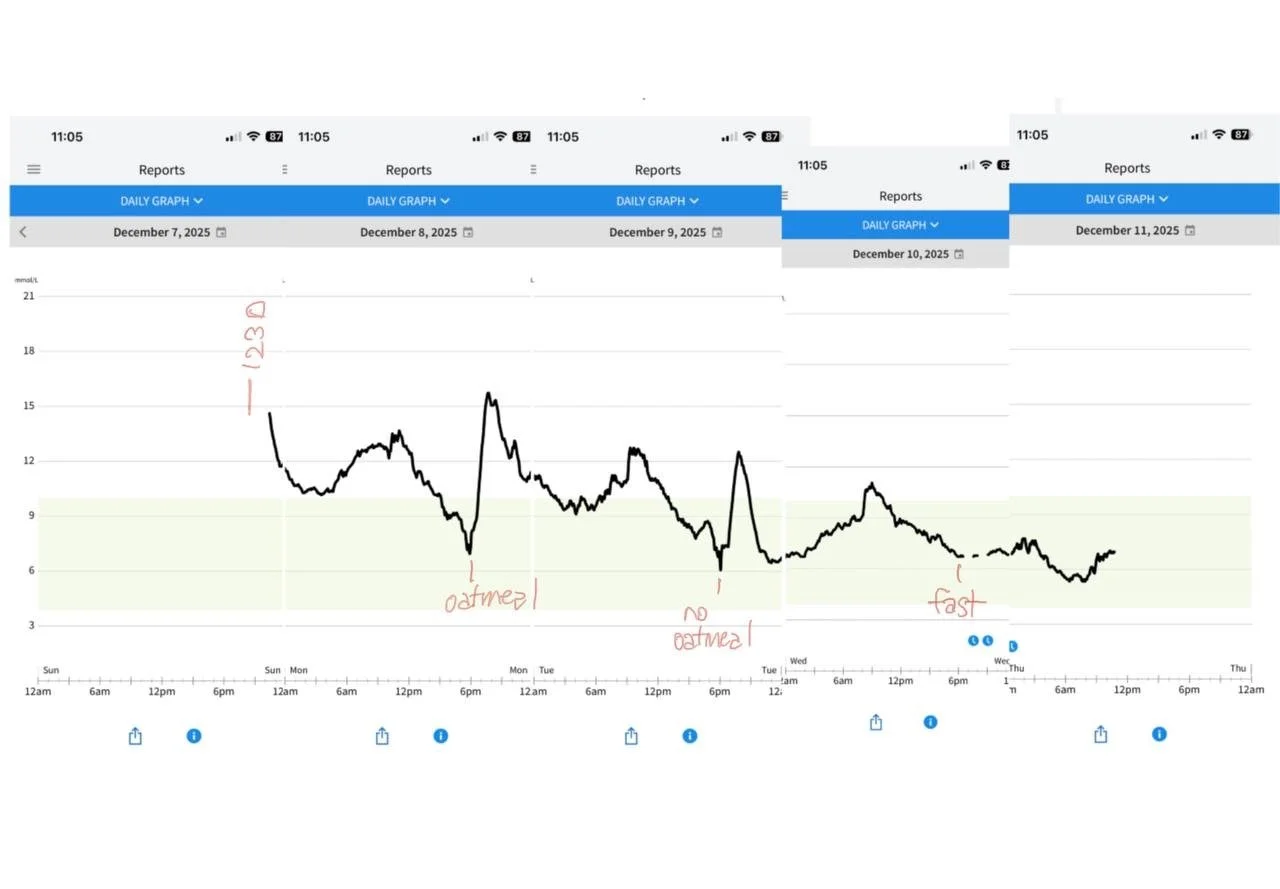
We transitioned him to the medium protocol for 30 days:
Weight: 144 lbs → 124 lbs (20 lbs lost)
Blood pressure: 105/70 (normal)
Fasting glucose: 4.5 mmol/L (81 mg/dL, perfectly normal)
Blood results: normal across the board
HbA1c: 11.2% → 7.8% in just 30 days
That HbA1c drop is extraordinary. HbA1c measures your average blood glucose over the past 3 months. To move it 3.4 points in one month means his blood sugar environment changed so drastically that even the 90-day average couldn't hide it.
His body was remembering what normal felt like.
Kim didn't take a single medication. No metformin. No insulin. No blood pressure pills. No statins. Just food. Just fasting. Following the protocol.
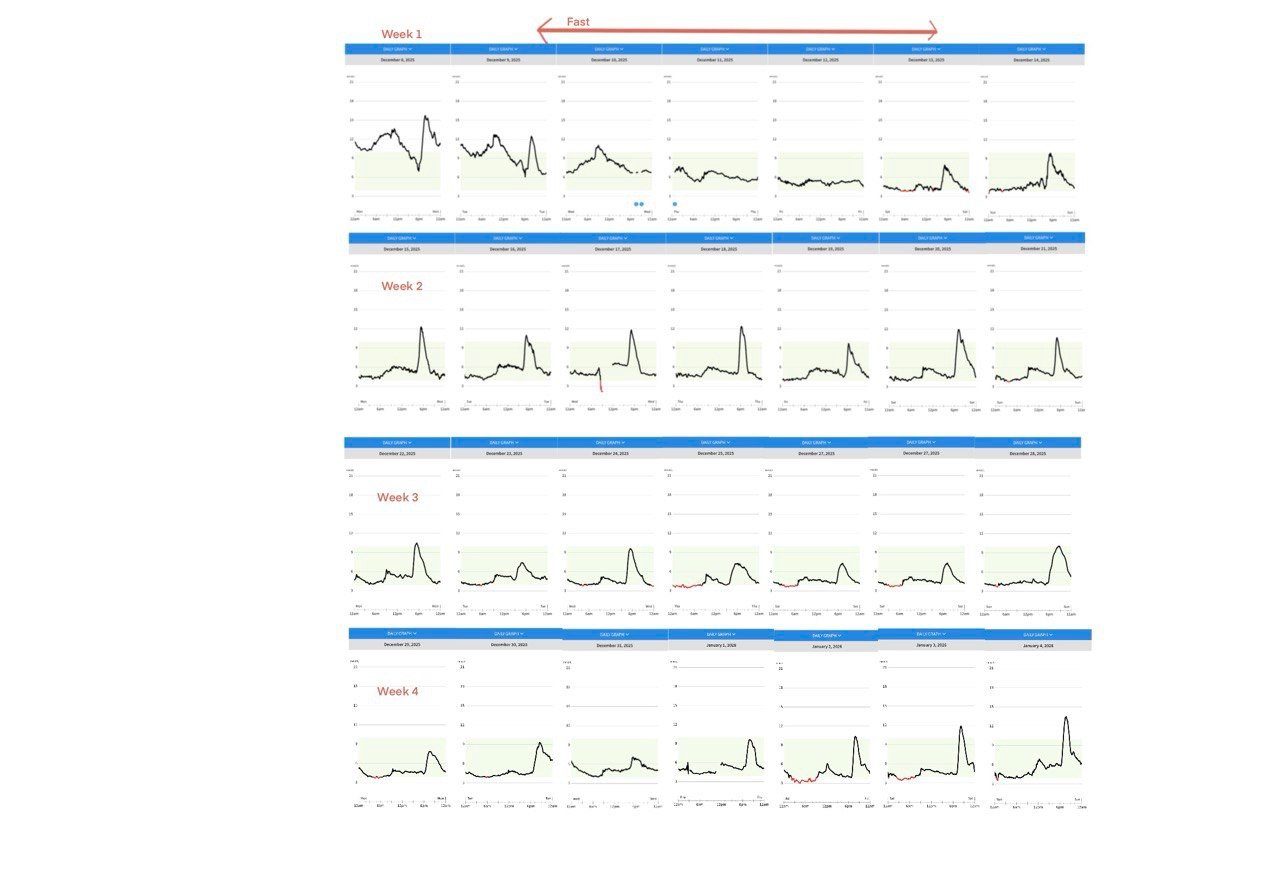
The body does not forget. It waits. It waits for you to stop poisoning it, and then it begins the work of repair with a speed that humbles the physician and stuns the patient.
Sir William Osler
I lost my dear friend Rob Thompson on February 10, 2025. He was 58. He was supposed to fly from San Francisco to Vancouver to visit me that very day. He died of a heart attack in the morning. I wasn’t able to help Rob. But Kim texted me that Sunday, and I believe that text message saved his life.
This newsletter is about one of the four Grim Reapers, high blood pressure, and the stunning, science-backed fact that it can be reversed in days to weeks without medications. Not managed. Reversed. Kim proved it. The studies prove it. And I want you to know it, so that when the Grim Reaper taps someone you love on the shoulder, you have the answer.
The Silent Invasion
Medicine is a science of uncertainty and an art of probability.
Sir William Osler
Nearly half of all American adults, 122 million people, have high blood pressure. Here are the numbers from the latest CDC data (NHANES 2021-2023):
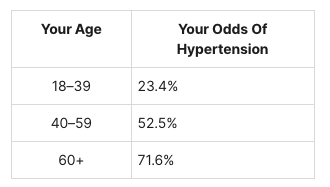
By your 60s, 7 out of 10 people you know have hypertension.
In Canada, it's 22.6%.
Worldwide, 1.3 billion people, doubled since 1990.
And yet, only 59% of Americans with hypertension even know they have it. Only 1 in 5 have it under control.
10.8 million people die every year from hypertension-related diseases. It is responsible for 54% of all strokes and 47% of all ischemic heart disease. A mere 2 mmHg reduction in population SBP would prevent 10% of stroke deaths globally.
But here is the statistic that should haunt every physician: 68% of all mortality attributed to high blood pressure occurs in people whose systolic pressure (the upper number) is between 120–140. This is the range most doctors call "borderline" and choose to “watch.”
Kim's blood pressure was 160/90. Rob's was probably in the "borderline" range. Watching is not enough.
What High Blood Pressure Does To You
The physician treats, but nature heals.
Hippocrates
Blood pressure doesn't hurt. That's the trap. It produces no symptoms until it has already done catastrophic damage. The WHO calls it the single most important risk factor for death worldwide. Kim felt perfectly fine at 160/90 with an HbA1c of 11.2. That's the terrifying part.
Your Heart: The muscle thickens to overcome the resistance. Then it stiffens. Then it fails. 69% of first heart attacks occur in people with BP above 140/90. Hypertension is the leading cause of heart failure.
Your Brain: A 20 mmHg increase in SBP doubles your risk of death from stroke. Chronic high pressure damages small cerebral vessels, causing white matter lesions and progressive cognitive decline. Midlife hypertension is now a recognized risk factor for Alzheimer's.
Your Kidneys: Hypertension is the #2 cause of kidney failure. High blood pressure damages the delicate glomerular capillaries, and the kidneys fail to excrete sodium, worsening hypertension. It’s a vicious cycle.
Your Eyes. Your Aorta. Your Limbs. Every vessel in your body takes the beating.
The body does not break all at once. It erodes. Like waves upon a cliff. Silent. Persistent. Until the cliff collapses.
Dr. Kevin Ham
The 5 Root Causes From First Principles
Le silence éternel de ces espaces infinis m'effraie. (The eternal silence of these infinite spaces frightens me.)
Blaise Pascal
Blood pressure does not rise randomly. It rises because something has gone wrong at a fundamental level. I found five root causes, each feeding the others in a vicious web:
1. Nitric Oxide Deficiency (Endothelial Dysfunction)
This is the master switch. The endothelium, the single-cell lining of every blood vessel, produces nitric oxide (NO), the molecule that relaxes and dilates your arteries. When NO is depleted, your arteries cannot dilate. Pressure rises.
Why does NO get depleted? Oxidative stress destroys it. The cofactor BH4 gets oxidized, and the very enzyme meant to produce NO (eNOS) starts producing harmful superoxide instead. A vicious cycle. The Western diet, high in salt, fat, and sugar, drives it. Lack of dietary nitrates (beetroot, leafy greens) starves the alternative NO pathway.
2. RAAS Overactivation
The Renin-Angiotensin-Aldosterone System is meant for emergencies: dehydration, blood loss. In essential hypertension, it's chronically stuck in overdrive. Angiotensin II constricts vessels. Aldosterone causes the kidneys to retain sodium and water. Insulin resistance activates RAAS, and RAAS worsens insulin resistance. The Western diet fuels the entire loop.
3. Sympathetic Overdrive : Cortisol and Stress
Chronic stress. Cortisol. Catecholamines. Your body is running a fight-or-flight system that never turns off. Cortisol suppresses nitric oxide production, triggers endothelin-1 (a powerful vasoconstrictor), and activates the RAAS. This has the single strongest association with essential hypertension of any mechanism.
4. Arterial Stiffness : The Thick Walls
Arteries are meant to be elastic. Years of high pressure, inflammation, oxidized LDL, and advanced glycation end products (AGEs) lead to collagen replacing elastin. Smooth muscle cells proliferate. The pipes become rigid. The heart pumps harder. Pressure rises further. Plaque narrows the lumen.
5. Renal Sodium Dysfunction
The kidneys are the final arbiter. ~50% of hypertensives are salt-sensitive. Genetic variants shift the pressure-natriuresis curve — meaning the kidney needs higher pressure to excrete the same amount of sodium. RAAS overactivation, insulin resistance, sympathetic overdrive, and gut microbiome disruption from high-salt diets all compound this.
The Yanomami people of the Amazon, who eat a traditional plant-based diet with minimal sodium, have ZERO age-related rise in blood pressure. An 80-year-old Yanomami has the blood pressure of a 20-year-old Westerner.
The age-related rise in blood pressure is not natural. It is the signature of the Western diet written on our arterial walls.
The Drugs
The person who takes medicine must recover twice, once from the disease and once from the medicine.
Sir William Osler
There are five classes of blood pressure drugs. They all lower the number. None of them fixes the cause. They lower blood pressure an average of −9.1/−5.5 mmHg at recommended doses. And 60% of medicated patients still have uncontrolled blood pressure.
Here's what each class does and what it doesn't:
ACE Inhibitors (Lisinopril, Ramipril) : Block the RAAS cascade. But: persistent cough in 15-20%, hyperkalemia, dangerous in pregnancy. Address only Root Cause #2.
ARBs (Losartan, Valsartan) : Block the angiotensin receptor. Better tolerated. But: still only address Root Cause #2. Your endothelium is still broken. Your arteries are still stiff.
Calcium Channel Blockers (Amlodipine) : Force arteries open by blocking calcium entry into smooth muscle cells. But: swollen ankles, headaches, gum overgrowth. They override the signaling rather than restore it. Address only Root Cause #4 — and only the functional component.
Thiazide Diuretics (Chlorthalidone, HCTZ) : Force kidneys to dump sodium and water. But: deplete potassium (dangerous), raise uric acid (gout), raise blood sugar (can trigger diabetes), increase cholesterol. Address only Root Cause #5.
Beta-Blockers (Metoprolol, Atenolol) : Chemically restrain the heart from beating too fast. But: a 2024 study of 97,639 patients found that beta-blockers as first-line caused MORE cardiac events than any other drug class. Fatigue, weight gain, depression, sexual dysfunction, and cold hands. Address only Root Cause #3.
Every drug addresses one root cause. The body has at least five. That's why the drugs fail in 60% of patients.
Dr. Kevin Ham
Reversal with Lifestyle
One of the first duties of the physician is to educate the masses not to take medicine.
Sir William Osler
Study 1: Water-Only Fasting: The Largest BP Reduction Ever Published
Dr. Alan Goldhamer, TrueNorth Health Center. 174 hypertensive patients. 10-11 days of medically supervised water-only fasting.
Average reduction: −37/−13 mmHg
Severe hypertensives (SBP >180): −60/−17 mmHg
89% normalized to below 140/90
100% discontinued all blood pressure medications
Compare: the average drug lowers BP by 9 mmHg. Fasting lowers it by 37. That's 4x the effect. No pills. No side effects. No refills.
Kim's result: 160/90 → 110/70 in 5 days. A 50/20 mmHg drop. Even greater than the study average.
Study 2: 1,610 Subjects: Buchinger Fasting (2020)
Published in the Journal of the American Heart Association. 10 days average. Hypertensives without meds: −16.7/−8.8 mmHg. Severe cases (>160/100): −24.7/−13.1 mmHg. Two-thirds of medicated patients reduced or stopped their drugs. JAHA Link
Study 3: NEWSTART Lifestyle: 14 Days
114 hypertensive subjects. Whole-food vegan diet + exercise + lifestyle coaching. SBP dropped −19 mmHg in two weeks. 40% achieved SBP below 120. 93% discontinued or decreased medications. Study Link
Study 4: McDougall Program: 7 Days
1,615 participants. Low-fat, starch-based, plant-based diet. Median SBP drop: −8 mmHg in 7 days — despite most antihypertensive medications being stopped at baseline. PMC Link
Study 5: DASH Diet: 2 Weeks
The gold standard dietary trial from the NEJM. Hypertensives: −11/−6 mmHg from diet alone. Effects begin within 2 weeks. No weight change required. Comparable to a typical antihypertensive drug. NEJM Link
Drugs vs. Food
The antifragile loves randomness and uncertainty... certain stressors and volatility make you stronger.
Nassim Nicholas Taleb
(fasting is that very stressor; it makes the body stronger)
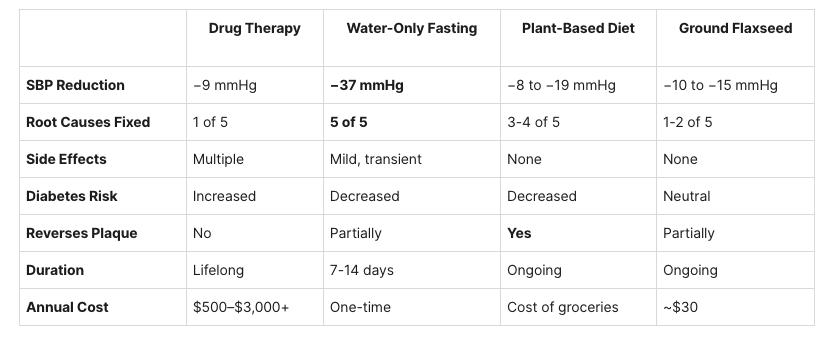
Top 10 Foods That Lower Blood Pressure
If we could give every individual the right amount of nourishment and exercise, not too little and not too much, we would have found the safest way to health.
Hippocrates
These are backed by clinical studies, not hearsay. Six of the ten were in Kim's daily meal:
1. Beetroot juice: Lowers BP within 2-6 hours. Nitrates → nitric oxide → vasodilation. Meta-analysis: −4 to −10 mmHg SBP. (PMC)
2. Ground flaxseed (30g/day): "One of the most potent antihypertensive effects achieved by a dietary intervention." Hypertensives: −15/−7 mmHg. RCT published in Hypertension. (AHA) ✓ Kim's daily meal
3. Hibiscus tea: Matched the drug Captopril in a head-to-head trial. −11% SBP / −12.5% DBP in 4 weeks. (PMC)
4. Leafy greens (spinach, arugula, kale): High in nitrates, potassium, magnesium, calcium. The same NO pathway as beetroot. ✓ Kim's daily salads
5. Pomegranate juice (50-150ml/day): 30% reduction in carotid artery wall thickness. Lowers SBP and DBP within 2 weeks. I drink 50ml daily. ✓ Kim's 50ml daily
6. Dark chocolate / cocoa (high flavanol): Increases NO bioavailability. 15 days → measurable BP reduction in hypertensives.
7. Garlic (aged extract): −5 to −8 mmHg SBP in hypertensives. ACE inhibition + hydrogen sulfide vasodilation.
8. Berries (blueberries, strawberries): Anthocyanins improve endothelial function. The highest intake is linked to the lowest hypertension risk. ✓ Kim's daily blueberries
9. Potassium-rich foods (sweet potatoes, white beans, bananas): Promote sodium excretion. −3 to −5 mmHg SBP. Counters the Western sodium overload. ✓ Kim's lentils and black beans
10. Seeds (pumpkin, chia, flax, hemp): Magnesium, potassium, L-arginine (NO precursor). Multi-pathway support. ✓ Kim's flax & chia seeds
Why Fasting Reverses All 5 Root Causes Simultaneously
Tout le malheur des hommes vient d'une seule chose, qui est de ne savoir pas demeurer en repos dans une chambre.
(All of humanity's problems stem from man's inability to sit quietly in a room alone.)
Blaise Pascal (quietly letting the body heal)
This is why fasting produces results 4 times greater than drugs. It doesn't target one pathway. It resets the entire system:
NO Restoration: Fasting reduces oxidative stress → eNOS recouples → NO production resumes → arteries relax
RAAS Reset: Zero sodium intake + reduced insulin → RAAS deactivates → sodium and water excretion normalizes
Sympathetic Downregulation: Parasympathetic activation → cortisol normalizes → heart rate drops → vasoconstriction eases
Vascular Relaxation: No dietary sodium, sugar, or saturated fat → endothelin-1 drops → functional stiffness resolves within days
Renal Recalibration: Kidneys excrete accumulated sodium freely → pressure-natriuresis relationship resets
It's like rebooting a computer that has been running for 40 years without a restart.
Dr. Kevin Ham
Kim's body rebooted in 5 days. His liver began emptying fat. His pancreas began recovering insulin function. His blood vessels relaxed. His kidneys began excreting the sodium they'd been hoarding. Every root cause began resolving simultaneously because we removed the cause, not just masked the symptom.
Save the Life of a Loved One and Friends
Forward my newsletter and YouTube channel to your friends and family.
122 million Americans have high blood pressure. 1.3 billion worldwide. Most don't know. Many are your loved ones.
Based on the data in this newsletter, you may be able to help save someone's life with knowledge alone. It could be your father, your spouse, or your best friend. It could have been Rob. It was Kim because he happened to text me on a Sunday.
You'll find these articles essential reading:
Reversing High Blood Pressure in 2 Weeks! — How I reversed a 71-year-old diabetic's high blood pressure so quickly
Reversing Diabetes in a Month! — How I reversed a 71-year-old's diabetes so quickly
The Diabetes Reversal Flywheel — Emptying the liver to live fully
Life-Changing Question
Before you heal someone, ask him if he's willing to give up the things that make him sick.
Hippocrates
What is your blood pressure right now? When was the last time you checked?
Don't wait for the Grim Reaper to reveal himself. Get a blood pressure cuff. Check it this week. If it's above 120/80, start making changes today — not next month, not next year. The studies show that even 7 days of the right diet can begin the reversal. Kim's showed results in 5.
If you are on medications, do not stop them without medical supervision. But know this: the science shows that with the right protocol, the majority of patients can reduce or eliminate their medications.
The body remembers what normal is. You just have to give it the chance to remember.
Next issue:
An Essay on Compounding Wealth
Subscribe to my Compounding Wisdom newsletter and start transforming your life. ham.com
Subscribe to my YouTube channel @DrKevinHam for videos on how I reversed my clogged arteries in 3 months, the top foods that clear your arteries, and the first principles of health that can save your life. Like, share and subscribe — it could save the life of someone you love.
The Architecture of Your Life
How your hands can guide you powerfully in life decisions.
How your hands can guide you powerfully in life decisions.
Three Life Threads Woven Together
Man is not destroyed by suffering; he is destroyed by suffering without meaning.
Viktor Frankl
As I wrote about Life, I have come to see life woven together from three threads:
Health
Wealth
Meaning
Health sustains us. It is our vehicle into the world.
Wealth drives us. It is the fuel to move throughout the world.
Meaning enlivens our spirit with purpose and inner drive.
Health can be measured by blood tests and exams.
Wealth can be counted in assets and valuations
Meaning resists measurement. It resides deep within you.
Meaning is immeasurable, unbounded and yet its absence is unmistakable.
Without meaning, health is life without a spirit.
Without meaning, wealth just becomes accumulation.
Without meaning, life is meaningless and being swayed by life’s storms.
Meaning is not a thought, it is the energy of your spirit, that must be honed as a discipline.
The Intelligence of the Body
The body is wiser than we are.
D.H. Lawrence
I am writing this at the end of another three-day fast.
When I discovered I had severe plaque in my heart arteries, it was shocking. I knew intuitively right away that I must adapt my diet to stop the progression of my disease. But I also felt that fasting and modifying my exercise would also be highly complementary to my diet. So I have fasted one day weekly and 2-3 days monthly. After doing this for six months, I’ve now decided to move my 3-day fast to quarterly and continue my OMAD (one meal a day) weekly.
The first day of the fast is habit breaking.
The second day is mentally hard to do but mental clarity starts.
The third day is physical weakness but strong mental clarity for me now.
When glucose is depleted, the body performs an ancient survival strategy. It turns inwards and starts converting fats into ketones, small fat molecules that can power all the healthy cells of the body. The cancerous cells which can only metabolize glucose suffer and the immune system starts to recycle the weakest cells and organelles like defective or old mitochondria. This is called autophagy, which means self-eating but really it is self-repair and optimization to survive a period of starvation. Growth hormone increases to preserve muscle so one can still be active. After five days, stem cells are activated.
The body preserves what is essential and eliminates what is weak and unnecessary. Diseased or weak cells.
The brain and heart uses ketones and the pathways are changed. The energy is efficient. Seizures cease after four days. This is the basis for the ketogenic diet for people with seizures. It is also the basis to weaken cancer cells.
If the body must eliminate to live, what must the soul eliminate to mean?
Forty Days of Elimination
Man shall not live by bread alone.
Matthew 4:4
As Moses went up Mount Sinai to receive the law, The Ten Commandments, he fasted for forty days and nights. He did this three times. The second time to receive the new set of Laws written on tablets of stone and also once more to pray on behalf of his nation that had broken one of the laws.
Elijah, one of the prophets also fasted for forty days when the King and Queen sought to kill him. This too at Mount Sinai, also called Horeb.
Jesus also fasted forty days in the wilderness before beginning His ministry.
Gandhi fasted 21 days in protest three times, each time having to stop his fast due to losing too much weight.
I struggle with just three days. And yet on the second and third day, hunger disappears, I no longer feel attached or dependent on food as my mind seeks to survive. Clarity fills me. Ideas, thoughts and emotions surface that were long dormant or buried.
I started to think deeply about my hands, my body, and numbers and I wrote a book in my heart and my mind. Iwould like to actually write it one day. I have a trilogy of books on meaning. I thought of a trilogy of books on health and also on wealth. I wrote out a high level plan of what they were and will start to put my thoughts … in my newsletter.
I hope it helps you in your life. Here goes.
The Anatomy of Power
Anatomy is Destiny.
Sigmund Freud
In 1543, a young anatomist named Andreas Vesalius stood in a candlelit theatre in Padua and began dismantling centuries of anatomical assumption. Until Vesalius, anatomy had been blindly inherited more than observed. Ancient authorities were copied by routine. Diagrams repeated. Hardly questioned as to veracity.
Vesalius questioned.
He dissected the human hand bone by bone. 27 bones. A choreography of tendons. Cables under tension that produced a symphony of coordinated moves of fingers and hands. A structure of astonishing precision. Our marvelous hands’ structure was breathtaking.
He traced two nerves in particular.
The median nerve governs the thumb, index and half of the middle fingers. It si the nerve of precision. It allows opposition, the thumb to touch the finger, a motion that separates us from most mammals. With it, we write, sculpt, draw and perform surgery. It is the architecture of execution. Power exemplified.
The ulnar nerve, running on the inside of your arm governs the ring, pinky and half of the third finger. Subtler. Less dominant. Yet when injured, grip weakens drastically. Power drains quietly. Coordination dissolves. It strengths and stabilizes. Precision and support.
The body is not random. It is paired and it is balanced.
In cardiology, plaque accumulates millimeter by millimeter. An LDL particle slips beneath the endothelial lining. Inflammation follows. Immune cells seek to contain it and start forming fatty streaks that turn into atheroma, which harden over time, atherosclerosis or calcified plaque. I have too much of this. From fried and heated oil foods.
There is no alarm until arteries are blocked 70% or more or when they are fragile and break off to clot the entire artery. Heart attack. Stroke.
Drift is anatomical.
And your conviction and dreams do not collapse overnight. It erodes by degrees like rock withering by the constant waves over a period of time. Discipline does not disappear dramatically. It loosens molecule by molecule.
Meaning dissolves the same way.
The body organizes strength in two hands. Most of us are right-hand dominant. The right hand signs contracts, lifts weights, builds, executes. It is the hand of power.
The left hand rests closer to the heart. Often less dominant. Harder to write and draw with. Yet necessary. When you tie your shoes, zip up. It stabilizes. It balances. It carries the covenant ring.
Power and proximity.
Execution and alignment.
It dawned on me, as I visualized my fingers in the quiet morning, woken up in the heat of a double layer of pajamas, as my hands and feet get cold when I fast, that the body is hidden wisdom and not merely functional but also instructional. A blueprint to use to design our life, our businesses, our products. Our varied organs organized to sustain and grow life.
Ten fingers. Mean Ten principles to live our lives by. By design, rather than by circumstance, blown by the wind.
The right hand demands training. Strength must be cultivated beore it is trusted. Without discipline, power corrodes and becomes toxic. With structure, conviction decays and disappears.
The left hand demands alignment. Integrity must stablize execution. Gratitude must temper ambition. Humility must steady strength.
Power without heart corrupts.
Heart without power is weak and stagnates.
The Right Hand: Power (Execution)
Power must be trained before it is trusted.
Dr. Kevin Ham
The right hand is: Execution. Discipline. Structure.
Thumb: Strength & Opposition
Symbol: Capability
The thumb makes grip possible. Without it, power collapses. It represents foundational strength and the ability to oppose resistance.
My principle here: Observe and seek truth deeply. Slow down enough to see early signals — in my body, business, relationships, and soul. Catch drift while it is still reversible.
Index Finger: Direction
Symbol: Truth and alignment of aim.
The pointing finger sets trajectory. It determines where force is aimed.
Mine: Choose Truth Over Comfort. Do not negotiate with facts — medical, financial, relational, or spiritual. Face reality quickly. Correction early prevents catastrophe later.
Middle Finger: Backbone
Symbol: Discipline — the structural spine of execution.
The tallest and most central. It stabilizes grip and anchors force.
Mine: Practice Discipline as Reverence. Repetition builds strength. Train when I don’t feel like it. Fast when it’s inconvenient. Guard inputs. Small, daily obedience compounds into strength.
Ring Finger: Covenant
Symbol: Stewardship and responsibility.
Traditionally associated with commitment. It reminds us that power must serve something larger than self.
Mine: Steward, Don’t Possess. What you hold is entrusted. My body, influence, money, time, and intellect are entrusted. I am accountable for how I use them, not how I accumulate them.
Pinky: Stabilization
Symbol: Systems and small daily habits that preserve strength.
Small but essential for grip strength. Often unnoticed until weakened.
Mine: Build Systems That Protect Your Future Self. Structure carries me when willpower fades. Install structure while I’m strong, routines, guardrails, calendar discipline, so that fatigue or emotion cannot undo me.
Master these first. The right hand of power. Without power, intention weakens.
The Left Hand: Heart (Alignment)
Alignment protects what power creates.
Dr. Kevin Ham
The left hand is: Alignment. Humility. Wisdom.
Thumb: Integrity
Symbol: Core moral alignment.
Foundation of character. What you oppose defines you.
Mine: Live as If Heaven Is Watching. Hardest one for me. Make decisions as if God sees the motive, not just the outcome. Optimize for integrity, not applause.
Index Finger: Examination
Symbol: Self-audit and humility.
Turns inward before pointing outward.
Mine: Revise Without Ego. Examine myself quarterly. Tighten what drifts. Admit error quickly. Growth requires correction.
Middle Finger: Perspective
Symbol: Gratitude and balance.
Central stabilizer in times of stress.
Mine: Give Thanks in Gain and Crisis. Crisis carries both Danger & Opportunity. The Chinese character for crisis is made of two characters: Danger & Opportunity. When something good happens, give thanks. When something hard happens, look for refinement.
Ring Finger: Commitment to the Vital Few
Symbol: Protecting what truly multiplies.
Long-term bonds and focus.
Mine: Guard the Vital Few. Small inputs compound. The fractal law. Nature repeats patterns at every scale — arteries, trees, oceans. Identify the 20% of habits, relationships, and decisions that shape 80% of my outcomes — and defend them ruthlessly.
Pinky: Dependence
Symbol: Wisdom through reliance beyond self.
Smallest digit. Essential support.
Mine: Ask, Seek, Knock for Wisdom, With Confidence. Wisdom is pursued. Do not trust intellect alone. Ask for wisdom before acting. Seek clarity before scaling. Dependence sharpens discernment.
Your turn, Your Hands
Providential Serendipity has five fingers to grab a hold of you and me. Just grab her hand and let her lead.
Dr. Kevin Ham
Look at your hands.
On the right, write five principles of power.
On the left, write five principles of heart.
Keep them short. Behavioral. Non-negotiable. Count them weekly.
See the Appendix below for your Ten Fingers Manifesto Worksheet
Master the right hand first. Then rotate to the left.
Power without heart corrodes. Heart without power stagnates.
Ten fingers. Ten decisions. Write yours. And live them. The hand was never merely mechanical.
It blesses. It builds. It heals. It is lifted in surrender.
Ten fingers. Ten daily decisions.
May my right hand build with courage.
May my left hand remain near the heart.
May both hands stay open before God.
I will not merely study the structure. I will live it.
P.S. If you write your ten principles, send them to me. I would genuinely love to see what governs your power and what guards your heart.
Expect and Attempt
Expect great things from God. Attempt great things for God.
William Carey
In 1792, William Carey stood before a modest gathering and spoke the sentence above that would echo across centuries and reverberate in my soul and spirit.
Expectation is faith. Attempt is stewardship.
Meaning is not contemplation alone, it is construction. The body removes damaged cells to survive. The soul must remove trivial pursuits to live.
Our ten fingers represent ten decisions based on ten principles to live, repeated daily in varying forms to various people and circumstances. Perhaps this is why it is Ten Commandments and not any other number.
You are already living by some set of principles. The question is whether you chose them.
One day these hands will tremble, weaken and rest. Before that day comes, let’s use them to live life with intention. Train the hand of power. Steady it with the hand of humility. Keep both open before God and man.
The anatomy was not accidental. It was for our instruction. The body teaches survival. The soul must learn to life.
Save the Life of a Loved One and Friends
Forward my newsletter and Youtube channel to your friends and family.
Based on statistics, you can help save many of your friends and family from today’s Grim Reapers, the top killer diseases.
You’ll find these articles insightful and helpful as well:
Life-Changing Question
What do your ten fingers tell you?
Fill out the worksheet below.
TEN FINGERS MANIFESTO WORKSHEET
Write five Power principles on your Right Hand and five Heart principles on your Left Hand. Each principle should be short, behavioral, and non-negotiable.
RIGHT HAND: POWER (Execution & Discipline)
1. Thumb (Strength & Awareness):
________________________________
2. Index (Direction & Truth):
________________________________
3. Middle (Backbone & Discipline):
________________________________
4. Ring (Covenant & Stewardship):
________________________________
5. Pinky (Stability & Systems):
________________________________
LEFT HAND: HEART (Alignment & Humility)
6. Thumb (Integrity & Character):
________________________________
7. Index (Self-Examination):
________________________________
8. Middle (Gratitude & Perspective):
________________________________
9. Ring (Vital Few & Commitment):
________________________________
10. Pinky (Dependence & Wisdom):
________________________________
Weekly Practice: Count them weekly. Master the Right Hand first. Then rotate into the Left Hand.
Annual Practice: Revise without ego
Next issue:
Reversing High Blood Pressure in a Week
What Most Doctors Don’t Know
Subscribe to my Compounding Wisdom newsletter and start transforming your life.
The Power of Asks
How asks can lead to life pivotal moments, all at once.
How asks can lead to life pivotal moments, all at once.
4 Small Actions
I dreamed a dream of a life where no disease prevailed, where no hearts ached, where life knew no bounds and the only sounds that echoed were the sounds of glory and praise for life forever and ever.
Dr. Kevin Ham
I often ask “Why?” Why did my friend have to die without notice last year, on February 10, 2025, when he was supposed to catch the early morning flight from San Fran to Vancouver and have lunch with me, celebrate life and enjoy one another’s vitality for life and to do more than what was expected or required of us.
Why? I asked God. Why did my new puppy find her way out of our yard and die? Why such seemingly unreasoning injustice?
I have surmised my own answers after pondering these heartbreaking moments that reverberate throughout my life. Its partner, Grief, following like a diminishing shadow but still ever-present, reminding me of moments we dreamed together, thinking we had much more time together, was suddenly and abruptly cut short.
Then I have many more moments when I ask, “Why not…?” to which answers abruptly emerge with reasons: Not enough time, not enough money, not enough talent, not enough resources, not enough knowledge, not enough focus, parade in rapid succession to lead me to another uneventful day, week and month, and the years pass.
Where did my 55 years go? Why could I not dream more, aspire more, be more, do more, of all that arises in my heart? The chasm between my heart and my actions was as far as the earth is from the sun.
Then a ray of light dawns in the crevices of my clogged arteries, to let light in, and I start to wonder and ponder, “What if I do this?” But the dreams in my heart lay paralyzed, until I have the thought to pray for wisdom and ask, “Lord, grant me wisdom and lead my heart and my hands and feet. Let me ask for wisdom, which comes to all those who ask for Her presence and her many gifts, liberally, without reproach.” I consider this like a law of the universe, having discovered its magical powers in the book of James.
Then I ask, dare I ask, in a quiet whisper that moves from my heart to my hands, to my fingers, to my feet, to ask something that has sprouted within my heart.
I have also discovered another law of the universe, espoused by the Carpenter,
“Ask, and you shall receive. Seek, and you shall find. Knock, and it shall be opened to you.” People overlook or misunderstand this wise law, believing it to be merely a pleasant aphorism. Yet it is a cascading, powerful set of laws that move from thought to discovery to focused action.
Baseball is the sports version of Homer’s Odyssey. The first battle is to adventure from home. The last battle is to return home. This epic repeats over 9 innings. For each of your home runs, there are 3 bases and home. If you do not enter home, you are left stranded on one of the bases of life.
Ask (1st base) Most people remain waiting after “Asking,” impatient to receive the actions one must do to proceed to the next step.
Seek. (2nd base) Very few find because they grow weary of seeking.
Knock (3rd base) Those who stand at the door, knock timidly a few times then, depart before it opens. The door to their dreams remains closed, growing more downtrodden with each shrinking attempt.
Enter (Home base). When the door opens, you must enter prudently but quickly before it shuts.
When you hear stories of success, the preceding battles of unanswered requests, fruitless searches, and endless slammed doors are often told as fleeting footnotes. However, they are the necessary exercises that build resilience and sprout the roots of a determined will, nourished by tears and newfound insights as each ray of light gets hungrily swallowed by rejection and failure.
Then, there comes a time when one receives the precious insight that:
While one must ask for help, one must embrace Faith.
While one may seek to find, one must marry Hope.
While one may incessantly knock on doors, one must embody Love.
Oh My Dear Heart
Wisdom has many daughters. I have embraced three of them. Their names are Faith, Hope and Love.
Dr. Kevin Ham
Do the physical plaques obstructing the blood flow in my arteries and physical heart mirror the obstructions in my emotional and spiritual heart?
What is obstructing the love arising in my heart?
My mind calculates and reasons. With much veracity and logic, I consider my next set of actions, having asked, sought and knocked, with doors opening but my mind shutting them suddenly as it doesn’t make financial sense or is too big a commitment to step into that path, or too scary with too many unknowns, too many uncertainties. Excuses flood in to obstruct this sudden marvel at the door finally opening. I grab ahold of the handle and start to shut the door myself, turning my back on opportunity.
How many doors have I shut myself or not stepped through to embrace this new path?
I decided that I will trust. I will step into that room when the door I asked for opens. How many are able to get to this moment? I recollect all the potentially pivotal moments that passed me by. I have had the courage to step through many doors, but many more I was afraid to step through. Had I trusted and obeyed, how different might my life be?
But I have no regrets. These are lessons, and I can start anew. I can start now… again.
The Wisdom of Ants
Four things on earth are small, but they are exceedingly wise: the ants are a people not strong, yet they provide their food in the summer.
Proverbs 30:24-25
I decided to be the title sponsor this year for the Nearness of You cancer charity concert fundraiser, in honour of the late Grammy-award-winning saxophonist Michael Brecker. It is produced by Michael’s late wife, Susan Brecker, with proceeds supporting cancer research at Columbia University Medical Center, specifically the work of my dear friends, Dr. Azra Raza and Dr. Siddhartha Mukherjee. My heart said, “Yes, go for it!” But my mind screamed, “But you have no time, and why not use this for your own dreams?” I battled this great war between my heart and my mind. And, this time, my heart prevailed. I intuited that this path would open the doors of my heart and many other doors… quite quickly.
We booked our flights for a week from February 4th to 11th, and oh, what a journey it was.
We arrived at Azra’s temporary place, the Mamdani’s residence. Azra had just sold her home, and she was “squatting” at her friends’ place. She wanted us to stay with her. The Mamdanis were travelling, and their son, the new mayor of NYC, had moved into his official residence at Gracie Mansion, so I would occupy his room. Wow, that was surreal. As we stepped into the living room, we were introduced to another guest. It was supposed to be just us having dinner with just Azra, but this intriguing guest, who had just flown in from Portland and was supposed to meet Azra an hour before we arrived, had taken a nap that went unheeded, and arrived just 5 minutes before us. Azra asked if he could join us for dinner. Of course, we said yes.
His name was Ryan, and he was the genius who built the majestic ant colony at the American Museum of Natural History. We had just visited in December. It was amazing to see the leaf-cutter ants carry leaves 20x their weight. Ryan likened it to us carrying a 7-foot plank around for miles on end. He told us about how he brought the queen ant from a farm in Africa all the way to NY to make it her home. He described the many types of ants and their species, including a fascinating story about slave ants.
I had always marvelled at the instructions in Proverbs (6:6 and 30:24) to consider the wisdom and ways of the ants. “Consider her ways and be wise”. When I asked him about these two proverbs, he explained them to me very vividly. I had been asking God for such wisdom. Ryan offered to give us a private tour of the ants at the museum with his friend Matthew. What a privilege it was to receive even more wisdom from them. Serendipity is what Azra and I both remarked—that Ryan slept in and missed his date with Azra, so we could meet.
On our tour, we learned that another fellow ant lover is a famous actress whom Azra would love to meet one day. I believe their shared love of ants and the power of serendipity will one day connect and bind them. Who would have known there were so many ant lovers?!
The Heart Surgeons: Fragile Arteries
Do you see a man skillful in his work? He will stand before kings; he will not stand before obscure men.
Proverbs 22:29
The day of my flight, Azra asked me to call her. I wonder why? She asked if I would like to meet the head of cardiac surgery, but we would need to leave at 8 am. That would be 5 am PST. I said, “Yes!” Azra’s older brother was also a cardiac surgeon at Columbia University.
When I discovered I had major arterial plaques last year, I asked Azra to ask her brother, “Can plaques be reversed?” A simple “No.” “Has he ever seen any possibility?” Another “No.” But I was convinced otherwise because Dr. Esselstyn was also a cardiac surgeon, and his methods and dietary protocol showed otherwise. He had published studies in major medical journals and had written the book, “Preventing and Reversing Heart Disease.” I wondered why so few present-day doctors knew of him, even though he worked at the esteemed Cleveland Clinic.
A deep bow of respect to all doctors for their sacrifices and their hearts for helping people.
Hearing the history of cardiac surgery, surgical residents answering hard questions reminded me of my days as a resident doctor. When I saw the beating heart and the tiny 1.2-6 mm coronary vessels, it dawned on me how little plaque, just a few mm to half a cm, could end someone’s life suddenly. The fragility of life.
I showed Azra’s brother, the cardiac surgeon, the scans showing that I had reversed the plaque in my carotid arteries in just 3 months. He asked how I did it. Diet. But suddenly Azra beckoned me to follow her, so I got up and left before I had the chance to explain exactly how I did it.
Here I was among the most accomplished cardiac surgeons in America. How did this happen? I wondered.
Providential Serendipity
The Invisible Hand plants my feet along a path that opens new worlds with one step. Step after step is a whole new world.
Dr. Kevin Ham
Providential Serendipity. These were the words that imprinted into my heart during my magical week in NY. I felt a guiding hand, which President Washington referred to as the Invisible Hand, leaving His fingerprints along the path of my feet.
Auction Dinner
Most of our paths cross unnoticed but once a while, lightning strikes to fertilize and electrify our hearts to one another.
Dr. Kevin Ham
Azra wanted us to attend a pre-concert dinner auction. As we arrived, I was introduced as ‘Kevin from Canada.’ After dinner, Azra spoke about her mission to cure cancer and how she was finally on the verge of achieving it with her Stentinel. I wholeheartedly believe in her and her vision, and I invested a significant amount to jump-start her seed round.
Then, we went around the room doing introductions. My turn. I told the group how I met Azra and, upon reading her book, “The First Cell”. I was so moved and inspired by her life mission that I had the thought to ask her if she would like to write a book together on preventing cancer. She said to call her and said we should not only write a book together, but how about doing a documentary together, with Dr. Sid Mukherjee, Susan Brecker, the Nearness of You Concerts and the vision of curing cancer. I stepped through that door. In 2024, I arranged for Chris Froome, 4x Tour de France winner to come to Vancouver to lead a charity bikeathon for Azra. So Chris stayed at my place, and about 80 of us rode together with him. Can you imagine? Chris gave me one of his yellow TDF winning jerseys for my birthday the day after. Wow.
The next person said they were one of Azra’s patients in her book. Donna. For 30 years, Azra has been her oncologist. She spoke about how Azra empowered her to make decisions and that she believes empathy and care for her are what have kept her alive. She has travelled from Chicago to New York every two weeks for blood transfusions for the last 18 years to be treated by Azra. We had briefly spoken while getting our food. We connected even then. But after hearing her story, I fell in love with her spirit. She is 88. Azra had mentioned her a few times. We spoke heart to heart afterwards, and I must have hugged her many times out of joy and care. We instantly became close friends. How quickly hearts connect. We met many other wonderful people. It was an inspiring evening.
Providential serendipity visited us yet again.
The Nearness of You Concert
No longer here, I see you everywhere, feel you everywhere, hear you whisper and shout, telling me to go on and not succumb to Grief but dress her up with Compassion and Purpose.
Dr. Kevin Ham
I had invited 16 guests to join me at the concert, dear friends, some of whom I had not seen in decades. It was held at the magnificent Lincoln Centre. Hugh Jackman would be speaking, and James Taylor would be singing. I was seated next to Hugh. I visualized what words I would speak to him if given the opportunity.
“I so wanted to meet your father after I heard you speak about him on a podcast with Tim Ferriss. He seemed like such a great man and had values that I cherish. A devout faith and an ever-encouraging father.”
“I also admire and honour how you held the first charity event for Azra and Sid in your home 16 years ago.”
“I love your movies, especially The Greatest Showman and Les Misérables. Musicals which make my heart sing.”
“I was a huge fan of X-Men and Wolverine growing up, especially of X-Men comic book issues #136-142, Days of Future Past.”
But besides me saying, “Hi, I’m Kevin Ham,” I wouldn't get that chance, as he had to leave for an emergency at home. He did say, “Hi Kevin!” And in those 15 minutes sitting beside him listening to the singers, I again thought, “Providential serendipity.”

Hugh Jackman and me :)
James Taylor came up to the stage and sang the theme song of the concert, Nearness of You. I don’t know what happened, but I suddenly felt the wells of my heart proceed out of my eyes. As each chord he struck drew up the buckets of my inner wellspring while he tenderly sang the lyrics for Michael Brecker, the Grammy award-winning jazz musician, who passed away from leukemia two decades prior but still sings to us through his saxophone in these charity concerts for the research of Dr. Azra Raza and Dr. Sid Mukherjee.
The song, in its raw, powerful authenticity, struck a deep chord in my soul. The echoing question reverberating throughout my entire being was, "Can I do more?" Am I living to my fullest and being bold enough to stand up to such a great monstrous disease, Cancer, yet with the humility to bow the knees of my heart in prayer for wisdom, for strength and courage, not only for myself, but for all those infected by this and for those it lies in wait.
The NY Academy of Science
Providential Serendipity has five fingers to grab a hold of you and me. Just grab her hand and let her lead.
Dr. Kevin Ham
I had invited Nick Dirks, the President and CEO of the New York Academy of Sciences, to the concert and briefly spoke with him that evening. He has the look of Einstein, but more distinguished. Azra had introduced my daughter and me to her good friend, as we were curious about music schools in NY, since we love Broadway. She invited her husband and their brilliant son, who teaches Paradise Lost, which is our book to read this year. We connected like lightning in those short two hours, talking about Darwin, AI, cycling, education, philosophy, Paradise Lost, health, music, movies, Broadway, and salsa dancing. That first meeting left a lasting impression.
We met Nick for an early dinner, just before our Hamilton show. We had just filmed part of the documentary with Sid, Susan, Azra and me with a sweet, resilient Broadway dancer fighting cancer. Sid dedicated a toast to two enlightened souls. Man is enlightened by virtue of two attributes: his ability to reason and his fight for emancipation (freedom). The highest level of emancipation is from disease, to be free of disease, and the “Emperor of All Maladies” (Sid’s Pulitzer Winning biography on cancer) is cancer, the concert held to raise awareness and solidarity to find the solutions to this devastating disease.
The Manhattan traffic moved like cars with flat tires. We were 30 minutes late. He graciously texted, ‘No hurry.’
We got out two blocks early from the Uber and started running.
We spoke about the concert. I told the story of how I met Azra. He told us his first meetings with Azra and later Sid. He then spoke about his work at the NY Academy of Science. The prizes they awarded in US, UK and Israel to promising aspiring scientists. $250,000 Blavnik Awards. I had not had the pleasure of meeting the Blavniks, though they were at the concert.
He suggested during our meal that I visit and that I would meet very interesting people and also fascinating projects. I, of course, was interested. He asked if I knew Reid Hoffman. I adored Reid as I often listened to his podcast, Masters of Scale. He founded Paypal and Linkedin. But I loved that he majored in Philosophy. Nick also did. I told Nick I wished I had studied Philosophy as well. Philo = Love. Sophia = Wisdom. The Love of Wisdom. I loved Wisdom, and I ask and seek her daily. I told him I would love to interview Reid one day. He said he would gladly introduce him to me. I was delighted.
As we finished our meal and took a last-minute photo, he quickly said he would love for me to be part of the Board of Governors of the NY Academy of Sciences. I was focused on capturing a photo of us, and his request only partially registered. As my wife and I sat eating dessert, I asked her if I had heard correctly that Nick was asking me to join the Board of Governors. I quickly looked at who was on the Board of Governors. He had mentioned the former President of Yale.
I thought I must have heard incorrectly. I texted Azra that I think Nick asked me to be on the Board. She was overjoyed and told me that the likes of Jefferson, Madison, Edison and Einstein were once members. That it would be a momentous opportunity. I texted Nick right before Hamilton started. ‘I thought you were asking if I’d like to be on the Board of Governors, but it didn’t register until later that that was what you were proposing.’
Hamilton had inspired me so much 8 years ago. Just after I had watched it, I told my wife that I would one day make my own inspiring musical. I wrote the first and second drafts years ago, but have been too busy to make the dream a reality.
I had momentary questions intrude upon the show. “Could it be?” “How?” “Why?” ‘What does this mean?”
I already had so many Providential Serendipities in these few days. I had intuited, when I decided to stay for a week, that many doors would open for me to step through. Each day was expressed in “It was the best of times.” It was the worst [coldest] of times.” It was the coldest Feb in NY. -25 degrees Celsius. But the weather would not freeze our warm, connected hearts and the warm embrace of the Providential Hand.
The next morning, Nick replied, ‘Yes, I was asking you to join the Board of Governors for the New York Academy! It would be a privilege to be able to work with you on exciting projects in areas of interest in science and technology.”
My life reads like a novel. Like a dream. I write to capture the feelings and thoughts of my heart. To remind myself to dream, to be heart, to have Faith, Hope and Love as my guides, following Providential Serendipity. In turn, inspire each of you to dream with Hope, to live with Faith, and to love Love.
Providential Serendipity. Reach out and grab hold of her hand.
Ask and receive. With Faith.
Seek and find. With Hope.
Knock and open. With Love.
My heart is overflowing with these three daughters of Wisdom.
My gratitude and love to:
The Mamdani’s, for allowing us to stay in their private residence.
Ryan, the real Antman, for his love of nature and ever cheerful wisdom.
Donna, the resilient architect with a heart of joy.
Dr. Raza, for opening his hands and his heart to me.
Sid, for enlightening our souls.
Susan, for her beautiful heart
Nick, for his endearing heart and visionary soul.
Azra, for her friendship and love.
The marriage of Providence and Serendipity
Save the Life of a Loved One and Friends
Forward my newsletter and Youtube channel to your friends and family.
Based on statistics, you can help save many of your friends and family from today’s Grim Reapers, the top killer diseases.
You’ll find these articles insightful and helpful as well:
Life-Changing Questions
What is your ask?
What do you seek?
What door shall you knock on?
Who or what shall open unto you?
Just write the first answers that enter your heart.
Grab ahold of Providential Serendipity’s hands and embrace Faith, Hope and Love with all your heart and soul.
Next issue:
Reversing High Blood Pressure in a Week
What Most Doctors Don’t Know
Subscribe to my Compounding Wisdom newsletter and start transforming your life.